
Abstract
Objectives:
To provide clinicians who treat multiple sclerosis (MS) patients with evidence-based or expert opinion–based recommendations for promoting exercise and lifestyle physical activity across disability levels.
Methods:
The National MS Society (“Society”) convened clinical and research experts in the fields of MS, exercise, rehabilitation, and physical activity to (1) reach consensus on optimal exercise and lifestyle physical activity recommendations for individuals with MS at disability levels 0–9.0 on the Expanded Disability Status Scale (EDSS) and (2) identify and address barriers/facilitators for participation.
Recommendations:
Based on current evidence and expert opinion, the Society makes the following recommendations, endorsed by the Consortium of Multiple Sclerosis Centers:
Healthcare providers should endorse and promote the benefits/safety of exercise and lifestyle physical activity for every person with MS.
Early evaluation by a physical or occupational therapist or exercise or sport scientist, experienced in MS (hereafter referred to as “specialists”), is recommended to establish an individualized exercise and/or lifestyle physical activity plan.
Taking into account comorbidities and symptom fluctuations, healthcare providers should encourage ⩾150 min/week of exercise and/or ⩾150 min/week of lifestyle physical activity.
Progress toward these targets should be gradual, based on the person’s abilities, preferences, and safety.
If disability increases and exercise/physical activity becomes more challenging, referrals to specialists are essential to ensure safe and appropriate prescriptions.
When physical mobility is very limited, exercise should be facilitated by a trained assistant.
Keywords
Introduction
Wellness is a priority for people with multiple sclerosis (MS) 1 and can be achieved through health behaviors including physical activity and exercise.2–4
Physical activity, including lifestyle physical activity and exercise, comprises any bodily movement produced by skeletal muscle contraction that results in a substantial increase in energy expenditure over resting levels. 5
Lifestyle physical activity is the daily accumulation of at least 30 minutes of activities, including all planned or unplanned leisure, occupational, or household activities that are at least moderate to vigorous in their intensity. 6
Exercise is a form of leisure-time physical activity that is usually performed repeatedly over an extended period of time (exercise training) with a specific external objective (e.g. improvement of fitness, physical performance, or health). 5
These activities are distinct from rehabilitation, which is defined as intermittent or ongoing use of interdisciplinary strategies to regain or maintain optimal physical function, promote functional independence, prevent complications, and improve overall quality of life. 7
Meta-analyses and systematic reviews of randomized controlled trials have demonstrated that people with MS who engage in exercise and lifestyle physical activity experience benefits from immune cell through quality-of-life outcomes.8,9 Furthermore, exercise and lifestyle physical activity are safe for people with MS. 10 While initial studies established exercise as an effective symptomatic treatment (tertiary prevention), more recent studies have evaluated the disease-modifying effects (secondary prevention) as well as the impact on the risk of developing MS (primary prevention)—explaining why exercise and physical activity have been suggested as “medicine in MS.” 11
Unfortunately, MS patients are much less active than healthy controls.12,13 One recent review by an international panel of experts highlighted the opportunity for neurologists, advanced practice clinicians, and primary care providers to promote exercise and physical activity in their patients, 9 and a recent study demonstrated that adherence to a physical activity program is higher when referral is made by a physician. 14 Yet, qualitative research indicates that many providers lack the expertise to do so. 15
This paper offers clinicians specific exercise and lifestyle physical activity recommendations—evidence-based when possible, and expert opinion where published data are lacking—for their patients at all levels of disability. The recommendations are tailored by disability level using the Kurtzke Expanded Disability Status Scale (EDSS)—a method of measuring neurologic disability in MS (see Figure 1 in Supplemental Appendix 1). 16 Levels 0–9.0 (ranging from no disability to confined to bed) are considered in this paper.
Recommendations for the intensity of exercise/physical activity are based in part on an individual’s perceived exertion level (subjective evaluation of intensity, effort, strain, discomfort, and/or fatigue during exercise). See Table 1a in Supplemental Appendix 1 for use of Borg’s Rating of Perceived Exertion (RPE).17,18
Methodology
The National MS Society convened international experts in the fields of MS, exercise, rehabilitation, and physical activity (physicians, nurses, physical therapists, occupational therapists, exercise scientists, community health professionals) to (1) review the literature and reach consensus on optimal exercise and lifestyle physical activity recommendations for individuals with MS across major categories of disability on the EDSS and (2) identify and address barriers and facilitators of participation. The group used published exercise and physical activity guidelines19,20 as the starting point, supplemented by additional high-quality studies and expert opinion, particularly at the higher disability levels where evidence has been lacking. Sub-teams were created for three EDSS ranges corresponding to MS with mild impairments (0–4.5), MS characterized by greater mobility impairment (5.0–6.5), and MS characterized by diminished ability to carry out activities of daily living (7.0–9.0)—which are consistent with ranges used in the literature 21 (see Figure 1 in Supplemental Appendix 1). Following a review of the recent literature, evidence-based and expert recommendations were created.
Exercise and lifestyle physical activity recommendations throughout the disease course
To assist clinicians who are unfamiliar with the EDSS, Table 1 provides clinical descriptors for each disability range. Tables 2 and 3 provide exercise and lifestyle physical activity recommendations, respectively, as well as key messages for individuals in those disability ranges. The recommendations reflect the minimum exercise and lifestyle physical activity targets for people with MS; however, each individual’s starting point and rate of progress toward a target will differ. As disability increases and mobility becomes more challenging, so does the importance of personalized recommendations and guidance by a trained rehabilitation or exercise professional. For that reason, the EDSS level 7.0–9.0 has been sub-divided to allow for more specific recommendations for individuals with the highest levels of disability.
Clinical descriptors for EDSS ranges 0–4.5, 5.0–6.5, and 7.0–9.0.
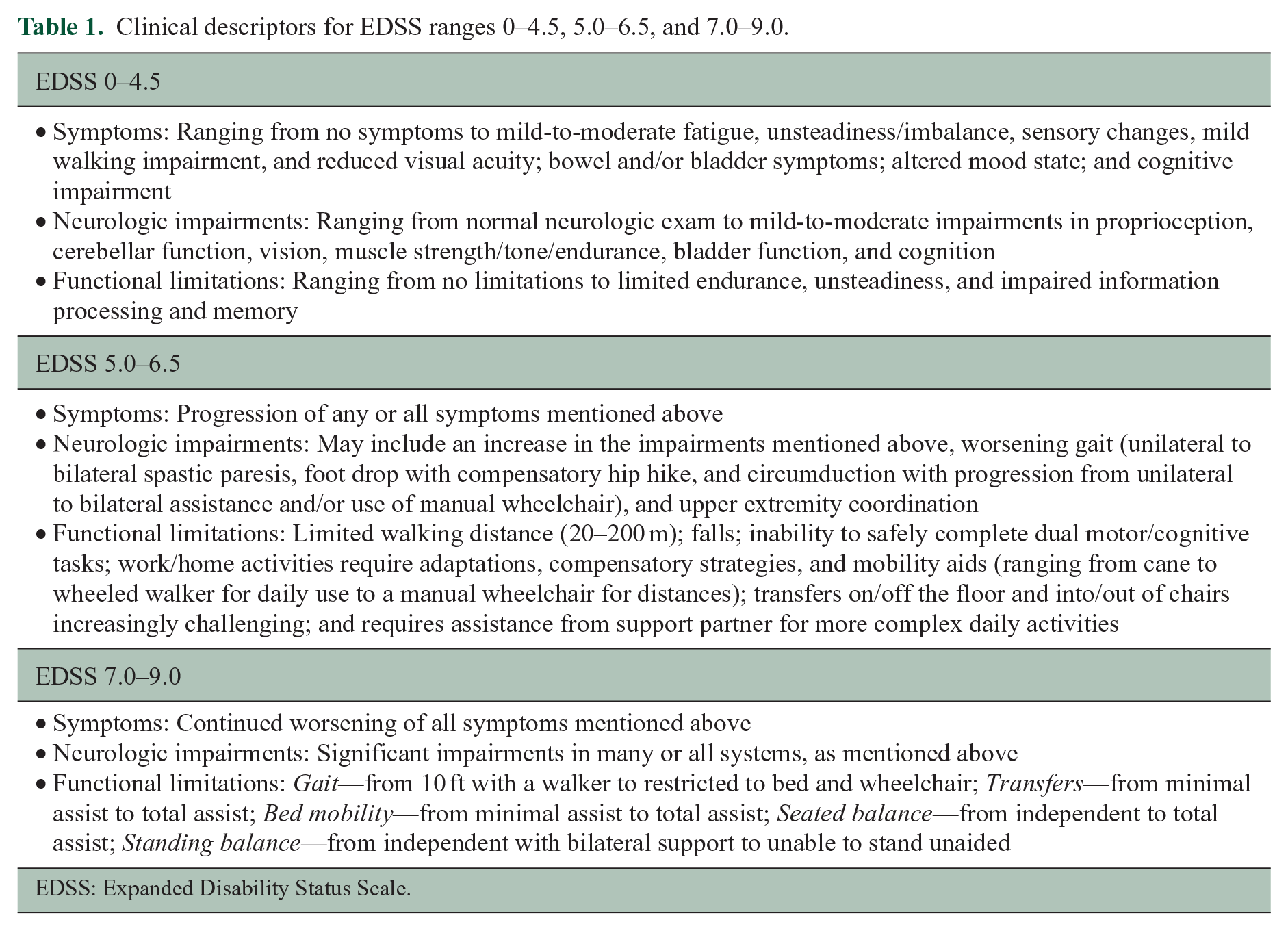
EDSS: Expanded Disability Status Scale.
Exercise recommendations and key messages for EDSS 0–9.0.
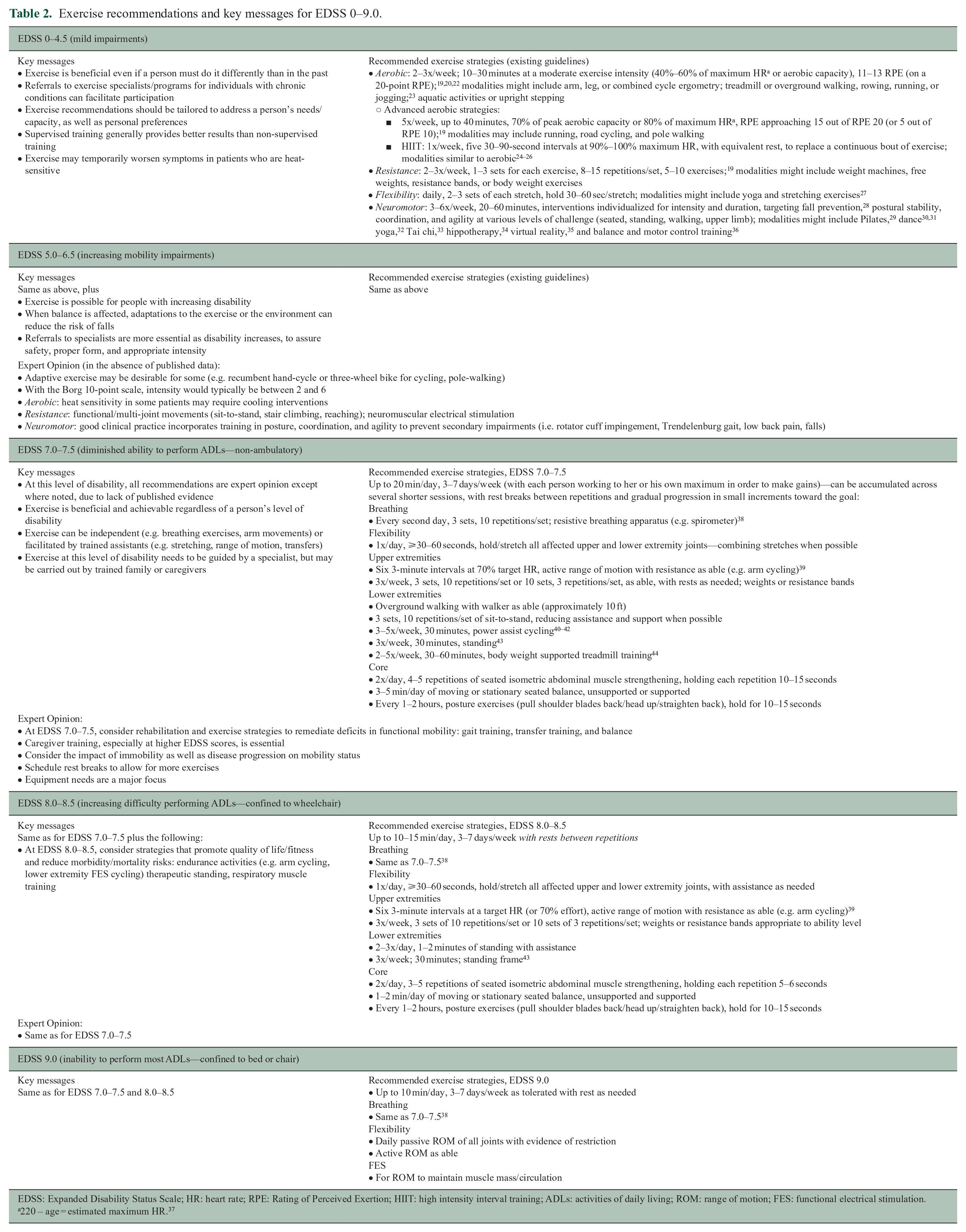
EDSS: Expanded Disability Status Scale; HR: heart rate; RPE: Rating of Perceived Exertion; HIIT: high intensity interval training; ADLs: activities of daily living; ROM: range of motion; FES: functional electrical stimulation.
220 – age = estimated maximum HR. 37
Lifestyle physical activity recommendations and key messages for EDSS 0–9.0.
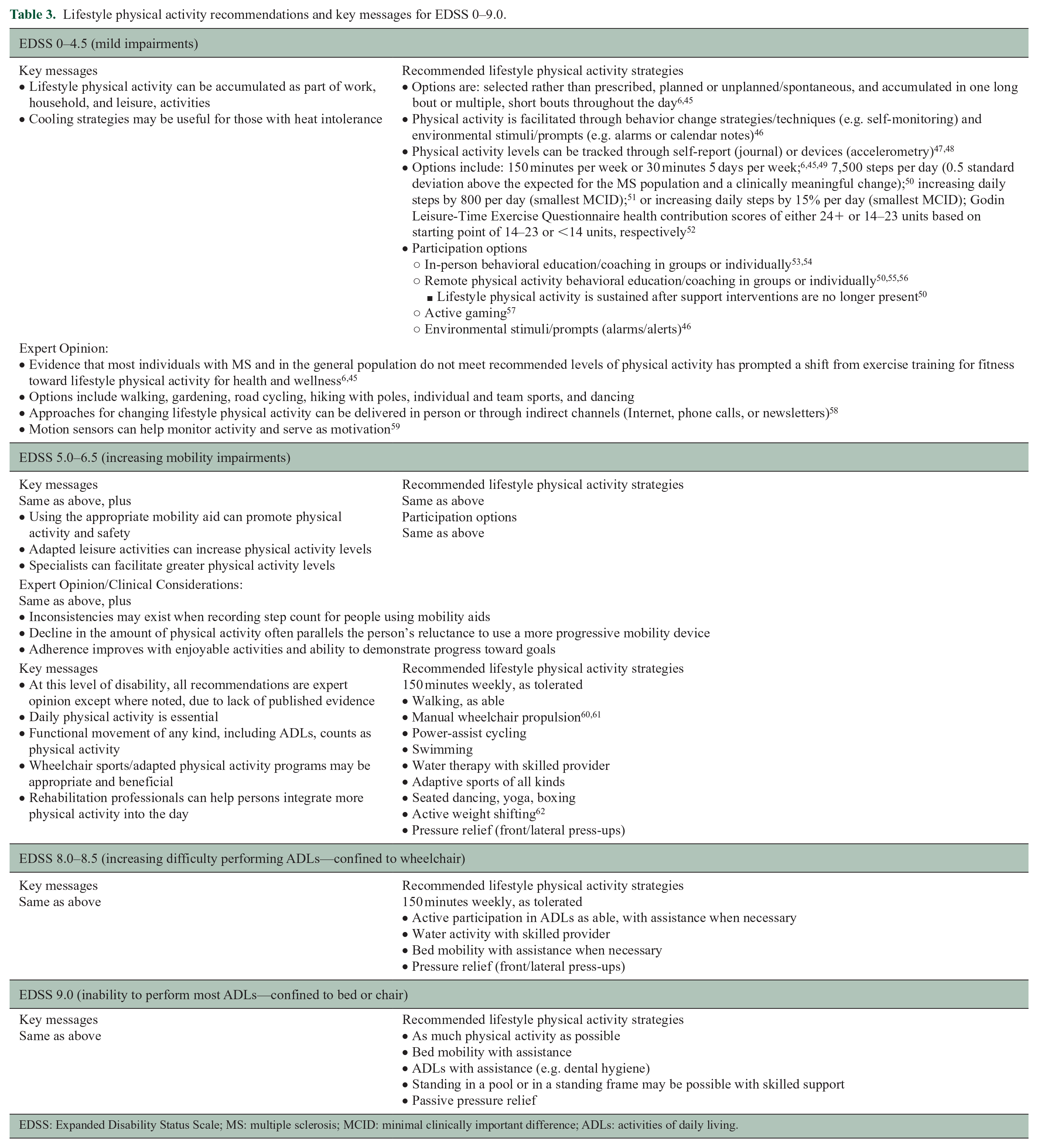
EDSS: Expanded Disability Status Scale; MS: multiple sclerosis; MCID: minimal clinically important difference; ADLs: activities of daily living.
Barriers and facilitators to exercise and lifestyle physical activity
Table 4 presents the types of barriers that may reduce a person’s ability to engage in exercise and lifestyle physical activity, as well as the facilitators that can increase a person’s ability to do so. 15
Barriers and facilitators to exercise and lifestyle physical activity.
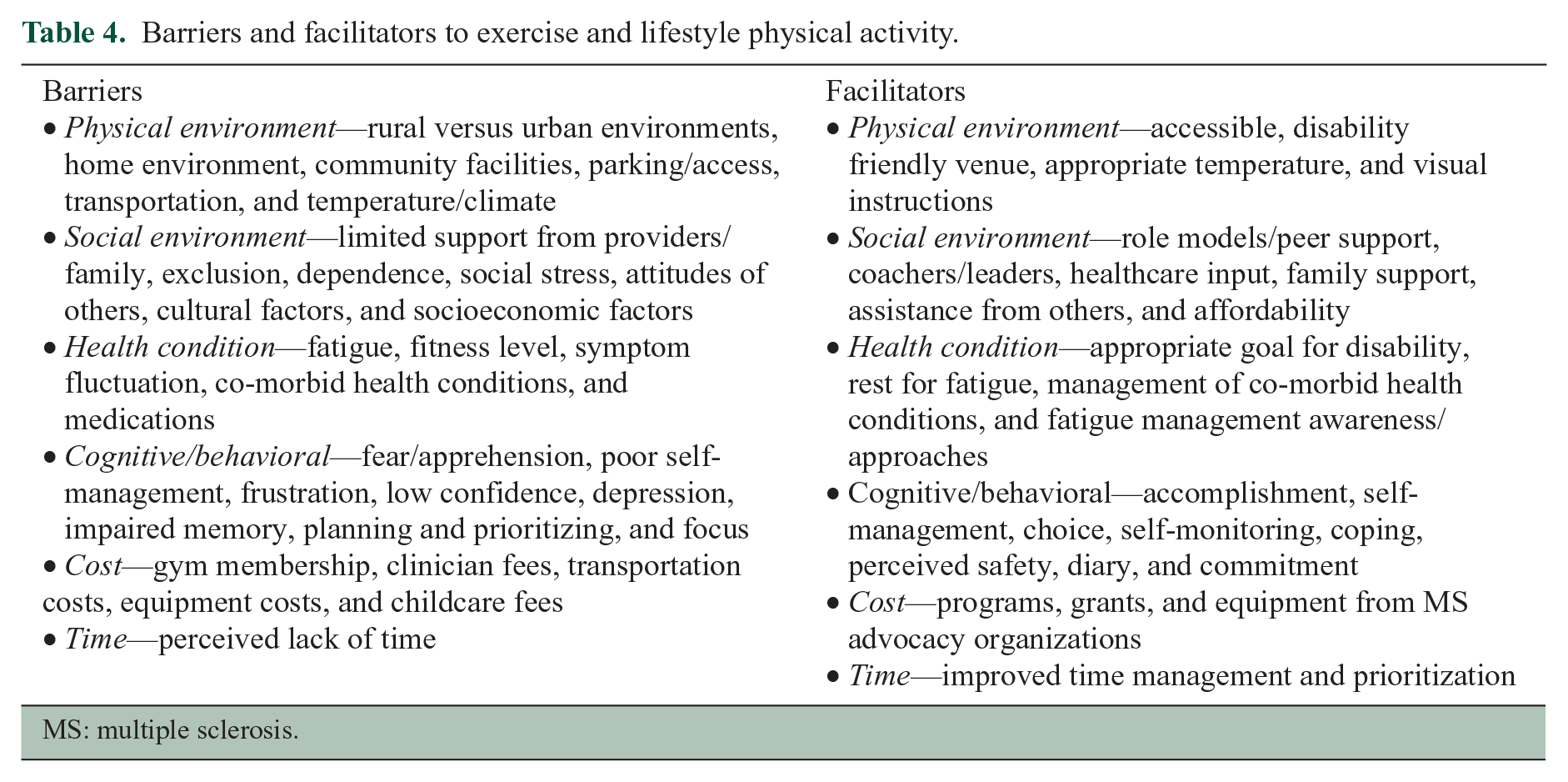
MS: multiple sclerosis.
Discussion
Despite ample evidence demonstrating the benefits of exercise and lifestyle physical activity for people with MS, MS patients continue to be substantially less active than their counterparts in the general population. Many people with MS doubt their ability to be physically active. Fatigue, mobility impairment, depression, fears about safety, reluctance to engage in activities they cannot do as easily or well as they did them before, and lack of access to appropriate venues are just a few possible reasons for their inactivity. Neurologists, advance practice clinicians, and other healthcare providers can be powerful advocates for exercise and physical activity, emphasizing the benefits for disease and symptom management, overall health, and quality of life, and assuring their patients that it will not worsen their MS. Healthcare providers are encouraged to 63
Ask routinely about a patient’s exercise and physical activity habits
Offer timely information about how and why to be physically active (benefits and expected outcomes) as well as guidance about exercise equipment, accessible exercise facilities, and transportation
Suggest strategies to increase self-efficacy, accountability, planning and goal-setting, and self-monitoring, to help the person sustain her or his exercise and lifestyle physical activities.
Experts in the field are urged to collaborate with the National MS Society and other advocacy organizations to create, evaluate, and disseminate the materials needed by healthcare professionals to fulfill this role.
Every patient can benefit from guidance that is tailored to her or his needs, abilities, and preferences. To that end, recommendations for exercise and physical activity should include a range of options that take into account individual differences at every level of disability. While individuals with mild disability may continue to be as physically active as they always have, they may benefit from training by specialists in fatigue and energy management, and in ways to adapt their favorite activities to meet their needs. As the disease progresses and engaging in exercise and physical activity becomes more challenging, referrals to specialists are essential for ensuring that patients’ exercise and physical activity strategies are individualized to best meet their needs. For these professionals to offer optimal interventions, the existing gaps in our knowledge must be filled by additional research—particularly at higher levels of disability. In the meantime, the expert recommendations in this paper complement the published guidelines to enable clinicians to promote and guide exercise and physical activity in their more disabled patients.
Supplemental Material
MSJ915629_appendix – Supplemental material for Exercise and lifestyle physical activity recommendations for people with multiple sclerosis throughout the disease course
Supplemental material, MSJ915629_appendix for Exercise and lifestyle physical activity recommendations for people with multiple sclerosis throughout the disease course by Rosalind Kalb, Theodore R Brown, Susan Coote, Kathleen Costello, Ulrik Dalgas, Eric Garmon, Barbara Giesser, June Halper, Herb Karpatkin, Jennifer Keller, Alexander V Ng, Lara A Pilutti, Amanda Rohrig, Paul Van Asch, Kathleen Zackowski and Robert W Motl in Multiple Sclerosis Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Rosalind Kalb received a consulting fee from the National Multiple Sclerosis Society for the preparation of this manuscript. Dr Susan Coote receives funding from Novartis Pharmaceuticals to develop an exercise program for MS patients. The remaining authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: No funding, other than the consulting fee from the National Multiple Sclerosis Society to Dr Kalb for preparation of this manuscript, was received for the research and/ or publication of this paper.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.