
Abstract
Purpose:
To promote understanding of cognitive impairment in multiple sclerosis (MS), recommend optimal screening, monitoring, and treatment strategies, and address barriers to optimal management.
Methods:
The National MS Society (“Society”) convened experts in cognitive dysfunction (clinicians, researchers, and lay people with MS) to review the published literature, reach consensus on optimal strategies for screening, monitoring, and treating cognitive changes, and propose strategies to address barriers to optimal care.
Recommendations:
Based on current evidence, the Society makes the following recommendations, endorsed by the Consortium of Multiple Sclerosis Centers and the International Multiple Sclerosis Cognition Society:
Increased professional and patient awareness/education about the prevalence, impact, and appropriate management of cognitive symptoms.
For adults and children (8+ years of age) with clinical or magnetic resonance imaging (MRI) evidence of neurologic damage consistent with MS: As a minimum, early baseline screening with the Symbol Digit Modalities Test (SDMT) or similarly validated test, when the patient is clinically stable; Annual re-assessment with the same instrument, or more often as needed to (1) detect acute disease activity; (2) assess for treatment effects (e.g. starting/changing a disease-modifying therapy) or for relapse recovery; (3) evaluate progression of cognitive impairment; and/or (4) screen for new-onset cognitive problems.
For adults (18+ years): more comprehensive assessment for anyone who tests positive on initial cognitive screening or demonstrates significant cognitive decline, especially if there are concerns about comorbidities or the individual is applying for disability due to cognitive impairment.
For children (<18 years): neuropsychological evaluation for any unexplained change in school functioning (academic or behavioral).
Remedial interventions/accommodations for adults and children to improve functioning at home, work, or school.
Introduction
Despite all that is known about cognitive impairment in multiple sclerosis (MS) and its impact on individuals with MS and their families, cognitive function is still not openly discussed, routinely assessed, or optimally treated. 1 Ample evidence supports early and ongoing cognitive assessment and personalized treatment. However, significant barriers stand in the way of individuals with MS and their family members being able to access the care they need in this clinical domain.
The aims of this paper—which was developed by a multidisciplinary group of clinicians, researchers and people with MS chosen by the National Medical Advisory Committee of the National Multiple Sclerosis Society—are to:
Promote awareness of, and attention to, cognitive impairment—a common and highly disabling symptom of the disease;
Describe optimal screening, evaluation, and management of cognitive impairment as supported by the published literature;
Identify and address barriers that prevent people from getting the cognitive care they need;
Support the inclusion of cognition as a key component of comprehensive MS care and of lay and professional educational materials.
Recommendations to address the problem
Only by establishing high standards for the assessment and treatment of cognitive dysfunction is it possible to bring treatment of cognitive dysfunction up to the standards set in other areas of MS care and ensure that people with MS and their families receive adequate care in this critical domain. With this goal in mind, the National Multiple Sclerosis Society recommends the following (See Table 1).
Recommendations for education, assessment, treatment, and access.
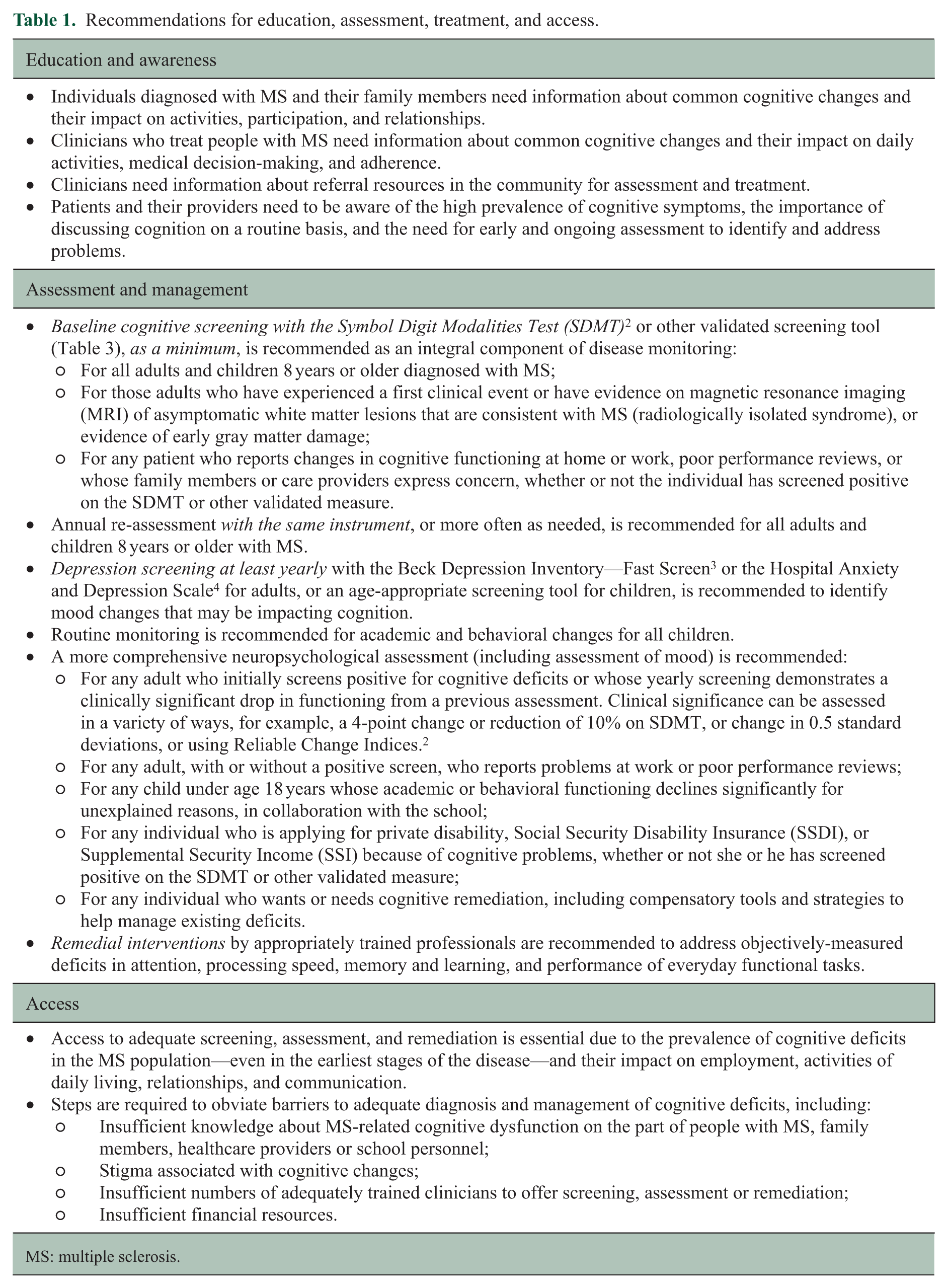
MS: multiple sclerosis.
Background
Etiology and prevalence of cognitive dysfunction
MS is characterized by inflammatory demyelination and neurodegeneration resulting in damage to both white and gray matter in the central nervous system (CNS). This CNS damage leads to a wide range of symptoms, including changes in cognitive functioning.5–7
Cognitive change is common in adults and children with MS. Depending on the sample studied (community vs clinic) and the criteria applied, the prevalence in adults ranges from 34% to 65%8–10 and is approximately 33% in patients under 18 years of age.11,12
Cognitive impairment occurs in all MS phenotypes,13–15 including clinically isolated syndrome (CIS),16,17 and has also been demonstrated in radiologically isolated syndrome (RIS). 18 In fact, cognitive impairment appears to predate the appearance of structural abnormalities on magnetic resonance imaging (MRI) and may serve as an early marker of disease activity.16,19 In a prospective study of cognitive performance prior to the first clinical symptoms of MS, Cortese et al. 20 found that men in the Norwegian Conscript Service database who later developed MS demonstrated significantly lower intelligent quotient scores than male controls, and those who developed primary progressive MS (PPMS) scored significantly lower than controls up to 20 years prior to their first progressive MS symptoms.
Progressive decline in cognitive functioning has been documented in some, but not all, longitudinal studies over short durations (1–3 years), 21 and while controlled studies are lacking, there is strong consensus that cognition declines in patients over longer (10–20 years) periods of time.22,23 Overall, the prevalence and severity of cognitive impairment appears greatest in secondary progressive MS (SPMS) and PPMS patients.13,24 In a 10-year follow-up of cognitive functioning in patients with MS, degree of physical disability, progressive disease course, and increasing age predicted the extent of cognitive decline, and limitations in a person’s work and social activities were correlated with degree of cognitive decline independent of the person’s level of physical disability. 22 However, not all individuals with MS experience cognitive impairment and not all of those with impairment progress significantly. Adults with early cognitive impairment tend to show greater decline.22,25,26 MRI predictors of cognitive outcomes over 7 years included diffuse brain damage and progressive central brain atrophy during the first 2 years after diagnosis. 27
Some, but not all, longitudinal studies of cognition in pediatric MS demonstrate worsening over time. 11 Younger age at onset may be a risk factor for pediatric MS-associated cognitive problems.
Cognitive symptoms and their impact on functioning and quality of life
Information processing and memory are the most commonly affected cognitive domains in MS.2,5 Other cognitive symptoms include deficits in complex attention, executive functioning, verbal fluency, visuospatial perception5,10,28 and social cognition.29,30
Slowed information processing speed is the hallmark cognitive deficit in MS,2,5,24,31,32 with processing deficits found in newly diagnosed relapsing-remitting (RRMS) patients, 32 as well as CIS16,18 and RIS. 18 Processing speed is a foundation for higher-level cognitive processes—which means that slowed processing impacts downstream domains. 31 For example, significant variance in new learning can be attributed to processing speed. 33 Similarly, in one study, after controlling for processing speed, there are no differences between healthy controls and people with MS in executive functioning. 34 And, cognitive speed is the primary factor impacting daily activities and participation in everyday life. 35
However, like all symptoms of MS, cognitive impairment is highly variable in severity and progression. Some patients may not decline or decline slowly, while others may experience significant decline. Some changes may be relatively mild and easily compensated for, while others may impact functioning in key areas of daily life, including work, driving, or management of business affairs. Table 2 highlights the potential impact of cognitive deficits on daily functioning and quality of life—demonstrating the need to screen for deficits, assess their severity, and remediate cognitive challenges that impair functioning.
Impact of cognitive deficits on daily functioning and quality of life.
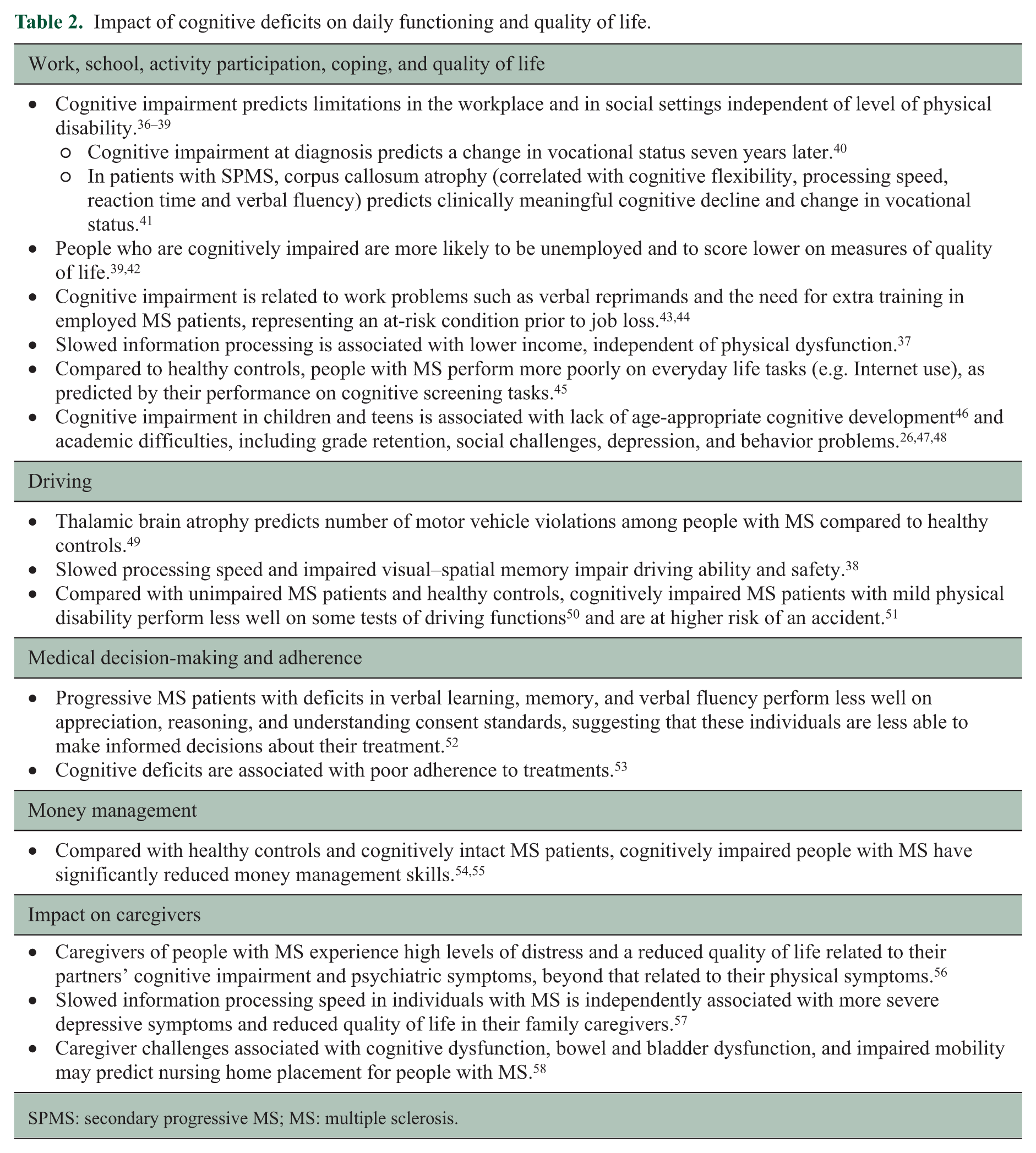
SPMS: secondary progressive MS; MS: multiple sclerosis.
Establishing a standard of care for cognitive dysfunction in MS
Appropriate management of cognitive dysfunction in MS includes education for people with MS and their family members, early screening and ongoing monitoring throughout the disease course, and interventions to remediate dysfunction and provide compensatory strategies to optimize function and participation.
Early screening followed by ongoing monitoring
The standard components of the neurologic exam, including the Mini-Mental State Exam or asking patients to remember three words or objects are not sufficient to detect cognitive impairment in MS.1,59–61 Several valid and reliable brief screening and evaluation tools have been used in MS (See Table 3).
Validated screening and evaluation tools used in MS.
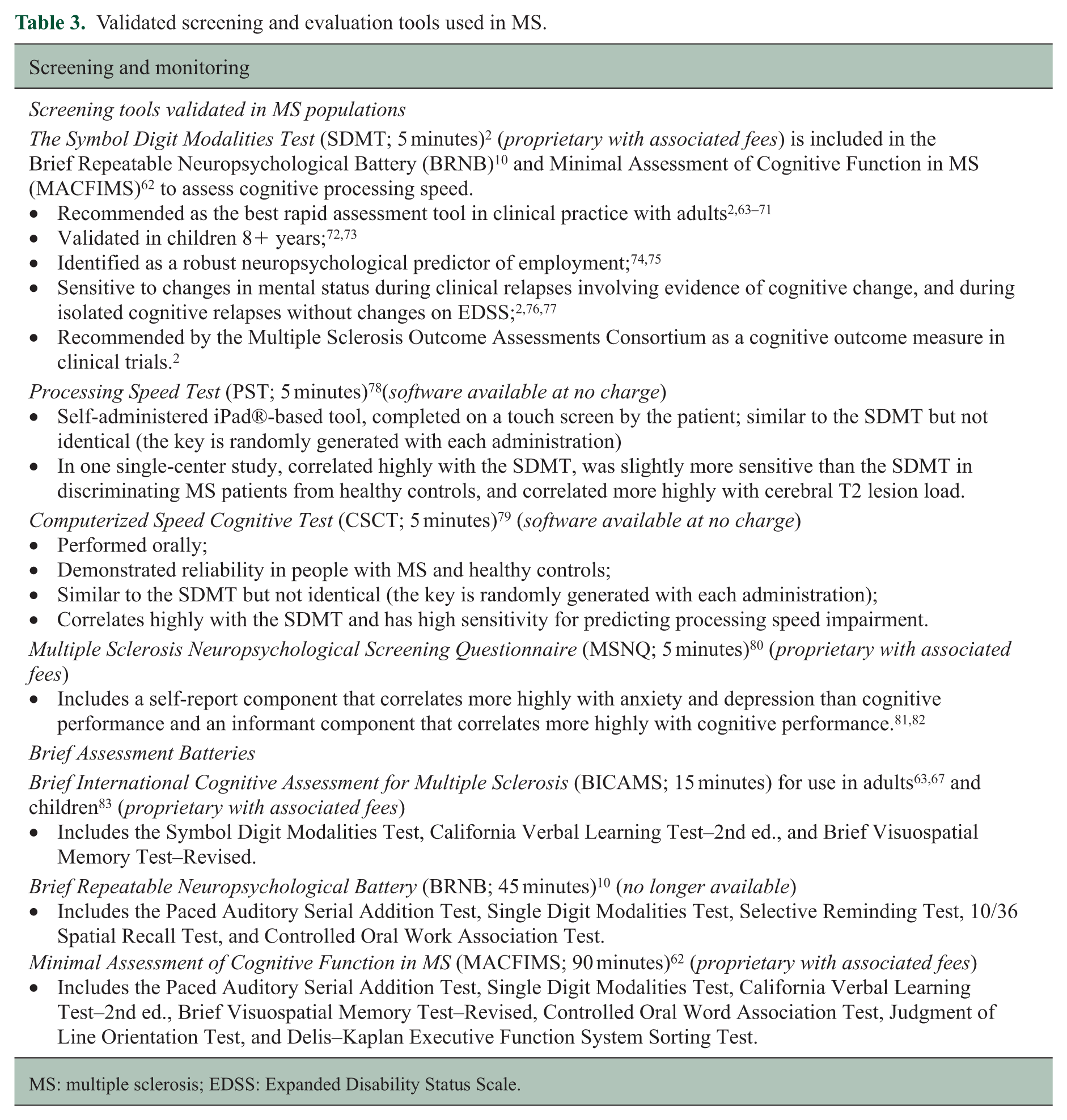
MS: multiple sclerosis; EDSS: Expanded Disability Status Scale.
Assessment of cognitive function early in the disease course has been shown not only to identify individuals with cognitive impairment but also to predict future impairments, limitations, and MS disease progression. Therefore, early detection of cognitive change may lead to earlier, more targeted treatment interventions:
Given that significant cognitive impairment has been found in individuals with CIS and RIS,16,18 and that cognitive relapses can occur independent of sensorimotor changes or subjective cognitive deficits,76,84 early, regular cognitive assessments can help clinicians recognize MS disease activity and tailor treatment recommendations.
Clinically silent T2 lesions in the frontal, parietal, and temporal lobes impact cognition, with deficits in cognitive processing speed, executive function, and memory occurring in the absence of Expanded Disability Status Scale (EDSS) progression. 85
Cognitive impairment at the time of diagnosis, particularly processing speed and memory, predicts disability progression and conversion to SPMS.86–88 In a 10-year longitudinal study, patients with cognitive impairment at baseline had a three times greater rate of reaching an EDSS of 4.0 and two times greater rate of conversion to SPMS compared to patients without cognitive impairment. 88
Early and ongoing cognitive screening could identify: ○ Patients at risk of income or job loss43,44,74 so that potential accommodations could be implemented in the workplace. In addition, successful applications for Social Security Disability Insurance (SSDI) and Supple-mental Security Income (SSI) require clear documentation in the medical record of symptom worsening over time; Deficits that interfere with driving and inform necessary accommodations to improve safety; Individuals who may have difficulties with self-care, treatment adherence and medical decision-making—thereby enabling providers to tailor patient interactions.52,89
Since cognitive deficits in children can be present as early as the first relapse or diagnosis of CIS, 12 early recognition and monitoring are essential for ensuring optimal academic, social, and emotional support and for minimizing future vocational problems.11,90 Such monitoring can also assist with planning as pediatric-onset MS patients may be at greater risk for physical and cognitive disability than adult-onset patients. 91
Current definitions of “benign MS” take physical disability into account but do not consider cognitive impairment:92,93
In a study comparing non-benign and benign patients, Gajofatto and colleagues found that both groups were cognitively impaired at baseline. Although significantly more subjects in the non-benign group progressed on the Expanded Disability Status Scale (EDSS) after 5 years, the proportion of subjects with cognitive impairment increased by the same amount in both groups during the same time period.
94
No evidence of disease activity (NEDA) diminishes from 31% to 17% when cognitive function is accounted for in MS.
95
Cognitive assessment and MRI metrics in people with benign MS can predict short-term disease evolution to SPMS and EDSS ⩾ 4.
96
A longitudinal cohort study of benign MS patients led investigators to conclude that routine monitoring of non-motor symptoms (including cognitive dysfunction) and imaging studies can improve diagnostic accuracy and treatment recommendations.
97
A positive cognitive screen at any point in time may indicate the need for a more comprehensive evaluation to assess a person’s cognitive and emotional status and suggest accommodations to enhance functioning at home and work.
Comprehensive evaluation as needed to identify areas of cognitive deficit and strength
Following a positive screen with the Symbol Digit Modalities Test (SDMT) or other validated measure, a more thorough assessment by a neuropsychologist or other trained specialist (psychologist, speech/language pathologist, or occupational therapist) is recommended to assess areas of cognitive deficit and strength, as well as to evaluate all factors that could be impacting cognitive functioning, such as cognitive reserve,98–101 depression and/or anxiety102–107 fatigue, co-morbid health conditions, and medications. Studies have demonstrated the importance of identifying a person’s areas of deficit in order to determine which remedial interventions are likely to be of greatest benefit and in which order they should be provided.102,103 For example, processing speed, which impacts a variety of cognitive functions,2,108 also impacts a person’s ability to benefit from memory retraining interventions. However, these assessments are long, expensive, not always covered by insurance, and may be unavailable in some areas of the country (see potential barriers below). Some speech/language pathologists and occupational therapists also provide evaluations, although their assessment tools may be less sensitive and comprehensive.
For a person who is planning to apply for private disability or SSDI/SSI with cognitive impairment as a reason for leaving the workforce, a thorough assessment is essential, even if the person must travel some distance for that evaluation. 109
The Minimal Assessment of Cognitive Function in MS (MACFIMS) covers the essential components of a neuropsychological assessment to quantify MS-associated neurocognitive disorder. 62 In the absence of a complete neuropsychological assessment, the Brief Repeatable Neuropsychological Battery (BRNB), 10 and the shorter Brief International Cognitive Assessment for Multiple Sclerosis (BICAMS) 63 assess the cognitive functions that are most likely to be impaired in MS. The MACFIMS is unique in assessing executive function (Delis–Kaplan Executive Function Scale; D-KEFS). The BICAMS has been shown to predict actual performance of everyday tasks more accurately than self-report. 45
Treatment to address functional deficits
Various treatment modalities have been studied to address cognitive dysfunction in MS, including cognitive remediation, exercise, and pharmacologic management. Although studies have been limited by symptom variation, as well as design issues, recent findings highlight the positive impact of cognitive remediation 110 and suggest a potential benefit of some exercise strategies. The evidence for pharmacologic interventions remains very limited (See Table 4).
Treatment modalities for cognitive impairment in MS.
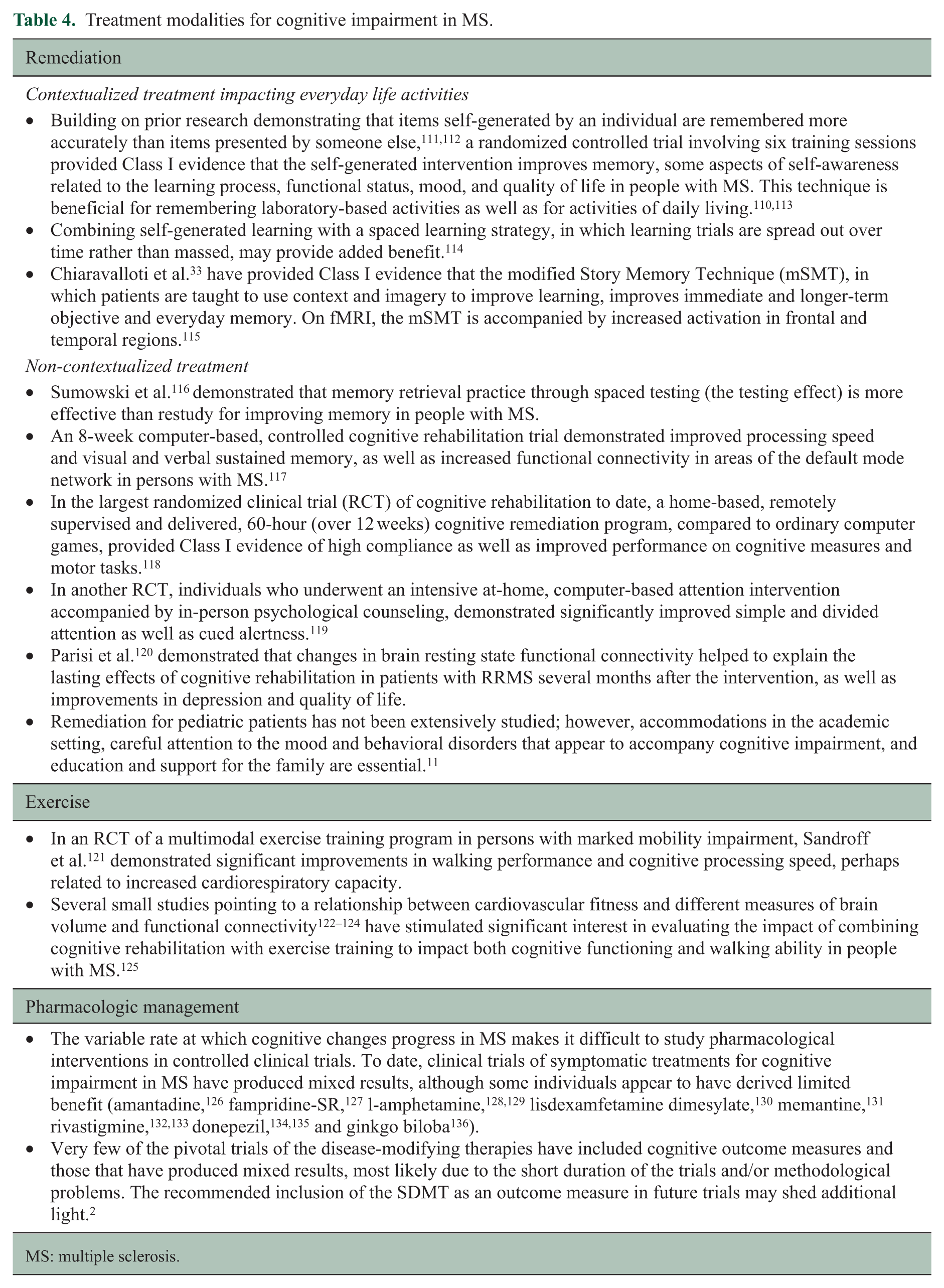
MS: multiple sclerosis.
An updated review of the literature on cognitive rehabilitation for people with MS identifies specific tools that can be considered as practice standard for use by rehabilitation specialists. 137 Patients who require rehabilitation to address cognitive changes impacting their functioning at home or at work should be referred to a specialist. The optimal referral is to a specialist in MS neuropsychological rehabilitation (neuropsychologist, speech/language pathologist or occupational therapist); the second option is referral to a neuropsychological rehabilitation specialist without MS-specific expertise; the third option is referral to a behavioral health specialist who is willing to learn about MS and cognition.
Managing other factors that impact cognition
The assessment and management of cognitive impairment must take into account a variety of factors that are known to impact cognition since adequate management of those factors may improve cognitive performance.
The interaction of mood, fatigue, sleep problems, and cognition.
The research in this area suggests a complex interrelationship between mood, fatigue, and sleep in people with MS, which in turn have a variable impact on both objective and self-reported cognitive functioning. Effective management of each of these factors is likely to improve the accuracy of both objective and subjective assessments of cognitive dysfunction:
Depression and anxiety appear to worsen memory, processing speed and executive functioning in people with MS.105–107,138,139
Self-reported sleep problems in MS patients with depression, fatigue, or pain, contribute to perceived cognitive problems above and beyond the impact of depressive symptoms. 140
Sleep disturbance and obstructive sleep apnea are associated with decreased visual and verbal memory, executive function, attention, processing speed and working memory, such that optimal management of sleep problems may improve cognitive functioning in people with MS.141,142
Medications and Cannabis.
Anticholinergic medications used on a chronic basis to treat overactive bladder significantly reduce information processing speed and some memory functions. 143
Because polypharmacy may result in cognitive impairment and/or fatigue that can compound the cognitive issues, a thorough medication review is recommended. 144
Smoked cannabis users are more cognitively impaired than non-users, particularly in information processing speed and memory,145–147 with more marked cognitive deficits associated with decreased gray and white matter volume. 148 Male users are potentially more vulnerable to cognitive deficits. 149
Acknowledging and addressing the barriers to optimal care
Information about the barriers to optimal care comes primarily from anecdotal reporting by people with MS and healthcare providers in various clinical settings. The authors of this paper represent the perspectives of patients and providers as well as the experiences in MS specialty centers, academic centers, and community settings. Based on these sources, the following barriers have been identified:
Insufficient knowledge on the part of people with MS, family members, and healthcare professionals regarding:
Prevalence, scope, and impact of cognitive dysfunction. Impact of mood changes, fatigue, sleep disruption, and medications on cognition. Availability of, or access to, validated screening and assessment tools and remediation strategies.
Reluctance to discuss cognitive symptoms on the part of:
Clinicians who feel they do not have referral options or the time or expertise to address assessment and treatment options. Patients who feel embarrassed or are afraid to report changes because it might threaten their employment, custody of children, license to drive, and/or independence.
Reluctance to address cognitive symptoms due to:
Number of disease- and symptom management issues needing attention during an office visit. Insufficient numbers of trained clinicians to do screening, testing, and remediation. Poor communication and coordination of care either within a single care team or from one provider to another. Cost of screening tools. Inadequate reimbursement for screening and treatment. Inadequate financial resources for MS treatment centers to hire the appropriate staff.
Although these barriers must be acknowledged and overcome, doing nothing in the meantime to address cognitive challenges among people living with MS is not acceptable. The critical steps going forward are to ensure that people with MS get the care they need while efforts are made to reduce the barriers. Strategies to address barriers to optimal care are listed in Table 5.
Strategies to address barriers to optimal care.
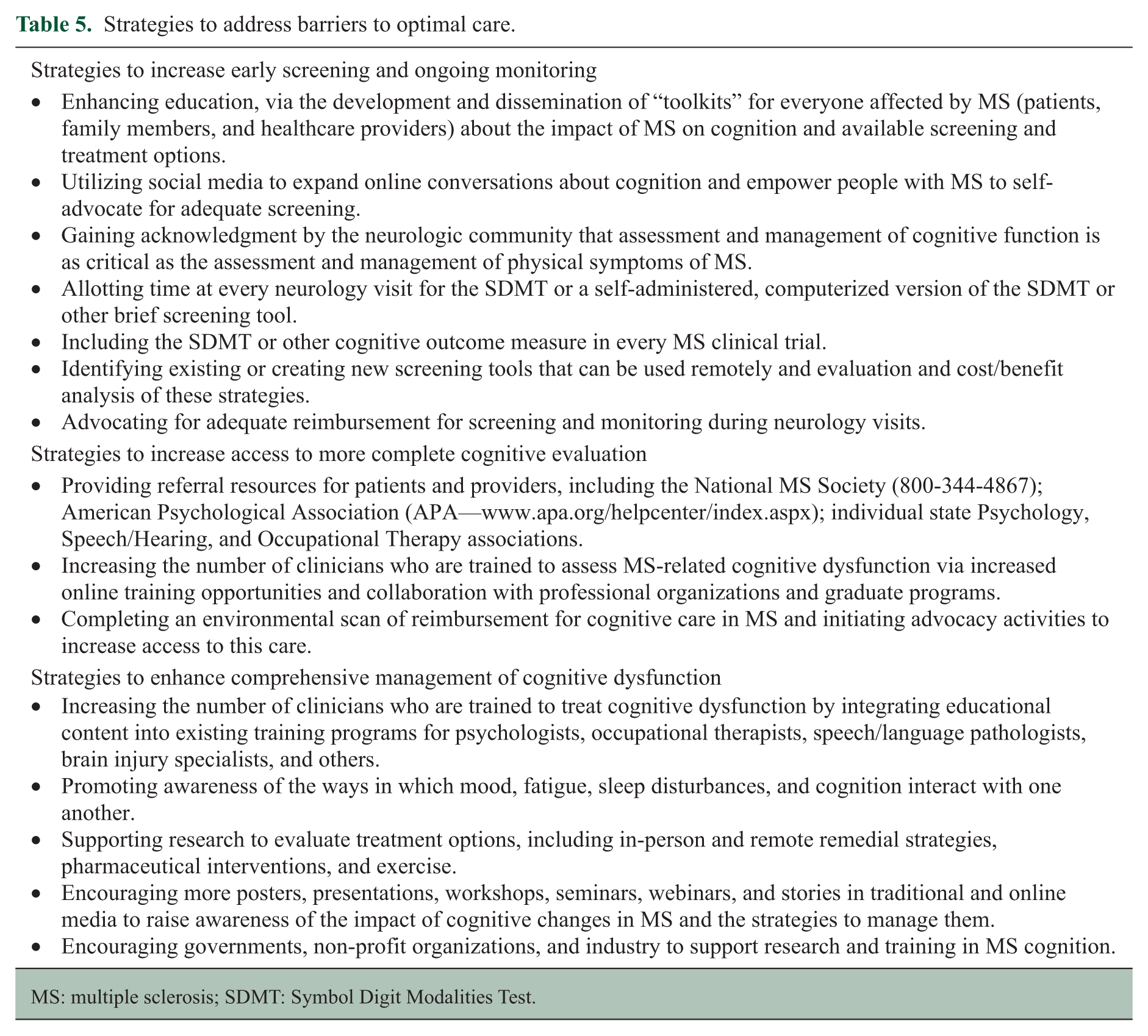
MS: multiple sclerosis; SDMT: Symbol Digit Modalities Test.
Summary
Comprehensive MS care requires (1) improved education about cognition for healthcare providers and individuals and families affected by MS; (2) baseline screening, as a minimum, with the SDMT or other validated screening tool when the patient is stable; annual re-assessment with the same tool for all adults and children 8 years of age or older to (a) detect acute disease activity, (b) assess for treatment effects (e.g. starting or switching disease-modifying therapy) or recovery from relapses, (c) evaluate progression of cognitive impairment, and/or (d) screen for new-onset cognitive problems; (3) a more comprehensive cognitive assessment for any adult or child who tests positive on initial cognitive screening or demonstrates a significant cognitive decline, as well as any individual who is applying for private disability, SSDI/SSI due to cognitive impairment; and (4) remedial interventions to improve functioning at home, work, or school.
Together, the MS community—including people with MS, family members, healthcare providers, MS advocacy organization—can improve the quality of care and access to care for MS-related cognitive dysfunction.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.