
Abstract
Background:
Axonal and neuronal damage are widely accepted as key events in the disease course of multiple sclerosis. However, it has been unclear to date at which stage in disease evolution neurodegeneration begins and whether neuronal damage can occur even in the absence of acute inflammatory attacks.
Objective:
To characterize inner retinal layer changes in patients with clinically isolated syndrome (CIS).
Method:
45 patients with CIS and age- and sex-matched healthy controls were investigated using spectral domain optical coherence tomography. Patients’ eyes were stratified into the following categories according to history of optic neuritis (ON): eyes with clinically-diagnosed ON (CIS-ON), eyes with suspected subclinical ON (CIS-SON) as indicated by a visual evoked potential latency of >115ms and eyes unaffected by ON (CIS-NON).
Results:
CIS-NON eyes showed significant reduction of ganglion cell- and inner plexiform layer and a topography similar to that of CIS-ON eyes. Seven eyes were characterized as CIS-SON and likewise showed significant retinal layer thinning. The most pronounced thinning was present in CIS-ON eyes.
Conclusion:
Our findings indicate that retinal pathology does occur already in CIS. Intraretinal layer segmentation may be an easily applicable, non-invasive method for early detection of retinal pathology in patients unaffected by ON.
Keywords
Introduction
Multiple sclerosis is an autoimmune disorder of the central nervous system that often manifests with optic neuritis (ON) as well as motor, sensory or cerebellar deficits in its earliest stage. 1 Current diagnostic criteria for MS require proof of dissemination of lesions or attacks in time and space. 2 In everyday clinical practice, patients presenting with a first clinical event that is highly indicative of MS are often instead diagnosed with a clinically isolated syndrome (CIS) or ‘possible’ MS. 3 A confirmed diagnosis of MS is possible once additional attacks or lesions present, as is the case for a significant proportion of such patients. 2
In light of this, pinpointing the aspects of CIS that are most predictive for subsequent diagnosis with MS has high priority 3 so that patients at risk can be identified. Diagnosing MS as early as possible and thus allowing for the widest range of therapeutic options, is therefore highly in the patients’ interest, in particular as irreversible axonal and neuronal injury is a key aspect and correlate of disability in MS in early disease stages.3–5
One easily-accessible means of assessing neuroaxonal damage in MS is the investigation of the retina. Optical coherence tomography (OCT) has shown specific retinal alterations in MS patients: 6 the retinal nerve fiber layer (RNFL) is reduced in MS, 7 not only in eyes with a history of ON 8 but also in eyes without any previous clinical event of ON.9,10 Additionally, microcystic macular edema (MME) in the inner nuclear layer (INL) has been reported in a subset of MS patients. 11 Although MME might not be specific to MS, but instead ON-dependent, 12 the INL has become a key focus of clinical investigation of MS pathology after a postmortem histopathology study reported neuronal loss in the INL.13,14
Additionally, retinal changes in MS do not merely reflect the visual system, but potentially also overall disease pathology. RNFL thinning correlates closely with brain atrophy,15–17 and with reduction of N-acetyl-aspartate as marker of neuroaxonal integrity in the visual cortex. 18
These findings suggest that the retina and, in particular, intraretinal layers may be an effective means of detecting subtle neuronal and axonal damage already present in CIS. To investigate this theory, we performed a cross-sectional study analysing intraretinal changes in CIS patients. We were especially interested in retinal pathology in eyes that had not suffered from previous ON and therefore applied a rigorous classification of eyes not only on clinical assessments but also visual evoked potentials (VEP).
Methods
Study participants
Patients were prospectively recruited from outpatient clinics at two university medical centers (Berlin and Düsseldorf). Inclusion criteria were clinical and paraclinical (MRI, CSF, EP) diagnosis of CIS suggestive of MS after relevant differential diagnoses had been ruled out, and an age between 18 and 65 years. 2 Patients received MRI to exclude the possibility that the disease had developed into MS since first diagnosis of CIS. Neurological disability was assessed according to the Expanded Disability Status Scale (EDSS). 19 A history of ON was diagnosed by a treating physician and was cross-checked using medical records. Patients with a refractive error of more than ±5.0 dioptres or with any history of eye disease that could impact OCT measurements (i.e. glaucoma) were excluded. A second exclusion criterion was steroid therapy within 30 days prior to examination. A group of healthy controls matched by age (+/−3 years) and gender was recruited from patients’ family members, medical staff or volunteers. Both centres assessed the matched controls to their patients. To exclude potential centre effects, we additionally performed centre-specific analysis or included centre as covariate. In these analyses, centre did not have a significant effect (data not shown). Local ethics committees approved the study and all participants gave written informed consent.
Visual evoked potentials
VEP were either performed during the clinical work-up or as part of the study protocol prior to or on the same day as the OCT assessment. We used the P100 latency values as a parameter to prove optic nerve conduction slowing potentially related to a history of ON. VEP amplitude was not analysed because the two centres involved in the study performed VEP using different devices in a non-standardized manner.
Optical coherence tomography
Experienced operators performed OCT on un-dilated eyes using Heidelberg Spectralis SD-OCT (Heidelberg Engineering, Germany). All scans were checked for appropriate image quality. All participants were examined using the peripapillary ring scan, which measures RNFL thickness (pRNFL) around the optic nerve head in a circle with an angle of 12°, resulting in a diameter of 3.4 mm (example shown in Figure 1(a)). Macular volume was assessed by a custom scan comprising 61 vertical B-scans (each with 768 A-Scans, Automatic Real-Time (ART) = 13 frames) with a scanning angle of 30° × 25° focusing on the fovea. Using this scan, TMV and intra-retinal layers thicknesses were determined within a cylinder of 6 mm diameter (Figure 1(b)).
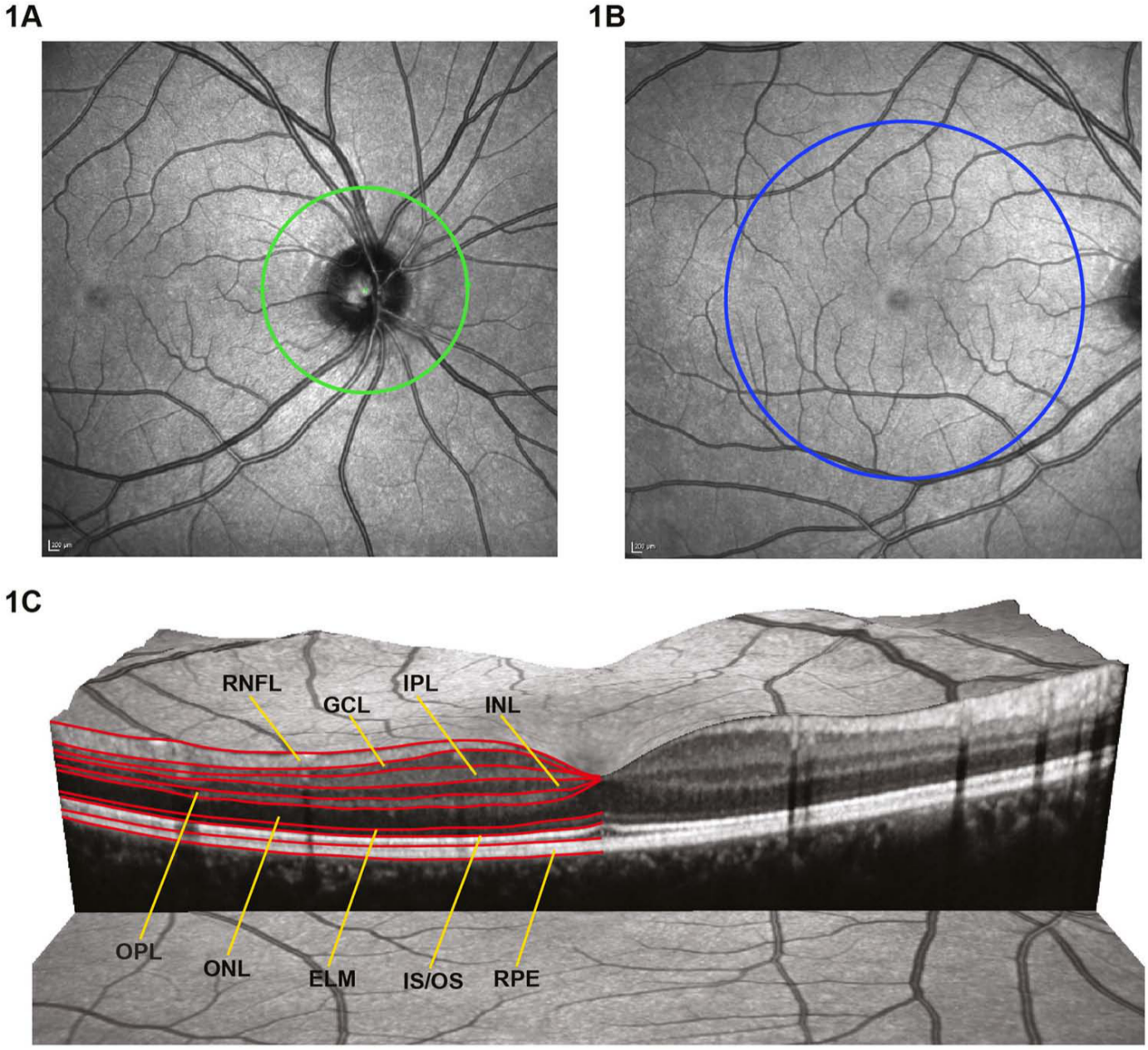
Examples of regions analysed in OCT.
Intraretinal layer segmentation
Heidelberg Engineering provided beta software that employed a multilayer segmentation algorithm for macular volume scans. To analyse the inner retinal layers, a subset of B-scans were segmented and manually corrected by an experienced assessor in a blinded fashion. The multilayer analysis was performed on the central B-scan through the fovea and on six B-scans each in nasal and temporal direction. Manual correction of automatically segmented B-scans is a time-consuming step. As a compromise, we manually corrected every fourth B-scan, thus analysing an area largely covering the 6 mm diameter ETDRS grid with a distance between adjacent B-scans of approximately 500 µm. For the combined analysis of both eyes, thickness maps of the left eye were mirrored vertically to match the topology of the right eye. The mean thickness maps within each of the study groups were calculated for the four innermost retinal layers: macular RNFL (mRNFL), ganglion cell layer (GCL), inner plexiform layer (IPL) and INL (Figure 1(c)). Because differentiating between GCL and IPL proved to be a hurdle, we used the combined thickness of GCL and IPL (GCIPL). Please see the supplementary data for individual analyses of GCL and IPL. By subtracting the group-specific mean thickness maps we produced spatial difference maps (Figure 3), in which negative values indicate a thinning of the patients’ group compared to matched healthy controls, whereas positive values indicated thickening.
Statistical analysis
Generalized estimation equation models (GEE) accounting for within-subject inter-eye effects were used to compare OCT results between the study cohorts. For the subgroup analysis, only controls that were matched to the respective CIS patients’ eyes (NON, SON, ON) were used. Correlations between VEP and OCT results were performed by linear regression. All statistical analyses were performed and all figures were created using R version 2.15.0. Statistical significance was established at p < 0.05.
Results
Study participants
In total, 45 patients (Berlin 29, Düsseldorf 16) were enrolled and compared to matched healthy controls (Berlin 29, Düsseldorf 16). All patients were diagnosed with CIS at the time of OCT examination and diagnosis and non-progression towards MS was confirmed by means of MRI. Of the patients, 16 had unilateral optic neuritis (seven on the right, 10 on the left) and 14 patients presented with spinal cord symptoms. Six patients experienced relapses with findings suggestive of infratentorial brain lesions, in seven patients supratentorial signs were found, and one patient exhibited both supratentorial and spinal clinical signs. Examination of one patient’s eye did not pass the quality criteria due to image artefacts and was excluded. Demographic and clinical data are summarized in Table 1.
Demographical and clinical parameters.
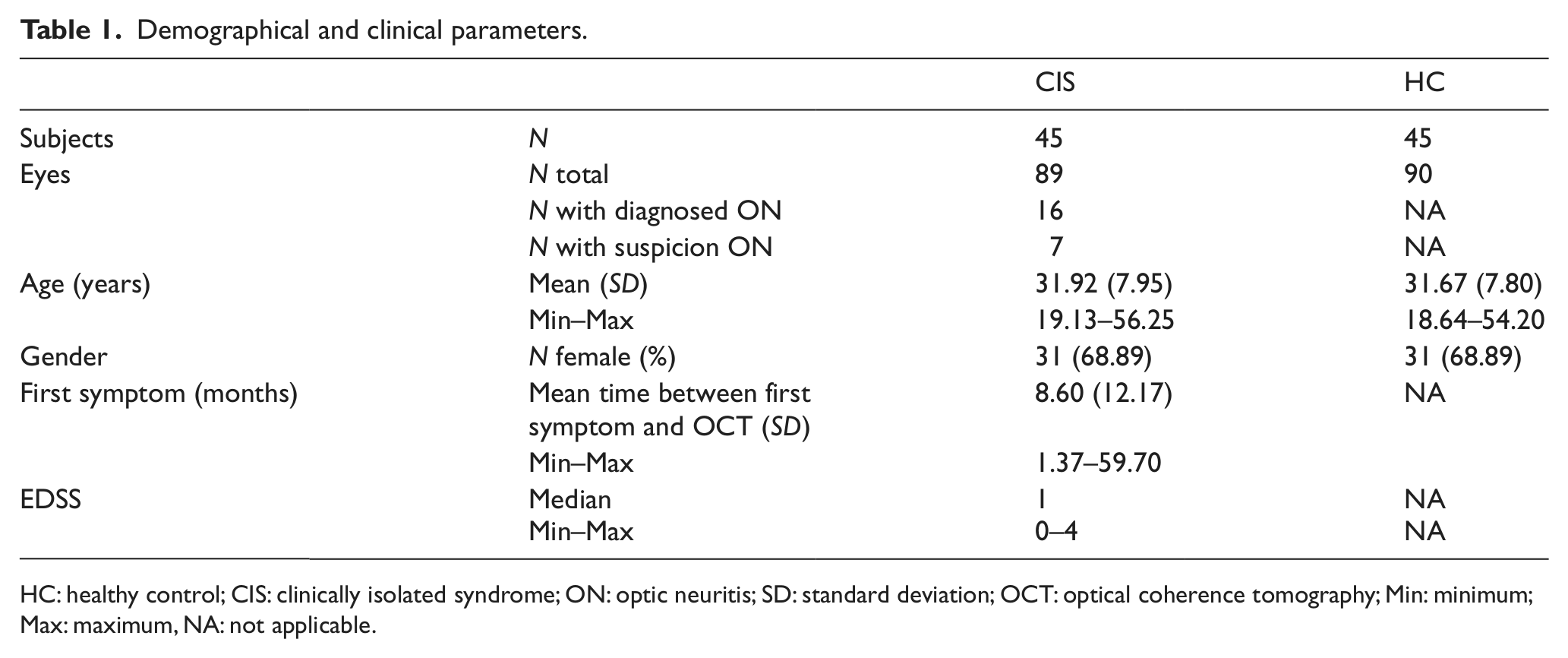
HC: healthy control; CIS: clinically isolated syndrome; ON: optic neuritis; SD: standard deviation; OCT: optical coherence tomography; Min: minimum; Max: maximum, NA: not applicable.
ON classification according to VEP latency and correlation to standard OCT results
As a clinical diagnosis of ON may have been missed by patients or physicians, we created another category of subclinical (or suspected) ON in eyes without a clinical ON history, as assessed by VEP. In addition to the group of confirmed ON eyes (CIS-ON), we defined a group of suspected ON eyes (CIS-SON), defined as eyes with prolonged P100 latency of over 115 ms but, as stated above, without a clinical history of ON. The latter value of a 115 ms limit for normal eyes is in accordance with literature 20 and proved an effective means of distinguishing between eyes diagnosed with ON and unaffected eyes (Figure 2(a) and 2(b)). In total, seven eyes were classified as CIS-SON. Both eyes of two patients were classified as suspected ON and all other CIS-SON eyes were contralateral to CIS-ON eyes. Figure 2(a) shows the correlation between P100 latencies and pRNFL thickness, while Figure 2(b) is a graph of the relationship between the TMV and the VEP results. Linear regression showed significant correlation between pRNFL and P100 VEP latencies in all CIS eyes (R2 = 0.243, p < 0.001) and in CIS-NON eyes (R2 = 0.065, p = 0.039) but not in CIS-SON and CIS-ON eyes. Similarly, TMV correlated significantly to P100 latencies for all CIS eyes (R2 = 0.124, p < 0.001), but not for the other subgroups.
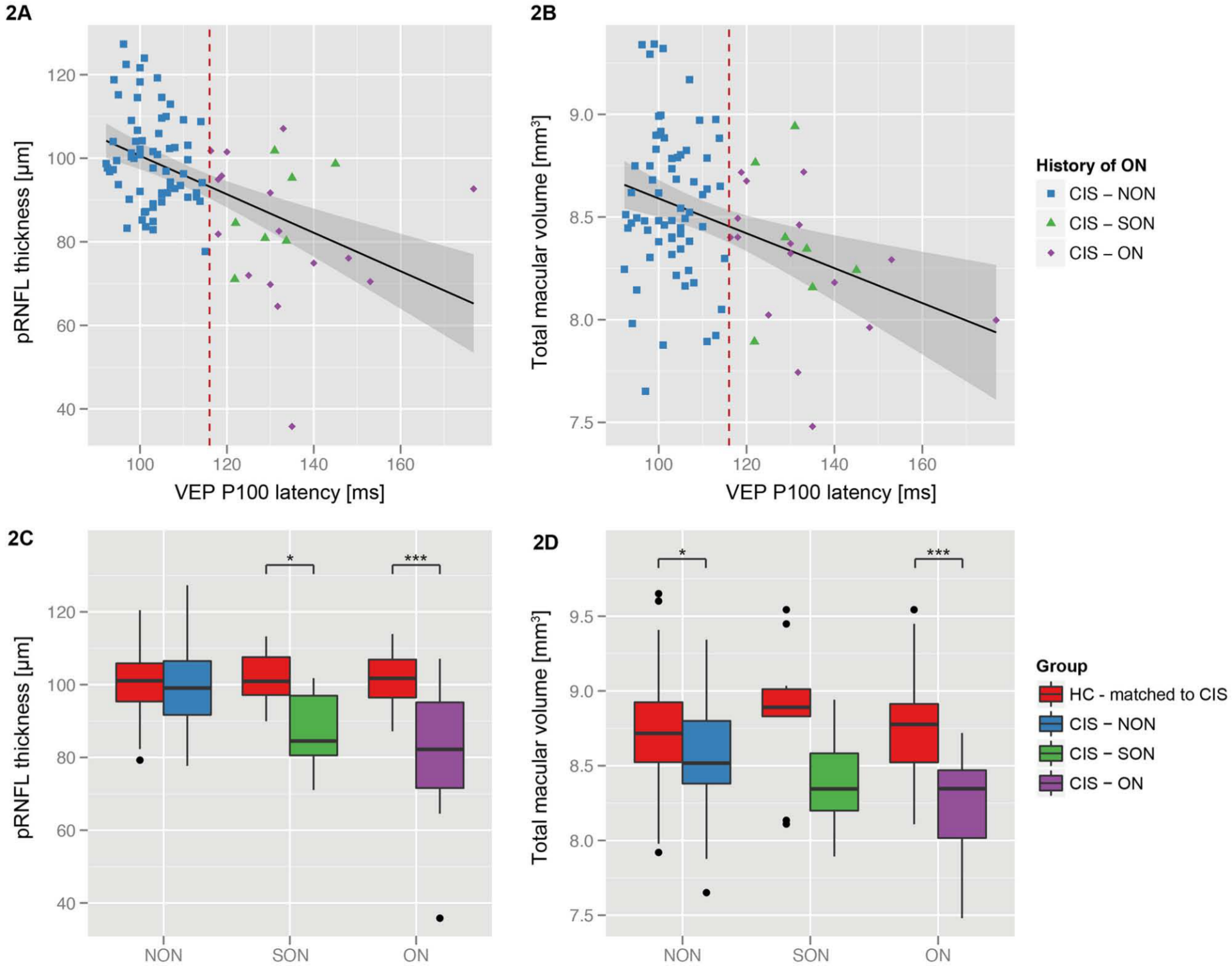
VEP and standard OCT results.
pRNFL and TMV comparison
When compared to the corresponding age- and sex-matched controls, pRNFL thickness was reduced in CIS-ON (p < 0.001) and CIS-SON (p = 0.014) but not in CIS-NON eyes (p = 0.636) (Figure 2(c)). Analysis of macular scans revealed significant TMV reduction in CIS-ON eyes (p < 0.001) and, importantly, also in CIS-NON eyes (p = 0.031) versus controls (Figure 2(d)). TMV reduction in the 7 CIS-SON eyes was not significant.
Intraretinal multilayer segmentation
The mean macular thickness values for inner retinal layers (mRNFL, GCIPL, INL) of the different groups are summarized in Table 2. A graphical representation of the spatial changes of CIS patients compared to the matching controls is given in Figure 3.
Mean (SD) retinal layer thickness and total macular volume results.
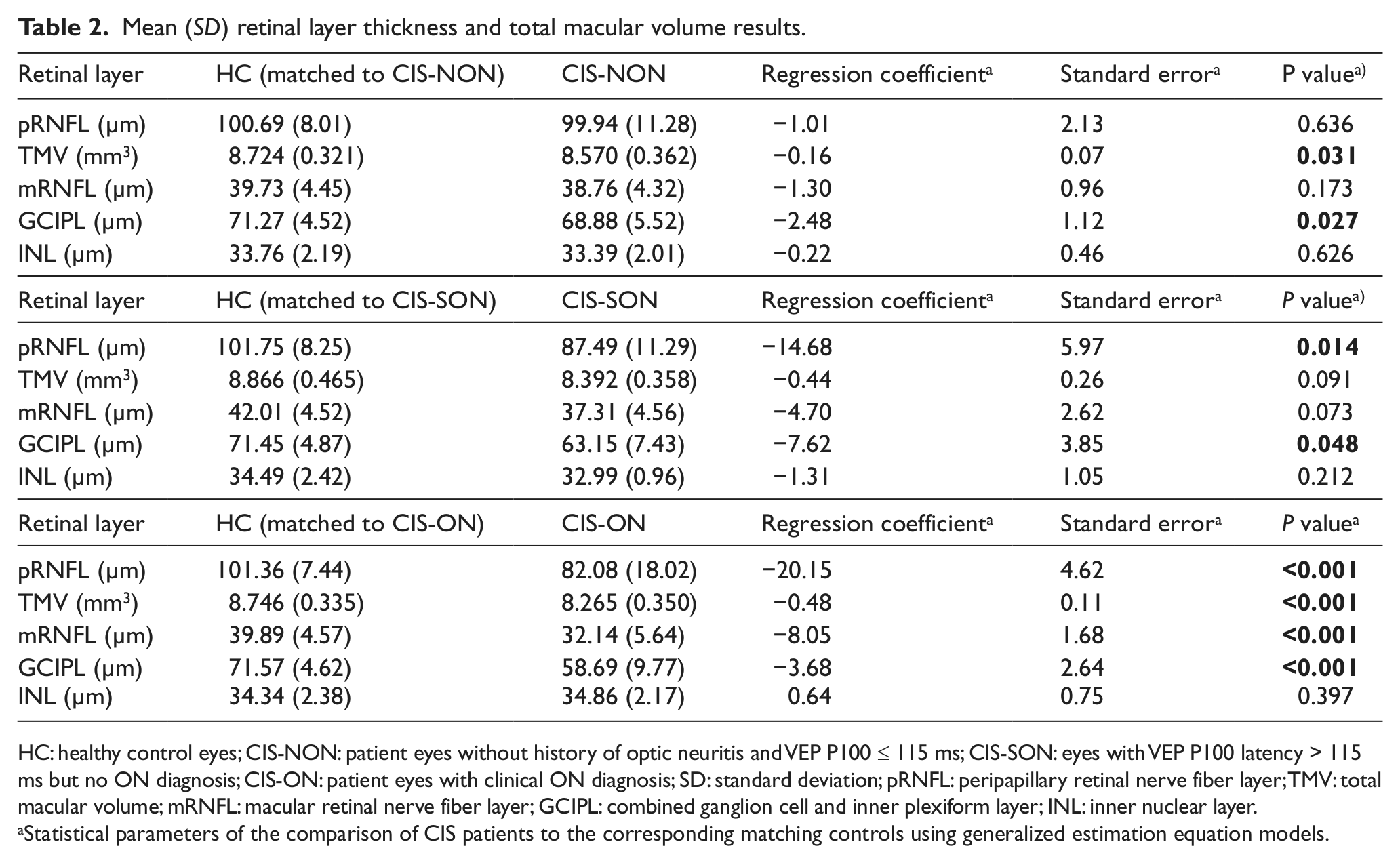
HC: healthy control eyes; CIS-NON: patient eyes without history of optic neuritis and VEP P100 ≤ 115 ms; CIS-SON: eyes with VEP P100 latency > 115 ms but no ON diagnosis; CIS-ON: patient eyes with clinical ON diagnosis; SD: standard deviation; pRNFL: peripapillary retinal nerve fiber layer; TMV: total macular volume; mRNFL: macular retinal nerve fiber layer; GCIPL: combined ganglion cell and inner plexiform layer; INL: inner nuclear layer.
Statistical parameters of the comparison of CIS patients to the corresponding matching controls using generalized estimation equation models.
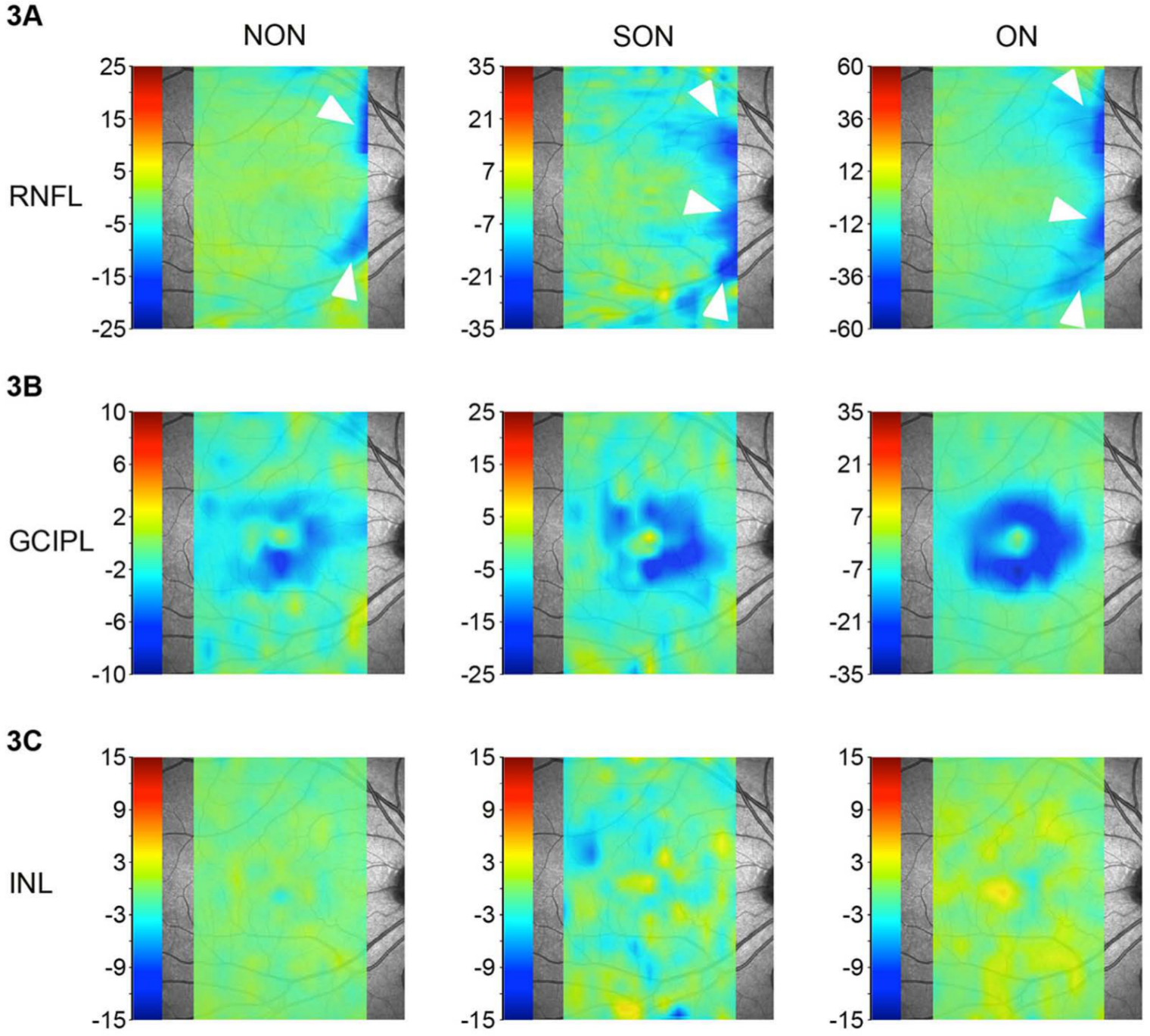
Spatial analysis of changes in CIS eyes versus healthy control eyes.
Analysis of the central macular area (6 mm in diameter around the fovea) showed significant reduction in mRNFL thickness in CIS-ON eyes, but not for CIS-SON and CIS-NON in comparison to matched controls (Table 2). Spatial difference maps showed that mRNFL thinning was most prominent in close proximity to the optic nerve head (Figure 3(a), white arrows). Here, even for CIS-NON eyes mRNFL thinning was visible very close to the optic nerve head. It should be noted that macular volume scans are not designed to investigate the papillary region and that this area is highly penetrated by blood vessels, potentially causing segmentation errors; thus, the mRNFL results have to be evaluated with caution.
All patient groups showed reduced GCIPL thickness compared to the matched healthy controls. Spatial differences of the GCIPL were found in the perimacular region (Figure 3(b)) and statistical analysis of the GCIPL confirmed that the thickness in this area was significantly reduced for all patient groups compared to controls (Table 2). The thinning in CIS-ON and CIS-SON eyes was more pronounced than in the CIS-NON group, while the spatial distribution of changes was similar. Please refer to the supplementary material for detailed data on the analysis of the GCL and IPL individually.
Analogous to pRNFL and TMV, we analysed a potential correlation between VEP latencies and intraretinal layer thicknesses: mRNFL (R2 = 0.203, p < 0.001) and GCIPL (R2 = 0.315, p < 0.001) were significantly correlated to VEP latencies (supplementary Figure 2). There was no correlation of intraretinal layer thicknesses or VEP latencies with symptom onset in the CIS-NON group (supplementary Figure 3).
Discussion
We analysed intraretinal changes in a cohort of CIS patients, which included both eyes with confirmed previous ON, eyes with suspected ON, and eyes without evidence of ON compared to age- and sex-matched healthy controls. Notably, we identified significant thinning of GCIPL in the eyes of CIS patients without any clinical history of ON or suspected previous subclinical ON as determined by VEP changes. A supplementary analysis using distinct GCL and IPL thicknesses localized this GCIPL thinning to the GCL in CIS-NON patients. Additionally, and as expected, eyes with a confirmed history of ON showed an even more pronounced thinning of retinal layers. In contrast, INL appeared unaltered. Our data indicate that retinal neuronal damage can accompany CIS independently of a prior history of ON.
Three previous studies have investigated retinal changes in CIS patients: The first study failed to detect pRNFL or TMV reduction in the eyes of CIS patients without prior ON. 21 A second study reported no retinal damage in the eyes of patients with isolated unilateral ON. 22 However, these studies were conducted before the introduction of spectral-domain OCT (SD-OCT), the superior spatial resolution of which over time-domain OCT (TD-OCT) 23 allows for the investigation of intraretinal layers. 24 Previously and in particular, in the above studies, retinal alterations may have simply not been detectable by TD-OCT and, more importantly, GCIPL changes that can only quantified using SD-OCT might be superior for detecting even subtle neurodegeneration in CIS over pRNFL. Peripapillary RNFL also failed to detect differences in our groups, suggesting that this parameter is in general less sensitive for detecting MS pathology than new intraretinal layer measurements like GCIPL. With this in mind, the failure to detect significant pRNFL alterations in our CIS-NON cohort may simply be a power issue. A third recent study comprising 45 CIS patients showed a reduction of pRNFL but not TMV using SD-OCT. 25
The present study is the first to investigate intraretinal layer changes or detect retinal neurodegeneration independent from ON in a larger cohort of CIS patients. A recent study that reported reduction of the GCIPL in MS patients with and without a history of ON included seven CIS patients while the remaining patients had long-standing diagnoses of MS, which precluded reliable assessment of retinal damage in early disease stages. 26 Other studies have shown INL impairment (i.e. microcystic macular oedema) in MS patients with longer disease duration.11,14 Such changes were not detected in our CIS patients, suggesting that INL impairment might be a symptom of later or more severe disease stages.
Our finding that damage to the GCIPL is detectable in CIS eyes without clinical history of ON and with normal VEP latency lends additional support to the increasingly widespread understanding of MS as both a demyelinating and neurodegenerative disease. 27 We show that neurodegeneration is not, in fact, limited to advanced disease stages, in which it is considered responsible for the continuous progression of neurological disability, even in the absence of relapses. Instead, neurodegeneration can begin very early in disease development. Our data corroborate MRI data showing neuroaxonal damage during the very earliest MS stages,4,28 as well as histopathology data from brain 29 and eye, 13 and from experimental autoimmune encephalomyelitis.30,31 In line with previous investigations, our study provides evidence that inflammatory attacks to the optic nerve to the extent of a clinical or subclinical ON may not be a pre-requisite for damage to the retinal GCIPL. 26
Our finding that neuronal retinal damage begins during very early disease stages raises urgent questions, the answers to which may challenge our understanding of the underlying pathology and mechanisms of MS. 32 Is the damage we found in the retina a consequence of the retrograde degeneration of retinal nerve fibres that occurs as a consequence of autoimmune brain inflammation in MS? If the answer is yes, it follows that retrograde RNFL damage would subsequently initiate a degenerative process in the GCL via a dying back mechanism. Indeed, the hypothesis that retrograde retinal neuroaxonal damage takes place both after ON as well as brain inflammation without clinical ON is supported by experimental animal data from intracranial optic nerve sections. 33 Here, ocular pathology was shown to be limited to the inner retina. Evidence for inner retinal layer damage has been further provided by the first large scale pathological description of retinae from autopsied MS patients showing – apart from the anticipated extensive axonal damage – neuronal loss in both the GCL and the INL. 13 In contrast, a recent OCT study has suggested a primary retinal pathology as a novel distinct subtype of MS, which would implicate that a dying back pathomechanism does not apply to all patients: 24 the study identified MS patients exhibiting substantial reduction of TMV and significant thinning of the outer and inner nuclear layers despite normal RNFL values. The authors suggested that retinal pathology in this disease subtype (termed ‘macular thinning predominant’) occurs independently of optic nerve pathology and may be a harbinger of a more aggressive disease course. However, these findings have yet to be confirmed by other groups and with other OCT devices in larger cohorts. 34
Some important caveats of our study should be noted. Firstly, undetected subclinical ON episodes in our patient cohort may have skewed our results. However, we dealt with this potential cohort bias swiftly by conducting a thorough clinical assessment and examination of the individual patients. Additionally, each patient had to undergo VEP: Eyes with P100 latency suspicious for ON were classified as subclinical ON and not as unaffected eyes. Furthermore, all patients received MRI as proof that a confirmed diagnosis of MS could not yet be established. Although this approach cannot be guaranteed to prevent all errors in ON identification, it does ensure that the risk of misclassification as CIS-NON or MS is negligible and that the conclusions drawn from our data are valid.
A further limitation of our study is that we could not correlate morphological data to functional visual measures such as low contrast letter acuity. However, we are currently addressing this aspect in an ongoing CIS study that includes Sloan charts as suggested by a previous study. 35 The high number of statistical analyses in comparison to the relatively low number of patients should also be noted. As we did not perform a previous power calculation and since OCT parameters are related and thus likely correlated, we did not correct for multiple comparisons, since doing so would have likely caused an overcorrection. We did carefully examine our cohorts for a possible influence of outliers and distribution effects, finding no such effect. However, it is important to reproduce our findings in an independent cohort.
Segmentation of intraretinal layers is a novel technique and no studies have been performed so far to better understand how segmentation-derived results relate to in-vivo morphological changes that appear in MS (e.g. through histopathological studies). However, a number of recent studies have successfully applied intraretinal segmentation,9,14,17,26,36 and comparison of different segmentation techniques showed excellent reproducibility and reliability. 37 We have investigated reliability of the novel algorithm applied in this study in a cross-centre inter-rater reliability study on a defined set of OCT macular B-scans. Results support the excellent reliability of intraretinal segmentation reported by others, 37 with the exception that no histopathological correlation has been performed so far (publication in preparation). However, GCL and IPL are still difficult to differentiate in OCT scans and therefore we based our study results mostly on the combined layer of both (GCIPL) and present individual layer analyses as supplementary data only.
Of note is the large amount of eyes that were classified as suspected ON (n = 7) in comparison to the number of eyes with definite clinical ON (n = 16). Retinal layer-thinning in these eyes was in-between NON and ON eyes, further supporting the notion that optic nerve inflammation is not a yes or no event. Instead, substantial damage might be caused by optic nerve inflammation before clinical visibility in form of an apparent clinical ON might be established. As our cohort comprised only patients with CIS, failure to detect subclinical ON potentially might compromise the discrimination between CIS patients and patients who already have definite MS. Clearly, detection of subclinical alterations in visual and other functional systems urgently needs improvement. Our study did not investigate the discriminatory properties of OCT and VEP between CIS and MS patients, and consequently, this question must be addressed by a future study.
In summary, our study shows that retinal neurodegeneration is already detectable in CIS patients and is dependent but importantly also independent of clinical relapses (i.e. ON). Accordingly, irreversible neuronal damage in MS might be much more prevalent than previously thought. Long-term follow-up of our study patients, who exhibited very early substantial and presumably irreversible neuroaxonal damage, is vital to ascertain diagnosis in patients likely to develop MS as early as possible.
Footnotes
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
This study was supported by grants from the German Research Foundation (DFG Exc 257) and the German Federal Ministry of Economics and Technology (BMWi ZIM KF2286101FO9). The MS center at the Department of Neurology, Heinrich-Heine-Universität Düsseldorf, is supported in part by the Walter-and-Ilse-Rose-Stiftung (to O.A. and H.-P.H.), the Eugène Devic European Network (E-rare/EU-FP7; to O.A. and H.-P.H.), and the German Ministry for Education and Research (BMBF, ‘German Competence Network Multiple Sclerosis’, KKNMS-BMBF; to H.-P.H.). The funding bodies neither influenced the study design, data collection and analysis, nor the decision to publish, and preparation of the manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.