
Abstract
Background:
Although many individuals with multiple sclerosis (MS) experience depression, there are no studies on the frequency and effect of peripartum depression among parents with MS.
Objective:
To examine the frequency of peripartum depression in individuals with MS and its potential association with children’s psychiatric disorders.
Methods:
We conducted a cohort study in British Columbia, Canada, using linked health databases, of parents with MS and their children, and age-matched unaffected parent–child dyads. The diagnosis of peripartum depression, MS and psychiatric disorders in children was based on information from hospital admission, physician visit and drug prescription claims.
Results:
Peripartum depression was significantly more common among MS parents (n = 360) versus unaffected (n = 1207) parents (25.8% vs 18.5%, p value 0.02), especially among MS affected fathers versus unaffected fathers (25.7% vs 10.2%, p value < 0.001). The incidence of psychiatric disorders in children was 3.3 and 2.7 per 100 child-years among children with and without an MS parent, respectively. The rate of psychiatric disorders was significantly higher in children with an MS parent (vs without, hazard ratio (HR): 1.34; 95% confidence interval (CI): 1.03–1.74) and among children with parents who had peripartum depression (HR: 1.87; 95% CI: 1.36–2.55).
Conclusion:
Parental MS is associated with a higher risk of peripartum depression and increases the risk of psychiatric disorders in children.
Introduction
Peripartum depression is the most frequent form of maternal morbidity in pregnancy and affects 15%–20% of mothers in the first year following delivery; 10% of fathers are also affected.1,2 Peripartum depression is under-recognized and adherence to treatment is poor. Approximately 18% of women exhibit depressive symptoms antenatally. 3 In 2013, the American Psychiatric Association amended the nomenclature postpartum depression to peripartum depression and stipulated that the onset of depression can occur in pregnancy or after childbirth. 4 Peripartum depression affects the individual’s quality of life; its impact extends to the partner and family and influences mother–child attachment. 5
Multiple sclerosis (MS) is a chronic condition of the central nervous system, with clinical symptoms characteristically manifesting in early adulthood aged between 20 and 40 years, when individuals are of reproductive age. 6 Depression and anxiety affect individuals with MS at twice the frequency observed among people without MS. 7 Although many individuals with MS will experience depression, there is a dearth of information on the rate of peripartum depression among parents with MS.
Maternal postnatal psychological distress is a significant predictor of childhood anxiety even after controlling for distress in the prenatal and early childhood periods. 8 Previous work has demonstrated that parents with MS have a substantially higher rate of mental health disorders as compared with parents not affected by MS. Also, children of a parent who has both MS and a coexisting mental health condition are at an increased risk of developmental problems.9,10 We, therefore, carried out a study to examine the timing of parental depression, specifically peripartum depression, and its potential association with psychiatric disorders among children exposed to parental MS since birth.
Methods
This study was part of a broader programme of research examining the association between parental MS and routinely collected childhood developmental outcomes. The publicly funded provincial health care programme in British Columbia covers all residents; a lifelong unique personal health care number is assigned to each resident and available in all health databases. The anonymized linked health data files used in this study included the Discharge Abstract Database (with hospital admission dates and diagnosis codes), 11 the Medical Services Plan Billing database (providing information on physician visits and diagnosis codes), 12 the PharmaNet database (with information on dispensed prescriptions) 13 and Vital Statistics birth files (with records of all births in the province). 14 Registration files 15 provided dates of entry and exit from the provincial health care plan (which confirmed residency in British Columbia), and socioeconomic status (SES) was based on average neighbourhood income (obtained through postal codes and national census data), 16 expressed as quintiles. Diagnoses in these databases were coded using the International Classification of Diseases codes (ICD-9 or ICD-10-CA), and prescription medications were coded using Drug Identification Numbers and the Anatomical Therapeutic Chemical (ATC) classification system.
MS in parents was identified using a validated algorithm, as those with ⩾3 records related to MS in hospital admission or physician visit claims between 1 April 1985 and 31 December 2011 or in prescription claims after 1 April 1996 (Supplementary Appendix Table 1). 17 Parents with MS were linked to their offspring using the birth registry and the registration file databases. All persons with MS who had a child born in British Columbia between 1 January 1994 and 31 December 2006 were included in the study cohort. The MS cohort was restricted to individuals whose MS onset occurred before their child’s birth, based on the first date for MS or a demyelinating condition identified in any of the hospital, physician or prescription claims (Supplementary Appendix Table 1). A matched reference cohort of up to four children with parents who were not known to have MS or a demyelinating condition was selected from the population of British Columbia. Children in the matched reference cohort were matched on the year of birth and school district. The parent with MS was also matched by sex to a parent in the reference cohort. In instances where exact matching for parental sex could not be carried out (i.e. in 4% of cases), the available parent in the database was selected. Children for whom both parents had MS were excluded. All children in the study were followed up for a minimum of 4 years and up to 18 years between 1994 and 2011.
Peripartum depression was defined to include mood or anxiety disorders since these conditions have a shared psychopathology, are highly comorbid and are often difficult to distinguish in primary care.18,19 Parents in the study were classified as having peripartum depression if they had one or more records related to mood disorders or anxiety in hospital, physician or prescription drug claims in the last 4 weeks before delivery and up to 12 months after the child’s birth (Supplementary Appendix Table 1). Subsequent parental depression or anxiety (in the period following the peripartum period) was identified based on one or more records related to mood disorders or anxiety in hospital, physician or prescription drug claims after the peripartum period. History of depression was defined as the presence of depression or anxiety in the 2 years prior to the peripartum period.
Psychiatric disorders in children were defined based on one or more records for internalizing (mood or anxiety) psychiatric disorders or externalizing (attention-deficit hyperactivity disorder (ADHD) or conduct) psychiatric disorders in physician or hospital claims (Supplementary Appendix Table 1).20,21 The date associated with the first record of such a psychiatric disorder was considered the date of onset for the condition. Diagnosis of a psychiatric disorder in children was restricted to the period after the child’s fourth birthday since the accurate diagnosis of depressive and anxiety disorders in very young children is often difficult due to issues related to cognitive and emotional immaturity, and the asymptomatic expression of depression in children.19,22 Although recent studies20,21 have used a similar approach to identifying mental health disorders, we also identified mental health disorders in children and parents using a previously validated algorithm.22,23 The latter diagnoses were used in a sensitivity analysis to assess whether results comparing children of parents with and without MS were affected by potential changes in diagnostic accuracy.
The date of cohort entry (index date) for all children was defined as the month of the child’s fourth birthday. Children were followed up from the index date until the first diagnosis of a psychiatric disorder, emigration from British Columbia or the study end date, which was 31 December 2011. The child’s characteristics examined included sex, the child’s first language at home (English vs other), presence of an older sibling (yes vs no) and SES at index date (expressed as quintiles). The parental characteristics studied included parental sex, parental age (continuous) and marital status at the time of the child’s birth.
Conditional logistic regression was used to compare the characteristics of the parent–child dyads in the MS and matched reference cohorts. The frequency of peripartum depression among parents with and without MS was estimated using cumulative rates and 95% confidence intervals (CIs). Multivariable log-linear regression models with robust variance estimators 24 were used to determine the association between parental MS and peripartum depression, after adjusting for potential confounders including parental marital status, parental subsequent depression or anxiety, age at the time of the child’s birth, parental sex and SES.
The incidence (density) of psychiatric disorders in children among parents with and without MS was quantified by dividing the number of children with psychiatric disorders by the total follow-up time in child-years in each category. Incidence patterns of psychiatric disorders in children were examined using Kaplan–Meier curves and Cox proportional hazard regression accounting for matched factors. In the Cox models, standard errors were adjusted for within-family clustering 25 to account for the sequential births to the same parent in the cohort. Confounders were included in the final model based on the literature26,27 or statistical significance (p value < 0.1), and the proportionality assumption in the Cox model was checked for each variable in the model. 28 The full Cox model included the child’s sex (female vs male), SES (expressed as quintiles), peripartum depression (present vs absent), parental subsequent depression or anxiety (present vs absent) and parental marital status (not married vs married). Modification of the effect of parental MS by other factors was examined using interaction terms, and stratified analyses were presented to illustrate potential effect modification.
Results were expressed as odds ratios (ORs) and hazard ratios (HRs) with 95% CIs. Regression model fit was assessed using the likelihood ratio test, and a two-sided p value <0.05 was used to determine statistical significance. Analyses were performed using SAS Version 9.2 (SAS Institute Inc., Cary, NC). The University of British Columbia’s Clinical Research Ethics Board approved the study.
Results
The study cohort included 360 children with an MS parent and 1207 parent–child dyads in the matched reference cohort (Figure 1). The characteristics of children with a parent with MS and those with unaffected parents were similar in terms of sex, birth order and SES at cohort entry (Table 1). Parents affected by MS were on average older, more likely to be English speakers, have a higher frequency of subsequent depression and to be married at the time of the child’s birth. The median age at onset of MS was 28 years and the median disease duration at the index date was 8.5 years. Approximately 32% of the parents affected by MS had received disease-modifying medication by the index date (Table 2).
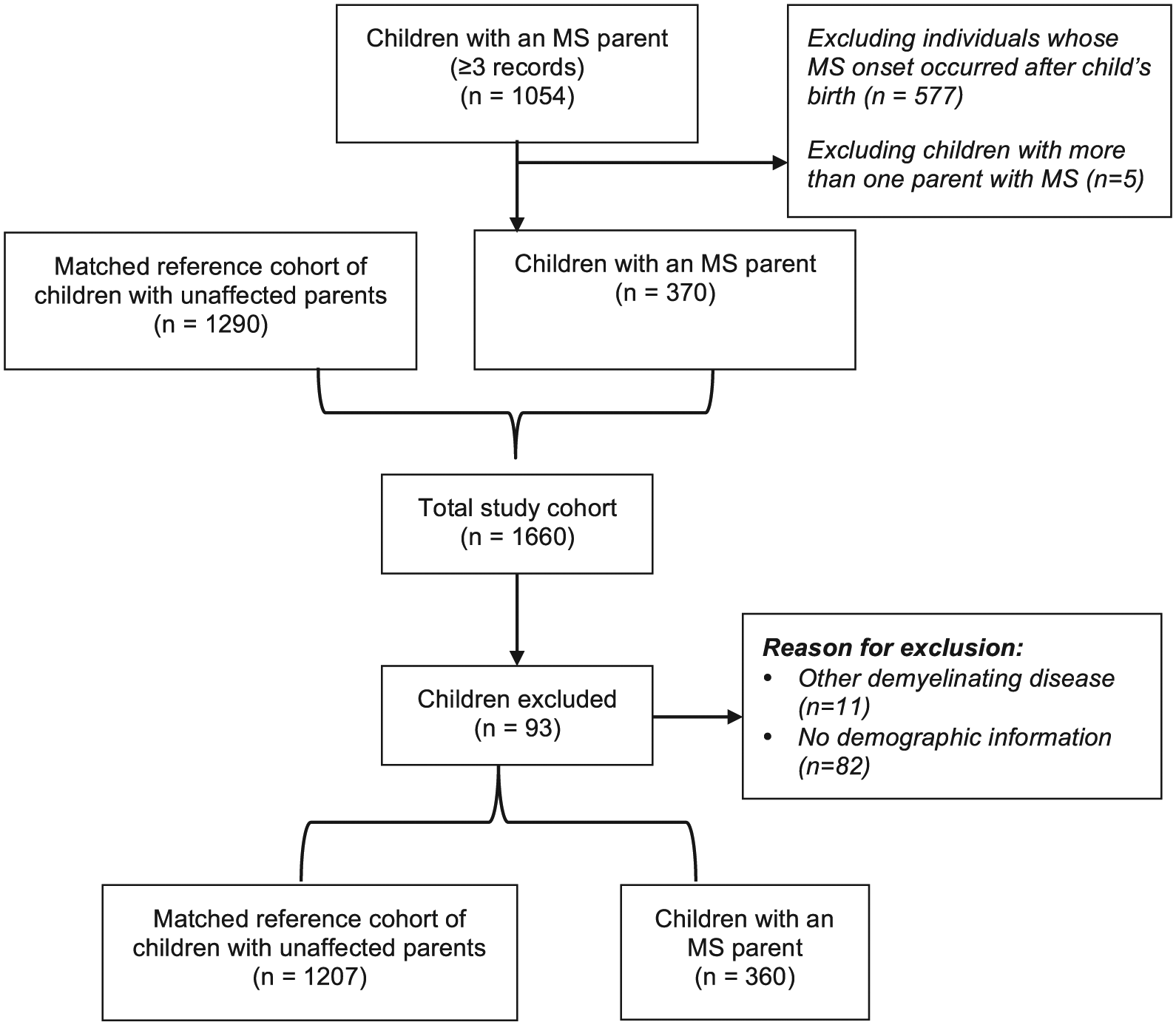
Schematic depiction of the cohort selection process.
Characteristics of parents with and without multiple sclerosis (MS) and their children, British Columbia, Canada.
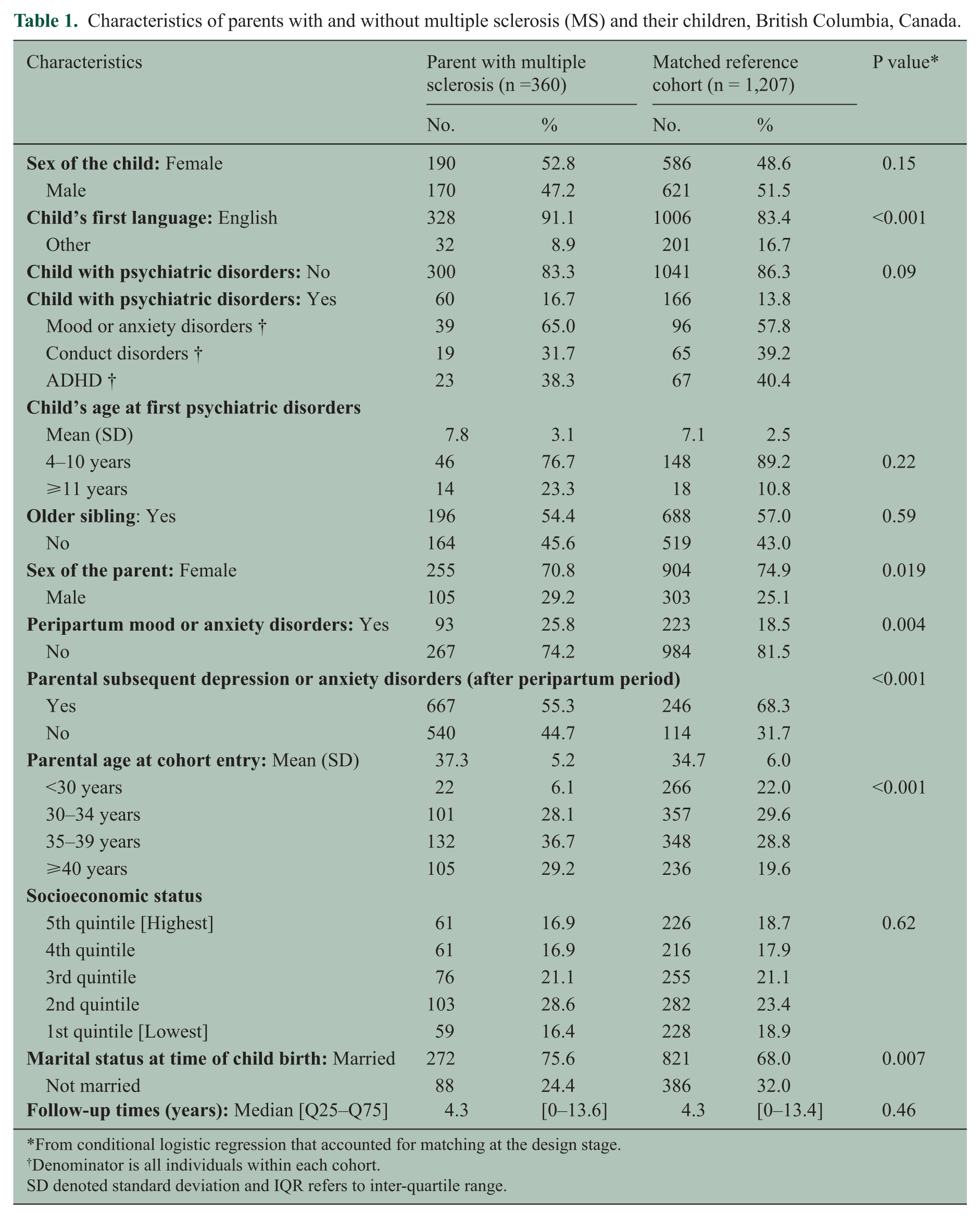
From conditional logistic regression that accounted for matching at the design stage.
Denominator is all individuals within each cohort.
SD denoted standard deviation and IQR refers to inter-quartile range.
Additional characteristics of the cohort of parents with multiple sclerosis (MS), British Columbia, Canada.
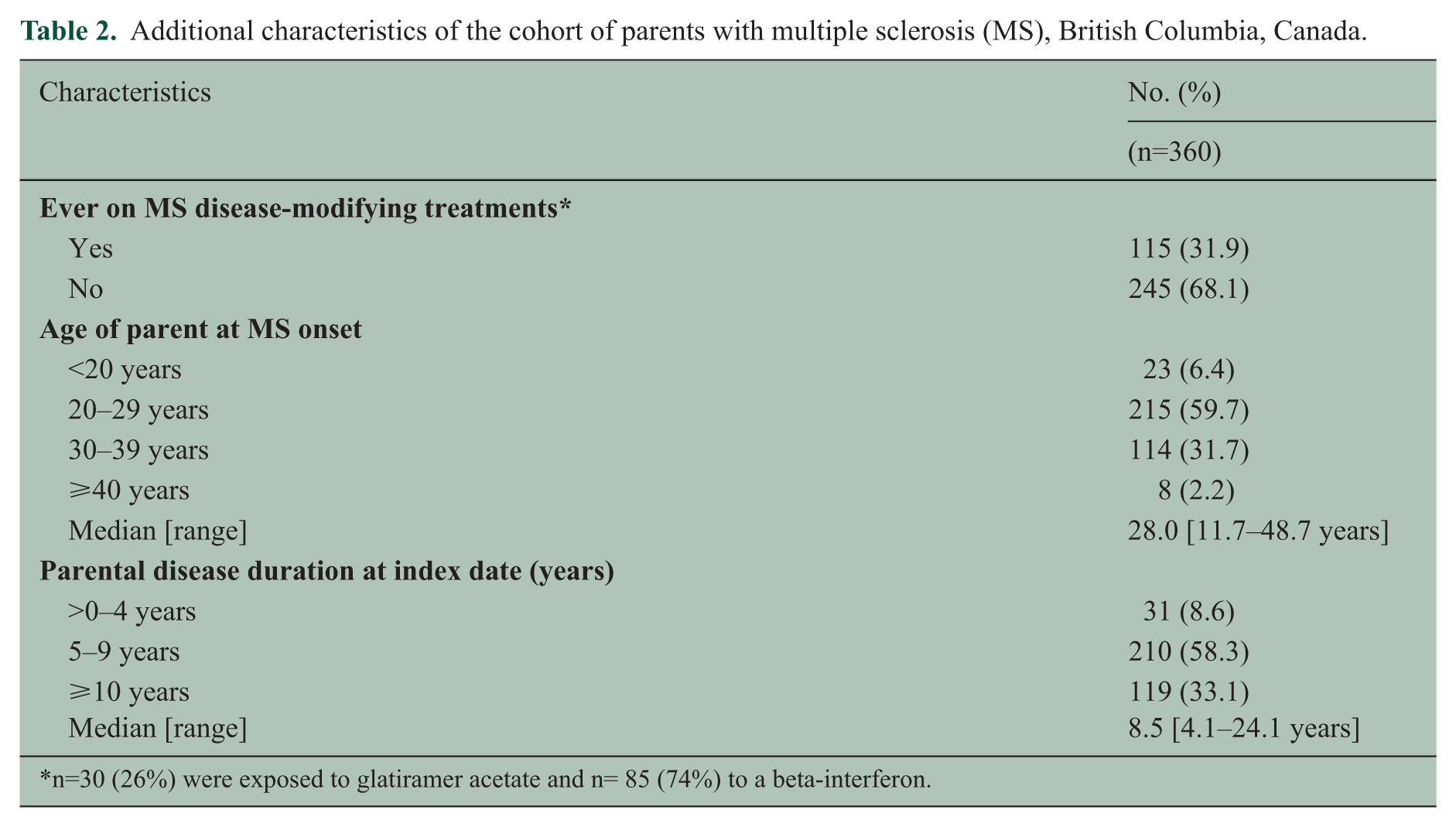
n=30 (26%) were exposed to glatiramer acetate and n= 85 (74%) to a beta-interferon.
A total of 316 (20%) parents were diagnosed with peripartum depression. Parents affected by MS had higher rates of peripartum depression compared with parents in the reference cohort (25.8% vs 18.5%, p value 0.004; Table 1). Similarly, fathers who had MS had considerably higher rates of peripartum depression compared with unaffected fathers (25.7% vs 10.2%; Figure 2). Among individuals with peripartum depression, 52% of parents with MS and 48% of unaffected parents had a prior history of depression (Supplementary Appendix Table 2). Adjusted analyses showed that parental sex modified the effect of parental MS on peripartum depression (p value for interaction term 0.008; Table 3). Adjusted analyses stratified by parental sex showed that the rate of peripartum depression was 2.68 times higher (95% CI: 1.68–4.29) among fathers with MS as compared with fathers not affected by MS, while the rate of peripartum depression was 28% higher (95% CI: 0.99–1.65) among mothers with MS as compared with mothers without MS.
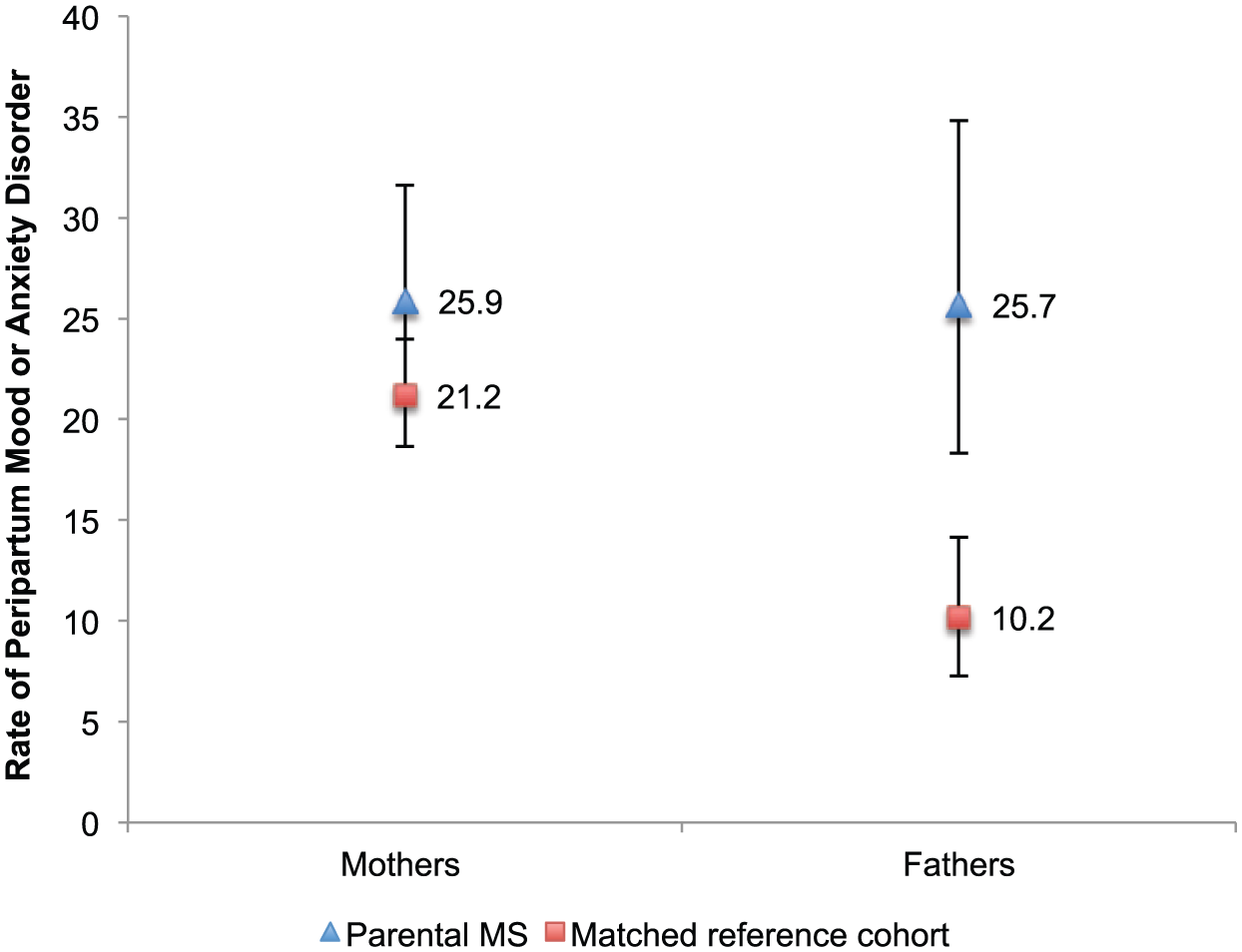
Peripartum depression (%) by parental multiple sclerosis (MS) status and parental sex, British Columbia, Canada. Error bars represent 95% confidence intervals.
Unadjusted and adjusted odds ratios and 95% confidence intervals from log-linear regression showing the association between parental multiple sclerosis (MS) and peripartum depression, British Columbia, Canada.
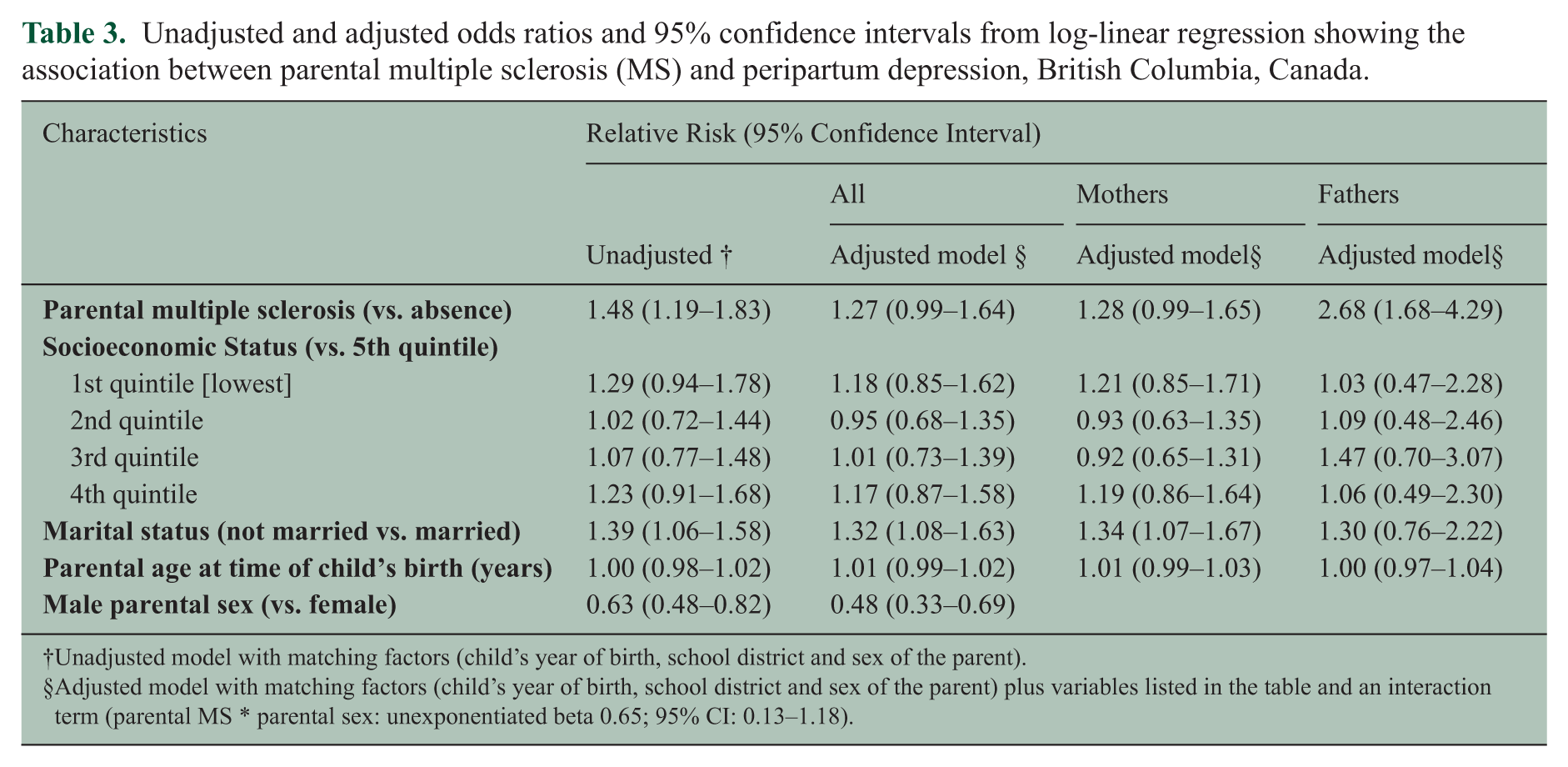
Unadjusted model with matching factors (child’s year of birth, school district and sex of the parent).
Adjusted model with matching factors (child’s year of birth, school district and sex of the parent) plus variables listed in the table and an interaction term (parental MS * parental sex: unexponentiated beta 0.65; 95% CI: 0.13–1.18).
During the follow-up period, 226 children (14%) were diagnosed with a psychiatric disorder (Table 1). Among children with psychiatric disorders, mood or anxiety disorders were more common than ADHD and conduct disorders. In the Kaplan–Meier analysis, 1309 (83.5%) children were followed up until the end of the study period, 226 (14.4%) until the diagnosis of a psychiatric disorder and 32 (2.1%) until emigration from the province. The incidence of psychiatric disorders in children aged 4–17 years (per 100 child-years) was 3.3 among children of parents with MS and 2.7 among those with parents not affected by MS (crude HR: 1.19; 95% CI: 0.93–1.54; Table 4). The incidence rate of psychiatric disorders in children was higher among boys, children whose parents had peripartum and subsequent depression and children whose parents were not married (Table 4).
Incidence of psychiatric disorders in children, British Columbia, Canada.
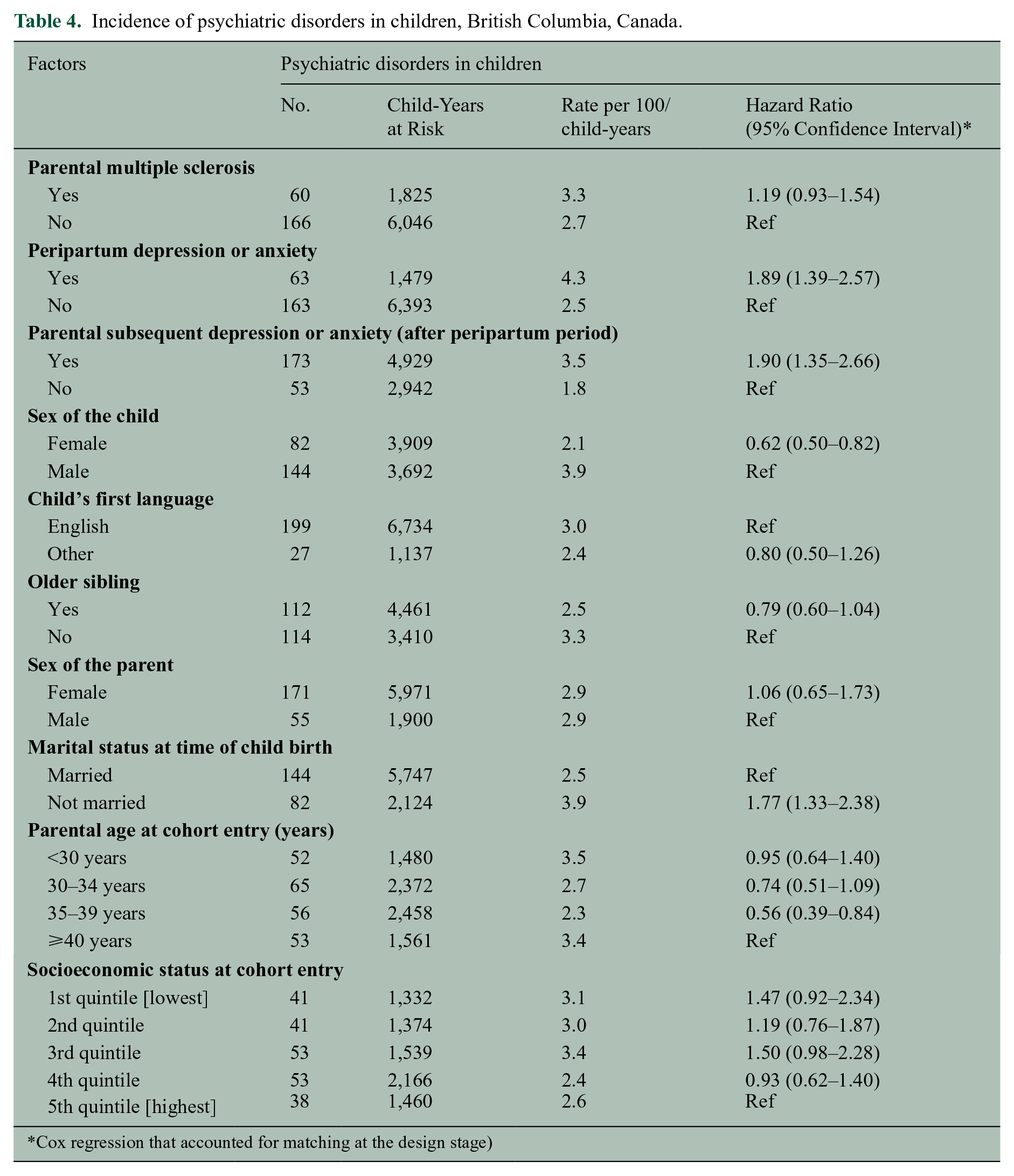
Cox regression that accounted for matching at the design stage)
The adjusted Cox model showed that children with parental MS had a 34% higher rate of psychiatric disorders compared with children without parental MS (adjusted HR: 1.34; 95% CI 1.03–1.74; Table 5, model 2). The rate of psychiatric disorders was also higher among children whose parents had peripartum depression compared with children whose parents did not have peripartum depression (adjusted HR: 1.87; 95% CI 1.3–2.55). Model 2 further showed that the relationship between parental MS and peripartum depression and child psychiatric disorders remained statistically significant even after controlling for subsequent parental depression or anxiety. Peripartum depression did not modify the effect of parental MS on psychiatric disorders in children (p value for interaction term 0.25). Sensitivity analyses based on mental health disorders identified using a previously validated algorithm yielded similar results.
Adjusted hazard ratios and 95% confidence intervals from Cox regression showing the association between parental multiple sclerosis (MS) and psychiatric disorders in children, British Columbia, Canada.
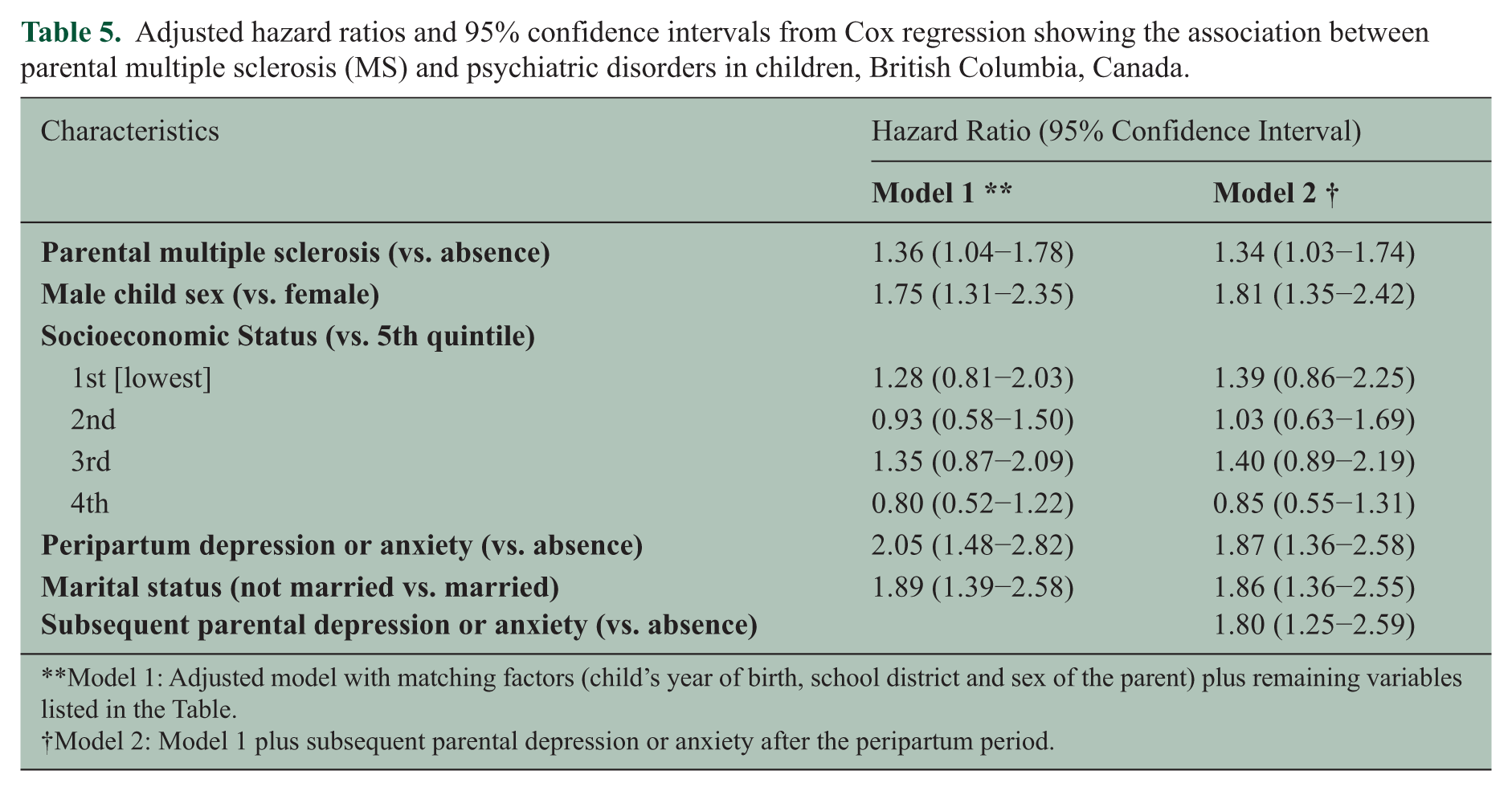
Model 1: Adjusted model with matching factors (child’s year of birth, school district and sex of the parent) plus remaining variables listed in the Table.
Model 2: Model 1 plus subsequent parental depression or anxiety after the peripartum period.
Sensitivity analyses carried out to ascertain whether the higher rate of peripartum depression among fathers with MS was secondary to their increased contact with the health care system showed that fathers with MS had an average of 11 physician visits during the peripartum period, while fathers without MS had 7 visits. The association between MS and peripartum depression among fathers was attenuated but remained significant even after adjusting for physician visits (rate ratio: 1.96; 95% CI 1.14–3.40).
Discussion
Our study provides evidence that parents with MS had an increased risk of peripartum depression as compared with parents unaffected by MS. Furthermore, children of parents with MS had a higher risk of developing psychiatric disorders compared with the children of parents without MS. Similarly, children whose parents had peripartum depression had a higher risk of developing psychiatric disorders compared with children of parents without peripartum depression. Higher rates of psychiatric disorders in children were also observed among boys, children whose parents had subsequent depression or anxiety and those who were not married.
To the best of our knowledge, there have been no previous reports that have quantified the frequency of depression or anxiety in the peripartum period among parents with MS. Studies in women with epilepsy show that approximately 25%–29% of such women screen positive for depression.29,30 In our study, approximately 26% of mothers with MS were identified as having peripartum depression or anxiety, compared with a lower 21% rate in mothers without MS. Depression is frequently missed among patients with MS and even when detected is often inadequately managed. 31 Maternal depression is particularly concerning because it is often a risk factor for a poor quality of life, paternal depression and adverse emotional, intellectual and cognitive development in children. 32 Peripartum depression in people with MS could also adversely impact an individual’s adherence to treatment, and this can have important consequences on their disease course. 33
In our study, fathers with MS had substantially higher rates of peripartum depression or anxiety (26%) compared with fathers without MS (10%). The latter rate is consistent with studies which show that peripartum depression is not uncommon among fathers and has a 12-month postpartum prevalence of 4%–10%. 2 An elevated risk of depression in those with MS compared with those without MS has also been observed in other studies; rates of depression among women with MS are 59% higher than among women without MS, while among men, rates of depression are 93% higher in those with MS compared with those without MS. 34 The higher risk of peripartum depression in men with MS could be triggered by their new role as fathers, which may require them to confront their physical or cognitive impairments and ability to address their family’s emotional and financial needs. 35 Furthermore, MS-related fatigue and physical disability and the unpredictable nature of MS symptoms can affect their ability to play an active role in caring for their young children and threaten their self-expectations of fatherhood.
The association between parental MS and psychiatric disorders in children is consistent with previous work demonstrating that maternal MS is associated with a higher rate of mood or anxiety disorders in children; this association appears to be mediated through maternal mental health morbidity. 36 The limited research on this issue supports the notion that children of parents with MS are at greater risk of psychiatric outcomes including higher levels of depression and anxiety as compared with the children of healthy parents. 10 Our study shows that both peripartum depression and subsequent parental depression independently increase the risk of psychiatric disorders in children. Other studies have also demonstrated that maternal postnatal psychological distress is a significant predictor of childhood anxiety even after controlling for distress in the prenatal and early childhood periods. 8 Studies examining the role of parental depression on child mental health suggest that the rates of psychiatric disorders among children of depressed parents are two to five times above normal and that the risk associated with maternal depressive symptoms may be comparable with that of paternal depressive symptoms. 32 Timely and appropriate interventions are key for such families; intervention studies targeted towards treatment for parental depression have shown significant improvement in children’s functioning and psychiatric symptoms within 1 year after initiation of treatment. 37
The strengths of our study include use of a comprehensive population-based data source and the use of previously validated case definitions for MS. The robustness of our analyses was also confirmed by the supplementary analyses in which psychiatric disorders were identified using a previously validated algorithm. We also accounted for the clustered nature of the data arising from sequential births to the same parent during the study period. One limitation of our study was our inability to assess severity of peripartum depression which could have differed between mothers and fathers. Furthermore, the time of onset of peripartum depression was defined as the date of the first record for a mood or anxiety disorder during the peripartum window, which may not necessarily represent the date of onset of symptoms. It is possible that more frequent contact with medical services in our MS cohort increased the opportunity to get diagnosed with a mental health disorder. However, adjustment for health services use did not abolish the association between paternal MS and peripartum depression. Another limitation of our study arose because the study sample was restricted to children born between 1994 and 2006, who had childhood developmental data. However, given that the assessment of childhood developmental outcomes has been routinely administered province-wide, the generalizability of our findings to the wider population of parents with MS was likely unaffected. Finally, we did not have a family-specific variable to assess SES, but used neighbourhood-level income as a proxy for SES.
Our study demonstrated that parental MS, specifically paternal MS, is associated with a higher risk of peripartum depression. Furthermore, parental MS and parental peripartum depression independently increase the risk of psychiatric disorders in children. Given that depression and other psychiatric disorders are believed to be under-diagnosed and under-treated in persons with MS, parents with MS require special attention from health care professionals to ensure that their mental health and their children’s mental health are optimized.
Footnotes
Acknowledgements
The authors gratefully acknowledge the late Professor Clyde Hertzman for providing guidance and helpful feedback in conceptualizing and planning this programme of research and for his role in obtaining funding. We thank the BC Ministry of Health, BC Vital Statistics Agency and BC PharmaNet for approval and support for accessing provincial data and Population Data BC for facilitating approval and use of the data.
Conflict of interest
Neda Razaz is funded by the Multiple Sclerosis Society of Canada (PhD Research Studentships). She has received travel grants from the Canadian Institutes of Health Research and the endMS Research and Training Network/Multiple Sclerosis Society of Canada. KS Joseph is the recipient of a Chair in maternal, foetal and infant health services research from the Canadian Institutes of Health Research. His work is also supported by the Child and Family Research Institute. Ruth Ann Marrie is supported by a Don Paty Career Development Award from the MS Society of Canada, and by a Manitoba Research Chair from Research Manitoba. Dr Marrie has received research support from CIHR, the MS Society of Canada, the National MS Society, Research Manitoba and the MS Scientific Research Foundation. She has conducted clinical trials for Sanofi-Aventis. Helen Tremlett is the Canada Research Chair in Neuroepidemiology and Multiple Sclerosis. She has received research support from the National Multiple Sclerosis Society, the Canadian Institutes of Health Research and the UK MS Trust; and speaker honoraria and/or travel expenses to attend conferences from the Consortium of MS Centres (2013), the National MS Society (2012, 2014), Bayer Pharmaceuticals (2010), Teva Pharmaceuticals (2011), ECTRIMS (2011, 2012, 2013, 2014), UK MS Trust (2011), the Chesapeake Health Education Program, US Veterans Affairs (2012), Novartis Canada (2012), Biogen Idec (2014), American Academy of Neurology (2013, 2014, 2015). Unless otherwise stated, all speaker honoraria were either donated to an MS charity or to an unrestricted grant for use by her research group.
Funding
This work was supported by the Canadian Institutes of Health Research (MOP-119393, PI Helen Tremlett).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.