
Abstract
Drawing on interview and diary data from 21 women in the UK, this paper focuses on how endometriosis, a long-term gynecological condition, is lived and navigated alongside paid employment. It discusses the intersectional dynamics of gender, disability, race, and ethnicity to explore how certain bodies are precarized across space and time by the rigid temporal organization of work. We advance existing discussions of precarity by showing how, in the absence of supportive interventions, the embodied precarity of a widely misunderstood and gendered condition with highly variable symptoms can paradoxically make precarious work more suitable because of its purported flexibility. But this creates a double bind of its own, given the well-documented insecurity and lack of clear employment rights which characterizes such work. Theoretically, we develop the concept of endo time as a non-normative temporality located within crip time to highlight its radical divergence from normative ableist and androcentric time and neoliberal labor logic for those working with endometriosis. Endo time advances feminist theorizing of precarity by shedding additional light on bodies at and not at work, those which can and cannot work regularly and consistently; long-term gendered health conditions; and the discursive representation of women’s bodies as leaky, unpredictable, and fragile.
Keywords
Introduction
In this paper, we analyze how living with the embodied precarity of an unpredictable long-term gendered condition interacts with labor precarity and participation. We consider women’s experiences of working with endometriosis as an example of the range of fluctuating long-term illnesses that contribute to precarious worker subjectivities which are also gendered. Whilst this paper focuses on the impact on work, this is clearly not easily separated from other aspects of life such as healthcare, which has remained stubbornly gendered with poor funding for women’s health (Fisk and Atun, 2009; Philbin et al., 2024). As such, we identify the intersectional layers of precarious subjectivities that are mutually produced and reinforced for people with endometriosis and likely also for those with other long-term gynecological conditions.
Using the lens of feminist disability theories of embodied precarity (Shildrick, 2019) and crip time (Kafer, 2013, 2021), we examine the precarious embodiment of living and working with endometriosis, and how in turn this precarious temporality is cripped. Whilst crip is a political reclaiming of the derogatory label “cripple” as popularized in disability theory and activism (Fazeli, 2016), crip theory interrogates the ways in which neoliberal capitalism contains and constrains disability within the context of compulsory able-bodiedness (McRuer, 2006; Napolitano and Sicca, 2024). From a crip theory perspective, Kafer (2013, 2021) developed the concept of crip time to refer to the unpredictable, non-linear and non-normative day-to-day negotiations and ever-shifting temporalities of being disabled. In this reading, disability is created by social barriers as opposed to it residing in the body; it “is something imposed on top of our impairments” (Finkelstein, 2001: 1) by exclusionary environments and social structures. As such, crip time is an understanding of time that disturbs the structural barriers of normative ableist regimes (Kafer, 2013).
We extend the concept of crip time by contributing the distinctive notion of endo time as an endometriosis-specific shifting temporality. In so doing we recognize its significance for labor market participation. Our conceptualization of endo time also expands existing discussions of precarity as being caused by external and embodied factors, and points to precarity generating considerable challenges for women with endometriosis and other long-term gendered health conditions, at work and elsewhere. Unlike crip time as a broader concept, endo time is gendered and associated with a condition which in and of itself is highly variable. This is important because, although it is a relatively common disease—the best available estimate suggests that 190 million cis women worldwide live with endometriosis (Zondervan et al., 2020)—it almost exclusively affects people who menstruate (there are vanishingly small numbers of cis men with confirmed endometriosis lesions). As a result, at least as we see it, it is widely misunderstood and profoundly under-diagnosed. Endometriosis is also characterized by its unpredictability, which marks it out from other long-term conditions whose symptomatology is typically more consistent. Endo time is gendered as it is embedded in a patriarchal system which has traditionally neglected the study and treatment of women’s health (Fisk and Atun, 2009; Philbin et al., 2024). This is due to the androcentrism of medical knowledge, which is grounded on less fluctuating (i.e. no menstrual cycle) and more stable cis male bodies (Hudson, 2022). Consequently, the result is an enduring gender health gap whereby women’s symptoms (and those of other bodies who do not fit with the cis male norm) that cannot easily be explained by medical science have been dismissed or considered psychosomatic (Hoffmann and Tarzian, 2001).
Endo time is embedded in feminist concerns and aims at disturbing dominant conceptions of knowledge and practices of inquiry that disadvantage women and other marginalized groups. Specifically, endo time advances feminist theorizing of precarity by exposing how lived experiences of endometriosis have been excluded and denied epistemic authority within the realms of health and the work environment. The knowledge that the concept of endo time produces becomes useful to people in marginalized positions and reinforces the feminist objective of situating the research investigation within the perspectives of the minoritized subject. For instance, endo time is situated within participants’ knowledge and understanding of “the conceptual practices of power [. . .] through which their oppression was designed, maintained, and made to seem natural and desirable to everyone” (Harding, 2004: 5); and, thus, how their precarity is shaped and exacerbated within unaccommodating workplace environments. As such, this paper challenges cultural norms about work and workers and structures of inequality embedded within the organization of work, whilst identifying solutions for intersectional gender equality in the workplace for those working with endometriosis and other gendered long-term health conditions.
Endometriosis, on average, takes 8–12 years to be diagnosed (Kiesel and Sourouni, 2019). It occurs when tissue resembling the lining of the uterus develops in other areas of the body, such as the ovaries, bladder, bowels, and lungs (Alifano et al., 2006; Tomassetti et al., 2021). Each month when this tissue breaks down and bleeds as part of the menstrual cycle, it remains trapped inside the body, leading to inflammation and adhesions (Bloski and Pierson, 2008). The fluctuating, unpredictable and debilitating symptoms this causes - including chronic pelvic pain, heavy bleeding, extreme fatigue, bladder and bowel problems, depression, and anxiety amongst others (Becker et al., 2022; Lemaire, 2004) - restrict the ability to work the regular pattern of a traditional working calendar. Indeed, when symptoms are at their worst, women with endometriosis can experience a loss of up to 15.8 employment hours per week (Soliman et al., 2017). In the UK, this is estimated to cost £5757.72 per employed person with endometriosis and £8.2 billion to the economy annually (Simoens et al., 2012). This is exacerbated by the fact that, as suggested above, endometriosis is a significantly under-researched and under-funded health condition and that it carries the stigma of its relationship to menstruation. Endometriosis can also affect anyone assigned female at birth; whilst our research examines the experience of cis women, we fully acknowledge the experience of intersex, transgender, and gender nonconforming people who are also balancing the embodied precarity of endometriosis with employment.
The paper begins with a discussion of precarity, embodiment, and crip time. It then discusses the challenges of balancing cripped temporalities of endometriosis with employment. The methodology is outlined afterward, followed by a findings section where we develop the theoretical concept of endo time. Finally, we summarize how endo time illuminates the challenges of balancing the embodied precarity of endometriosis and the need to operate in non-normative temporalities against neoliberal expectations at work that position unpredictability as problematic. This has consequences for the identities of those with the condition, specifically around their self-esteem, self-confidence, and sense of futurity—of being able to accumulate sufficient resources, construct egalitarian relationships and be certain about their futures. Additionally, we highlight the value of flexible orientations to time when navigating embodied precarity and how individuals may turn to precarious work in their absence. We show how precarious working conditions can be emancipatory in a biopolitical sense for some individuals with endometriosis, whilst others find themselves even less supported and protected. In this section we also emphasize how the various forms of precarity associated with endometriosis are worsened by Fricker’s (2007) epistemic injustice; in other words, and precisely—we believe - because it is a gendered condition, those with endometriosis are commonly not taken seriously when they report their symptoms to others and there is a paucity of discursive resources to interpret their experiences. The paper concludes by offering some implications for organizations and suggestion for further research.
Precarity, embodiment and crip time
Precarity is often understood as emerging from socioeconomic vulnerability (Kalleberg, 2009), such as the exploitative practices of atypical, casual and insecure employment as experienced by freelance, migrant, agency and gig economy workers. However, its conceptualization extends beyond this epistemological positioning as a labor or class category. Precarity also denotes a generalized state that is synonymous with human existence (Millar, 2017). All bodies are vulnerable, or precarious, to a certain extent as we are always susceptible to aging, accidents, or disease. For Butler (2004), however, precarity extends yet further. They theorize it as the unavoidable ontological vulnerability that is a condition of our relationality and the “social bonds that support life” (in Puar, 2012: 169). Butler (2009) insists on a distinction between precariousness and precarity; the latter arising from the differential distribution of socioeconomic and political vulnerability in oppressive societies. As they put it, precarity is a “politically induced condition in which certain populations suffer from failing social and economic networks of support and become differentially exposed to injury, violence, and death” (Butler, 2009: 4). Berlant agrees that precarity is, simultaneously, existential, structural, embodied, pervasive, relational, and political (in Puar, 2012). In other words, it is part of living in conditions of fundamentally inadequate social connectivity as well as being an inescapable characteristic of the human body.
Precarity therefore becomes “the individual predicament of vulnerable subjects” to overcome (Mery Karlsson and Rydström, 2023: 400): it “produces not only subjects, but also ‘insecurity’ as the central pre-occupation of the subject” (Lorey, 2015: np). Everyday precarity is experienced through the material struggles that affect some social groups more than others, such as working women’s use of food banks (Spellman and McBride, 2023); the much higher numbers of members of the global majority who involuntarily lose or are forced to leave their jobs compared to white people (Kalleberg, 2009); women’s unpaid household labor (Office of National Statistics, 2016); poorly rewarded feminized jobs (Perez, 2019); the lived experience of migrants and their precarious citizenship (Banki, 2013; Simola, 2018); and long-term work and income insecurity for older workers (Lain et al., 2019). It is also inextricably linked with subjectification and agency (Puar, 2012), as illustrated by Hancock and Tyler’s (2024) exploration of live performers’ experiences during COVID-19. They detail how socioeconomic precarity can create profound uncertainties around identity. Whilst the pandemic exacerbated the structural inequalities in an already precarious sector of employment, these material conditions set against the backdrop of canceled events brought the equally precarious sense of recognition and self-esteem that these performers derive from their work into sharp relief.
Following Berlant’s multi-faceted definition of precarity (in Puar, 2012), embodied precarity is equally tangled up with socioeconomic and subjective precarity. People with endometriosis, the focus of our study, are already physically vulnerable due to the vicissitudes of their long-term and uncurable condition. But their embodied precarity refers not only to such “fundamental corporeal vulnerability” but also its “relationship to wider socio-political conditions and interdependencies” (Earle et al., 2022: 2056). Embodied precarity is therefore also socially intensified. For example, Rice et al. (2023) explore how “episodic disabilities,” a term they use to refer to symptomatically fluctuating health conditions like HIV/AIDS, diabetes, epilepsy and chronic fatigue syndrome, are both “produced in” and simultaneously “pushed out” of the neoliberal university (p. 1734). Importantly for our purposes here, endometriosis could certainly be categorized as an episodic disability. Rice and colleagues, all of whom identify as disabled, use self-produced videos produced to surface experiences of embodied precarity marked by unpredictable experiences of health, in a context where the emphasis is instead “on accommodating stable, enduring disabilities, while provisions for illnesses generally assume that they are time-limited and non-recurring” (p. 1726). However, many disabled academics also face socioeconomic precarity in having to navigate fixed-term, insecure contracts. These forms of precarity are, at the same time, profoundly responsibilized, because the intensely pressured higher education environment means that “disability-coded academics [have to] split ourselves into pieces, hiding the messy, unruly, bruised, and injured parts, and avoid expressing hurt or complaint” (p. 1732).
Cheded et al. (2023) also show this neoliberal logic of self-responsibility when they analyze the complexities of navigating health uncertainties for women who have been identified as genetically vulnerable to developing breast cancer. Their research on an online collective of such “previvors” revealed membership expectations are “framed within a broader socio-moral order [. . .] fueled by the logics of responsibility of self-care and preservation of the body” (p. 58). As such, and even within this collective space of care, the neoliberal discourse of self-management and self-dependency individualizes the responsibility of embodied precarity. Shildrick (2019: 596) argues this is characteristic of the experience of disability in “ordinary lives [that] simply persist in a worn-down state without ever getting better.” Connected to the arguments above around inadequate social connectivity is the shrinking role of the welfare state and healthcare system, which once enabled us to care for one another and that under neoliberalism structures are increasingly undermined (Segal, 2023). Correspondingly, Butler (in Puar, 2012: 170) suggests that “precarity is indissociable from that dimension of politics that addresses the organization and protection of bodily needs. Precarity exposes our sociality, the fragile and necessary dimensions of our interdependency.” Embodied precarity can therefore be positioned as transcending the boundaries of not only individualism and self-dependency but also normative embodiment. As such, it is often a marker for socioeconomic exclusion (Shildrick, 2009).
Embodied precarity also creates non-normative temporalities, as exemplified by Kafer’s (2013) concept of crip time. Crip time diverges from ableist time and unravels the social construction of ability. Operating on crip time “involves an awareness that disabled people might need more time to accomplish something or to arrive somewhere” (p. 26). It is not just an extension of time but a reorientation to time where flexibility is essential (Price, 2011). Kafer (2013: 27) expands on this: Crip time is flex time not just expanded but exploded; it requires reimagining our notions of what can and should happen in time, or recognizing how expectations of “how long things should take” are based on very particular minds and bodies. Rather than bend disabled bodies and minds to meet the clock, crip time bends the clock to meet disabled bodies and minds.
Samuels (2017: np) argues crip time is the recognition of “time travel” because “Disability and illness have the power to extract us from linear, progressive time with its normative life stages and cast us into a wormhole of backward and forward acceleration, jerky stops and starts, tedious intervals and abrupt endings.” As such, this concept offers an understanding of how people with impairments, including those with long-term illnesses, experience the temporality of embodied precarity throughout their everyday efforts to survive, resist, and transform exclusionary environments.
Navigating non-normative temporalities will therefore be a recognizable experience for people with gendered long-term conditions, like endometriosis, who are embodied in precarious ways with unpredictable and fluctuating symptoms, long diagnostic delays, limited treatment options, inadequate state protections, and no cure (Denny and Mann, 2007; Di Guardo et al., 2019; Kiesel and Sourouni, 2019). Bodies with such conditions are made yet more precarious through operating in crip time, by androcentric medical spaces, hostile governmental policies and – our specific focus here - unaccommodating workplace environments (Bend and Priola, 2023). The constant fluctuation or regular irregularity of good days and bad days and living without a cure within socially disabling discursive practices can be extremely debilitating (Charmaz, 1993; Kafer, 2013).
Here we bring together the multi-faceted concept of precarity with processes of precarization and a gendered subset of crip time - endo time - to theorize the particular experiences of UK-based women working with endometriosis and how these are characterized by a set of non-normative relationships to the temporal regimes of employment in neoliberal organizations. This allows us to unravel the significant challenges of:
(a) regularly irregular embodiment and temporal disabling as against the demands for constant productivity;
(b) waiting and weighted time, wherein extended diagnostic delays and a culture of persistent disbelief in gendered and racialized pain amongst medical professionals create additional burdens, for example when workers are unable to sufficiently document their condition in order to take sick leave; and
(c) trade-offs and time travel, which our participants often engaged in to offset the difficulties indexed above, but which brought complexities of their own around opting for precarious forms of employment to enable them to better manage their endometriosis.
All of this also foregrounds considerable additional labor which working people with endometriosis engage in as a matter of course so that they can continue to earn a living.
Next, we discuss the challenges of balancing employment and the embodied precarity of endometriosis, with its effects on productivity and quality of working life.
Endometriosis and employment
The embodied precarity of endometriosis, with its unpredictable and debilitating symptoms, can negatively affect people’s jobs, careers, and economic prospects (Dudley et al., 2017). This is because of the normative expectations of employment under neoliberalism—being able to work as and when required, and always delivering high levels of productivity. In contrast, people with endometriosis often cannot work long hours or need to take increased sick leave (Denny, 2004; Mortimer, 2002; Sperschneider et al., 2019) due to workplaces being designed around an able-bodied norm (Remnant et al., 2023). Equally, they are often excluded from working in their desired occupation and have to take health-related limitations into consideration in their career decisions (Sperschneider et al., 2019). Research shows the relationship between endometriosis and shortened or interrupted careers (Armour et al., 2022). Those with endometriosis are at greater risk of job loss, falling into unemployment, being involuntarily pushed into part-time work, or “choosing” to become self-employed (Gilmour et al., 2008; Moradi et al., 2014). Indeed, of 7025 women with endometriosis from 52 countries, 41% had become unemployed (Hummelshoj et al., 2006). These are strong indicators that employers neither understand nor support the working lives of people with endometriosis. It is therefore unsurprising that they experience lower salaries, as well as a higher risk of leaving the workforce altogether, compared to people of the same age without the condition (Estes et al., 2020).
We recognize that these experiences are shared by people with other long-term conditions, many of which are not gendered, such as multiple sclerosis, arthritis, and epilepsy (Rice et al., 2023). However, as previously suggested, our position is that because endometriosis is a gendered condition associated with menstruation, it is especially poorly understood and much more likely to be dismissed by medical professionals, employers and line managers alike as “just bad periods.” Such widespread misunderstandings of female health are perpetuated by the aforementioned gender gap in medical research funding. For example, although there are a comparable number of women living with diabetes as endometriosis, if endometriosis were to be funded by the NIH at the same level as this non-gendered condition (assuming half of the budget for diabetes were allocated for female sufferers), endometriosis funding would increase 16 times—from $16 million–$250.40 million annually (Ellis et al., 2022). Consequentially, the long-term, misunderstood, un(der)diagnosed and un(der)treated pain this epistemic gap creates increases a person’s precarity, often by causing them to lose or leave their job.
Alongside symptoms and the financial burden of the disease, people with endometriosis can face the socially debilitating effects of a long-term and invisible illness at work. The stigma and low awareness associated with the condition often create a predicament about disclosing symptoms, which may drive workplace accommodations but also fuel discrimination (Dudley et al., 2017). Typically, long delays in diagnosis exacerbate the latter because the lack of official clinical evidence can result in a medical issue being treated as a performance management issue. Although employers often require medical diagnosis to implement workplace accommodations, such evidence is not mandated by the UK Equality Act for that purpose (GOV.UK, 2010). This is because, depending on its severity, endometriosis can meet the criteria of disability under the Act defined as a ““physical” and/or “mental impairment that has a ‘substantial’ and ‘long-term’ negative effect on [the] ability to do normal daily activities” (GOV.UK, 2010: np). Many employers are therefore failing in their legal responsibility to provide reasonable adjustments, whilst reinforcing the medical model of disability which casts the “disabled” body as flawed or less able than the “normal” body. This results in limited access to appropriate workplace support and places employment status in jeopardy (Jones et al., 2004). In other words, endometriosis can create embodied precarity in the labor market and within individual organizations for those who have the condition, regardless of the jobs they do, in similar ways to Rice et al.’s (2023) episodic disabilities.
Thus, here we focus on the social construction of the embodied precarity of endometriosis as disabling in the labor market. Experiences of endometriosis and employment remain a very under-traveled topic and, where research exists, it is typically quantitative (for an exception, see Sang et al., 2021). Our paper addresses this by focusing on how the non-normative temporalities of endometriosis are navigated in an employment context using a multi-method qualitative approach. Workers with other gynecological conditions with overlapping unpredictable symptoms may experience similar challenges (Remnant et al., 2023). Like endometriosis, these conditions are characterized by unpredictable symptomatology and have no cure. Our empirical study addresses the question of how time and temporality matter for women’s embodied experiences of endometriosis and employment.
We now set out our methodology before discussing the study’s findings.
Methodology
We draw on empirical data from a qualitative study of 21 women working with endometriosis in the UK, undertaken by Victoria for her PhD thesis. Participant recruitment was carried out online through social media, including by endometriosis charities, women’s health networks and activists, and individuals with endometriosis. Interested participants were asked to report their gender, age, ethnicity, sexual orientation, location, job title, industry, and to say whether they had any other condition(s). Selection was carried out on the basis that they had a medical diagnosis of endometriosis (a requirement of The Open University’s ethics procedure) and that they worked in the UK.
Potential participants were grouped by employment sector and then selected within each group to facilitate a more diverse sample in relation to ethnicity and age. This allowed an interrogation of intersectionalities in these women’s experiences. Full details of the purpose of the study and the participants’ rights were provided to those included in the study. Participants consisted of women between the ages of 19–49 working across 21 different sectors within the UK, taking account of second jobs. Seventeen identified as white British, Scottish, Welsh, or Irish, two as Asian British, one as dual heritage and one as black British. A list of participants, all of whom have been given pseudonyms, and their biodata can be found in Table 1. Identifying details have been deliberately kept to a minimum to protect their anonymity. The study was approved by The Open University’s Human Research Ethics Committee.
Research participants.
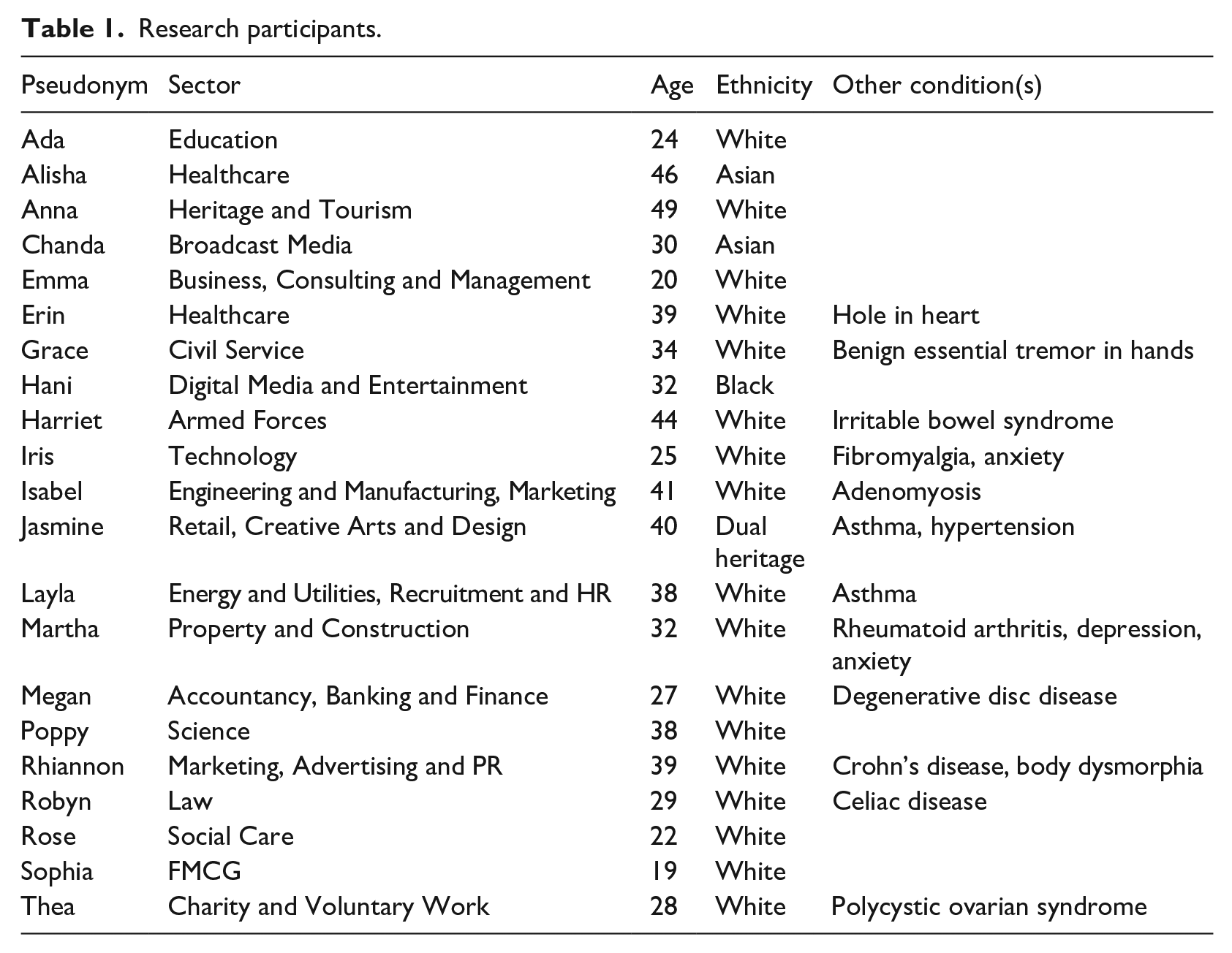
The study focused on exploring how people in the UK labor market experience working with endometriosis, through semi-structured interviews, a diary, and the diary-interview method (Zimmerman and Wieder, 1977), in that order. This multi-method approach contributed to understanding experiences of endometriosis across time. For example, open-ended questions in the first interview generated discussions of past experiences of working with endometriosis, including emotions, feelings, and motivations as they changed over an individual’s career trajectory, in response to global events, including COVID-19, the Black Lives Matter movement, and employment transitions, as well as future aspirations and anxieties around balancing a long-term illness with work. The diary element provided a useful record of an ever-changing present (Allport, 1943). Participants were asked to record entries for 2 months, which were then reflected upon in the subsequent diary-interview. Because we wanted to capture present lived experiences, we specifically set out to recruit only women who were in work. Further research should extend the study to women who stopped working due to their symptoms or their experience of managing symptoms at work. As endometriosis fluctuates in severity and is stigmatized by social norms as related to menstruation, the diary method was also deemed useful to reclaim contextual insights that may otherwise be muted or forgotten as time passes. Timely recording within diaries, as opposed to providing a retrospective or retelling “all of a piece” within interviews, was intended to enable participants to detail experiences as they unfolded. Many participants were already familiar with using apps to track their menstruation or pain levels to make plans and manage their work schedule and workload. However, keeping the diary allowed them to realize not only how many days a week they were in pain or “felt foggy,” but also how often they were mistreated at work, in many different ways. Reading their diary, for some, corresponded to greater awareness of the wider impact of their condition. In the follow-up interview some participants constructed this as a form of temporal agency against capitalism’s temporal bullying.
The use of a multi-method approach generated a rich portrayal of people’s past, present and future experiences of, perspectives on, and feelings about working with endometriosis. In the first stage, 21 participants were interviewed, of these, 16 recorded diary entries, either using a Word document or a mobile diary app called Indeemo; 11 of them took part in a second interview. The first interviews ranged between 36 and 110 minutes, with an average of 64 minutes and the second ranged between 14 and 75 minutes, with an average of 37 minutes. All interviews were recorded and transcribed verbatim, and all transcripts were anonymized to remove identifiable details including the names of participants and their organizations.
Reflexive thematic analysis
Aligning with a poststructuralist epistemological position (Davies and Gannon, 2005) that assumes multiple socially constructed and contested realities, Victoria used reflexive thematic analysis (RTA) to analyze the data (Braun and Clarke, 2019). This allowed her to explore the experiences of people working with endometriosis while understanding the meanings participants ascribed to their experiences, but also to distinguish how her positionality was influencing the analysis. Analysis began by noting interesting aspects during data collection, continuing during transcription and whilst re-reading the transcriptions. In line with RTA, reflective note-taking was used throughout the analysis as a way to document and develop awareness of Victoria’s positionality.
An abductive approach was applied to coding which supported the identification of largely unstudied experiences surrounding endometriosis and employment in the UK; experiences that also remain untheorized. During the coding process, three patterns were identified across the data: (1) the constant pressure to minimize sick leave so as not to trigger punitive absence management measures; (2) the sense that there were no adequate workplace policies or processes to support workers with endometriosis; and (3) that they “fell between the cracks” which existed between absence policies, wellbeing resources, flexible working policies, and so on. These codes were eventually encompassed into our overarching theme of temporal disabling.
Moving iteratively between data and literature, Victoria identified what she saw as the theoretical gap of endo time, conceptualized in the Findings section. Themes were subsequently generated by identifying patterns of meaning around prevailing shared experiences. We understand prevalence as the frequency with which themes appeared across the data set, but also the importance of what each theme captured in relation to the exploration of endometriosis and work. As suggested in “Precarity, embodiment and crip time” above, four themes were identified: regularly irregular embodiment; temporal disabling; waiting and weighted time; and trade-offs and time traveling trajectories. To illustrate one of these themes, Jasmine commented that, after moving to the UK, she had to “to start all over again, to be with doctors who ask you terrible questions like ‘are you sure the pain is internal? Maybe it’s because of something else’.” Here she refers to the fact that her UK doctors would not accept the endometriosis diagnosis she had been given in her country of origin. This we classified under the waiting and weighted time theme.
We should add that our team encompasses a range of perspectives on endometriosis, with two members having lived experience of the condition and one experiencing additional long-term conditions, and all occupying feminist research positions with interests in women’s health and experiences in the workplace. We feel such insights contributed an additional level of understanding of participants’ experiences. However, it is also important to acknowledge that we are white, heterosexual, cis female academics, which limits our understanding in other ways. Therefore, when arriving at our analytical conclusions, we adopt an intersectional reflexivity, “engaging in more nuanced reflection that considers how intersecting socially constructed categories of difference are mobilized” (Rodriguez and Ridgway, 2023: 1273).
We now turn to our findings.
Findings
This section explores interview and diary data by presenting the findings organized according to the four themes identified in the analysis.
Regularly irregular embodiment
Participants’ challenges in navigating endometriosis alongside work emerge from the intersection of their precarious embodiment and operating in crip time. The day-to-day negotiation of regularly irregular symptoms creates profound uncertainty and vulnerability in contexts that do not support such unpredictable shifts in embodiment. Iris shares the existential difficulties of fluctuating symptoms in her everyday life: On a regular basis [. . .] my pain is like a dull ache or like a humming in the background [. . .] It’s painful, but [. . .] it’s manageable with pain medication [. . .] My fatigue is at a level that I can manage, so I can still do other activities and I can still work out and I can still commute to work and things like that. But if I have a flare, the cramps that I get [. . .] they’ll become really, really extreme cramps that are consistent for hours and hours, sometimes days. And I’ll be bloated constantly. So, it will be [. . .] hard for me to eat. My fatigue will go through the roof, so I struggle to get out of bed or do anything other than just working. And I can’t think about anything but the pain, and the painkillers don’t help at all.
Embodied and existential precarity is deeply entangled with and intensified by gender, health and pain gaps (Carneiro, 2024). Women are disproportionately affected by pain but also receive inadequate pain management treatments, as Iris recounts. Such neglect has contributed to the damaging (re)production of discourses that normalize debilitating pain as an experience of the menstrual cycle. Harriet also describes her pain as “sometimes [lasting] for half an hour and just [being] a niggle and other times it’s really horrible for hours.” Embodied precarity for her is written into the everyday through the uncertainty of how long the pain will last and how severe it will be; her daily pain must be endured against a backdrop of inadequate societal recognition and medical treatment. Harriet adds: I went back to [a] leading [hospital] for endometriosis. And [. . .] they said, ‘well, your scans, your MRI scans and x-rays, aren’t showing it’s come back. So therefore we think it’s still under control’. And yet, in my mind, I’m thinking ‘it really isn’t, but you’re not listening to what I’m saying [. . .] I know that I’m in pain or I know that things aren’t right’. And then you begin to feel like you’re a hypochondriac or it’s in your head that you kind of go round and round in circles at that point. And I find that really difficult.
Harriet experiences profound vulnerability when she fails to be seen or have her pain recognized by medical professionals. Endo time, as a strand of crip time, specifically deals with this invisible aspect of the multifaceted temporalities of endometriosis. Harriet’s body is further precarized in how it is understood, treated and managed in a society that undervalues women’s health. Such lived experience that is routinely dismissed in favor of visible evidence of the disease produces vulnerable subjectivities by raising complex questions around identity and self-esteem. It can create experiences of non-citizenship because suffering is trivialized due to its differential moral and political weighting (Bloom, 2020). As such, individuals are often left without adequate resources to address regularly irregular symptoms and this can infiltrate all aspects of their life, especially work.
Robyn, likewise, expresses how her fluctuating symptoms can have a dampening effect on her ability to perform work tasks to normative expectations, which can be seen as embodied precarity: I have really bad pain days, but some days I’m not in pain at all. And that means that the way my symptoms affect my work isn’t consistent throughout any kind of week or month-long periods. But it means that, on the days when I’m in pain, I know I make more mistakes. I have to put in a lot more time into proof-reading what I’ve done. I find it a lot harder to concentrate if I’m in pain [. . .] I think I feel fatigue quite a lot as well. I think that makes me work a bit slower [. . .] I think it contributes to longer hours as well actually, when you know if I’m asked to proof-read a document on a good day, I can do it in an hour. On a bad day, it can take me like twice that time.
During symptomatic flares, which are already characterized by feelings of fragility, pain, and fatigue for Robyn, there is also an expectation placed on her to make up time to perform consistently and deliver against the norm. The extra time she invests points to the exploitation of certain bodies by mobilizing people operating in non-normative temporalities toward productivity as opposed to reducing their exposure to further harm and illness (Kafer, 2021). This exploitation further extends embodied precarity for an already oppressed social group in having to deal with stress and, in turn, the damage this does to their bodies. Grace explains: I am conscious that stress is not a good thing, and I am conscious that whilst I don’t want to say this is the cause, but I just spent the last three years working on [two projects] right at the heart of government [. . .] where everything’s urgent and everything’s for [department name] and working in that environment [for] long periods of time is not great for stress levels and stress levels are not great for endometriosis. I don’t know whether that contributed to my appendix bursting off the back of it.
Grace’s experience shows how multiple forces of precarity can impress upon the body. Here neoliberal capitalist working practices, expectations of keeping up with normative ableist regimes, lack of infrastructural workplace support for people living in non-normative temporalities, and the denial of stress as a health issue can exacerbate existing conditions. Such active neglect of experiences of endo time means that individuals must persist despite unethical and unsupportive working practices whilst their bodies become worn out (Shildrick, 2019). This exposes the vulnerability disproportionately afforded to people with endometriosis in their everyday struggles to keep up appearances, especially at work. We detect the same kind of phenomenon in Alisha’s diary entry about her colleague “getting the ‘royal treatment’” because of her pregnancy, whilst Alisha has “no choice but to carry on in pain and discomfort physically, cognitively, and psychologically without any special office set-up, and [I] sadly may not be able to have a child because of my condition.” Here the contrast between the normative temporality of pregnancy and the non-normative temporality of endometriosis at work is very stark.
Embodied precarity carries other spatial-temporal vulnerabilities. Erin’s symptoms mean she cannot attend work regularly and consistently: On a really bad day, I struggle walking because it’s gone into my spine, the endometriosis. So it’s affected all my nervous system and particularly my left side, so I’ve a bit of a limp and I get a lot of pain [. . .] So when I’m really struggling, just getting into work would be nearly impossible sometimes.
Similarly, Poppy’s unpredictable symptoms profoundly influence the insecurities she feels across time and space: I want to come across as professional and reliable, and you feel like it makes you look unreliable, even though it’s not your fault. It still is something you can’t control. So especially with the travel, there would be times where I’d be kind of walking across an airport with my team thinking, ‘am I going to [faint] now?’. Like, really. So, yeah, it definitely affected how I felt I was viewed. And, you know, it’s quite embarrassing as well to wake up on the floor and have people standing over you [. . .] And it’s just so sudden. You think, ‘Ah, I’m ok, I’ve got this’. And no, you haven’t at all, so . . .
The combination of anticipating symptoms that present without warning with particular aspects of a job, such as travel, which rely on uncertainty and unfamiliarity makes work very taxing. Poppy’s embodied precarity is experienced through a sense of losing control over her body, which has a profound effect on her self-confidence and self-esteem, as she contemplates apprehensively when and how her endometriosis symptoms might appear. Poppy’s fears have material consequences, disrupting both her work and worker identity and exacerbating the discursive representation of women as leaky, unpredictable, and unreliable. For example, she explains how her confidence was impacted to the point that she “canceled travel plans and really missed out” on career experiences and progression. As such, the anticipation that often accompanies embodied precarity can impact not only performance and participation but also work opportunities.
Temporal disabling
A related theme in the data was how participants’ endo time was positioned as problematic within organizational life. Precarity therefore permeated their lived experience in its disabling, disadvantaging and stigmatizing effects. Iris explains: I didn’t have my period in control at that point [. . .] I’d come on during my commute [. . .] When I got to work [. . .] I turned my computer on and I ran to the toilet to go and sort myself out [. . . W]hen I came back, my manager was stood at my desk with his arms crossed, looking really annoyed at me [. . . In] front of everybody, he shouted [. . .], ‘What gives you the right to not be at your desk ready to work at the start of your shift when everyone else is here?’ [. . .] I didn’t know how to tell him that I’d had to go and change my knickers because I’d bled through [. . .] I didn’t have time to ask him before [. . .] I remember my eyes welling up [. . .] I found that a reoccurring theme throughout every job [. . .] people think that you want special treatment or that you’re getting allowances when they don’t realize that you’re actually in pain or you’re bleeding and it’s not fun. I’m not sat in the toilet having a good time. I’m trying to clean myself up. And it was just so horrific [. . .] everyone was looking at me. And ever since then, I just get so paranoid about going to the toilet. And being questioned for it, basically.
Iris’s non-normative temporality is marked by the intersection of multiple sources of discrimination and hostility. Her manager’s response is a blatant expression of gendered and ableist microaggressions, berating her for not abiding by normative temporality for a scant few minutes and demeaning her work identity. Likewise, the shaming Iris endures, alongside menstrual stigma and representations of the ideal worker body, is portrayed in her fear about speaking up. The entrenched norms that give rise to such hostile workplace events have long term effects in the (re)creation of exclusionary environments. Iris’s precarity is increased, notably in her fear of using the bathroom, a resource needed by some social groups more than others, because she has experienced a humiliating restriction on its use. In fact, she is given only “seven minutes a day to go to the toilet” despite her organization’s awareness of her endometriosis. This is a discriminatory attack on Iris’s sex that limits her ability to respond to cyclical menstrual needs, such as visiting the bathroom to change menstrual products. It is also a discriminatory attack on her long-term condition that may require people to manage symptoms of irregular and heavy bleeding, changing of menstrual/incontinence products even more frequently, or the increased urge to empty one’s bladder or bowels when endometriosis penetrates these organs. Indeed, one of Iris’s diary entries recounts how, during an occupational health assessment, the doctor informed her that her manager had asked: ‘when will [Iris’s] condition resolve?’ and the doctor asked me if the company I work for were aware that endometriosis is not curable. It was very difficult to see that even after explaining countless times and practically begging for support, I’m still seen by management as exaggerating it. I’m not sure at this stage if they don’t understand or just do not care, I think it may be a combination of the two.
The workplace further precarizes these participants’ embodiment around presence in and absence from their jobs, as Thea explains: My bosses at the time were like, ‘Well if you can’t do it, then we don’t want you here’. I was like, I can’t give what they need because I felt like there was a barrier, like my pain, I was almost too scared [. . .] they were just like, ‘It’s just like a monthly period’, but it’s more than that. I don’t know how I’m going to be, week in week out [. . .] it’s hard because [. . .] I love teaching kids to swim, but [. . .] I think I became scared of that myself [. . .] And then I knew when I missed work because I was ill, I would then get called in when I was better and I got told off. So, I got too scared to take time off, I was too scared to teach so I just became riddled with anxiety: if I took time off because I was ill, I was going to lose my job.
The responsibility for being able to work normal hours, regularly and consistently, is individualized here, with added pressures to conform coming from able-bodied managers. Thea fears losing her job if she is not able to conform, but, like Iris, fears speaking up to correct the assumptions made about her pain and consequent inability to adhere to rigid workplace requirements. The intersection of androcentric and ableist workplace structures and stigmas about menstruation makes disclosing a widely misunderstood and gendered health condition in the workplace challenging. By disabling individuals working in endo time, the possibility of finding meaning in and leading a fulfilling working life is likewise reduced.
Fears of working in a non-normative temporality also intrude into Anna’s life. She is: Terrified of getting sick, you know, like, sick sick where I’m off for three weeks with the flu or something so that I’ve lost my sick leave [. . .] And, you know, I would use my annual leave. That’s how I did it [. . .] ducking and diving and working [. . .] little systems [. . .] without being fired [. . .] it’s mostly been me having to do it [. . .] there is a lot of lip service paid by management about helping and supporting me: that hasn’t translated terribly well into reality.
Workplace practices and policies based on able-bodiedness create precarious subjectivities by intrinsically linking the identities of those with long-term conditions with feelings of anxiety, insecurity and fragility. Anna self-organizes and works what Seear (2009) calls a third shift. Seear uses this concept to describe how people with endometriosis engage in a combination of self-management, self-care, and patient expertise, given often problematic advice from doctors and unreliable information online, in addition to other paid and unpaid work. Accordingly, Anna goes above and beyond the tasks involved in her paid work and domestic labor to conceal her non-normative embodiment and temporality which, like Thea, put her at risk of losing her job. Her considerable efforts to remain in work include utilizing her annual leave, as common colds and flus can affect her sick leave score. This indicates how management practices that ignore her condition can permeate other aspects of life such as holidays and relaxation time.
Sometimes the fluctuating but unavoidable demands of endometriosis in the context of ableist work norms mean participants have to take sick leave. Endo time then incorporates sick time, required to manage symptoms of a flare up or recover from periods of illness. Sick time is cripped for people with long-term conditions, who require a greater number of absences from work in comparison to able-bodied individuals. Normative constructions of sick time assume someone gets sick, takes time out to recover, rests and returns to work when well. However, as Isabel explains, it can be problematic living up to such a threshold: I’d come back from holiday and just felt really, really ill. I had my period and then [. . .] had a really bad bout of endometriosis but didn’t know what that was [pre-diagnosis . . .] I was just so ill for two or three weeks where I was so weak, and I couldn’t do anything [. . .] I was just in a real state [. . .]. [A]fter that [. . .], once every month I was having to have a day or two off work. So, my sick record was pretty terrible [. . .] because I just couldn’t work [. . .] And basically my boss - what they tried to do was say without a diagnosis, they tried to say that I was disabled and [. . .] put me on part-time.
Regularly irregular patterns of illness and absences reveal the tension inherent in the neoliberal organization of labor grounded on ableist assumptions that individuals are usually healthy and able to be fully productive and, on the rare occasion when this is not the case, sick leave enables them to recover completely and return to work. Isabel’s absences transgress these normative expectations, especially when she takes sickness absence following her annual leave. Her capacity to deliver consistently and regularly as a fully productive neoliberal worker-citizen does not meet the norm of the ideal worker (Acker, 1990). Her boss responds by pushing her into another identity category and trying to limit her contractual work arrangements. This is not only a form of temporal punishment but also discrimination based on a protected characteristic (disability), which may infringe the UK Equality Act. Such temporal standards set a precedent for which bodies can and cannot work regularly and consistently within organizations, and therefore which bodies are and are not welcome at work. Bodies that fluctuate with illness are not as valuable to capitalism where worth is earned through uninterrupted productivity and efficiency (Fazeli, 2016). Bodies orientated under endo time are therefore made yet more precarious: they are disabled by rigid designs of the working week and non-inclusive organizational practices and policies.
Waiting and weighted time
Sick time can be even more complicated for individuals living without a diagnosis. The marginalized experience in the workplace is a mirror of often prolonged and arduous encounters with the medical establishment. Diagnosis can come as a relief, though. Jasmine felt “saved” by her evidence of endometriosis. It orientated her in time in a certain way: it was “like receiving a badge to give to people. It’s like the visible plaster cast on your leg.” However, this medical recognition of a regular condition only confirms the irregularity of her body: I’m a bit scared because I’m like, ‘would I be able to follow the rhythm to’, you know, being creative is not an issue, but ‘can I be structured enough? Can I be productive enough? To make a living on it, of it, and be regular?’. That’s the really scary part for me. I start to believe in it a bit more, but that’s the scary part. If something happens and I’m stuck in bed for a month, I’m like, ‘I’m losing everything again’.
Jasmine highlights the economic vulnerability and social precarity she experiences in endo time whilst working freelance. Although she is not subject to standard organizational temporal expectations, she holds herself accountable to “capitalism’s temporal bullying” (Fazeli, 2016, np), unsure whether she can meet the “structured. . . productive. . . and. . . regular” reward. There is a price for the disruptions of her illness, making her fear “losing everything again.” This marks the liminal space of endo time, at once reinforcing expectations of the ideal worker, whilst one is compelled to attend to the demands of the body. However, another tension exists within endo time as bodies with the condition are not “disabled” by their environment consistently or regularly as, for example, a wheelchair user may be. Instead, symptoms fluctuate across minutes, hours, days, or months in accordance with flare ups and unaccommodating social and physical structures. As we suggested in “Precarity, embodiment and crip time” above Rice et al. (2023: 1726) point out that workplace policies for disabled people concentrate “mainly on accommodating stable, enduring disabilities, while provisions for illnesses generally assume that they are time-limited and non-recurring.” Neither of these applies to endometriosis.
In response to such unrecognized and highly variable embodied precarity, many participants devised individual life rhythms around flexible pacing strategies. Megan, for example, recounts “taking breaks every hour or so” because of the challenges of “working long spells” with endometriosis symptoms that suddenly flare up. Pacing is a “self-management strategy for activity, and against the worsening of symptoms that too much activity brings” under endo time (Harris, 2022: np). Prevailing societal beliefs establish that, if pacing is done well, if you manage yourself well, you can cure yourself (Lowenstein, 2021). This emphasis on a cure, or always moving toward a cure, is what Kafer (2013: 2) defines as curative time. She suggests that “Within this frame [. . .], the only appropriate disabled mind/body is one cured or moving toward cure.” However, when there is no cure, the chronic is ignored. It doesn’t have a place in or through endo time. Such moral pressures to pace, and subsequently cure, oneself place the burden of illness/disability solely on the individual to make all of the moves in the glorification of individualized responsibility (Shildrick, 2009). This further marks the body and one’s position within society as precarious. The regular irregularity of endometriosis is therefore present throughout working life alongside social, political, and economic vulnerability, a culture of disbelief, and experiences of non-citizenship.
Gendered prejudice and precarity drive such disbelief but also the aforementioned disinterest in women’s testimonies of endometriosis pain. When moving to the UK, as suggested earlier, Jasmine had: to start all over again, to be with doctors who ask you terrible questions like ‘are you sure the pain is internal? Maybe it’s because of something else’. So, I was back [to] square one. And I stopped. And started again. And stopped. And started again [. . .] to have ridiculous questions, to have ridiculous tests. Even though I came with proof that I had been diagnosed already.
Despite having diagnostic evidence from her country of origin, Jasmine must re-prove her symptoms to receive UK medical treatment. The medical and social journey she experienced in endo time doubles up on the precarity of her body. It represents a series of paradoxes layered on top of each other. An additional layer of oppression is present because Jasmine is a migrant woman of dual heritage. Waiting time for validation carries weighted time for different social groups, where some voices are less credible than others (Rosen, 2021: 1). UK doctors question Jasmine’s testimony, discrediting her symptoms as “something else,” which likely has its roots in the endometriosis-specific racial bias of the medical establishment. Studies have found black women’s symptoms are not taken seriously (Hoffman et al., 2016) and that they are even less likely to be diagnosed with the condition than white women (Bougie et al., 2019). Certain social groups are therefore orientated differently under endo time as a result of being made even more precarious than others through waiting (and waiting again) weighted time. This is further complicated by racialized disparities in medication, as Jasmine explains. She has had significant problems with blood pressure and potassium levels, which meant she has visited Accident and Emergency several times because the medications prescribed for her endometriosis are “not the right answer for black people.” As Jasmine says, this is “because of the way we did the research and stuff like that. It wasn’t part of the problem to fix any black person here in Europe.” She adds: “probably my body is not answering properly because of my origin.”
Limited research into how genetic differences interact with medicines causes Jasmine to experience negative side-effects, increasing her embodied precarity. This is a significant problem in the medical world at large, but also within endometriosis care specifically because it is a condition traditionally believed to be a white woman’s disease. This myth upholds the racialized assumption that the condition is rare in black women who remain underrepresented in (already scarce) endometriosis research. Bougie et al. (2019) also emphasize that black women may present with different symptoms of endometriosis and require different treatments. A vicious cycle exists for women of color who may experience longer diagnosis times, which systematically exclude them from participating in future endometriosis research. The precarizing of bodies of color with endometriosis is therefore increased, as they simultaneously confront symptoms, gender, pain, and racial oppression (Hossain, 2022) as well as the unwanted side-effects from generic medication tested on white bodies. An awareness of the intersections between gender and race in relation to endometriosis and work means we can identify overlapping and interdependent systems of discrimination and disadvantage for women of color working with the condition. This has consequences for disclosing and accessing support in the workplace, perpetuating inequality and oppression.
The intersections between gender, race, ethnicity, disability, and embodied precarity orientate bodies in specific ways at work. Alisha explains that: my [South African] upbringing was ‘Carry on regardless. Don’t let anybody know that you’re suffering because it makes you look weak’. And being an ethnic minority, if you look weak, it’s not a good sign because it makes you look like you’re not capable of doing your job. And that’s the message I kept getting from my first manager, ‘Well, if you can’t do your job, I can’t do anything about it. You need to think of another job.’ That’s the sort of tone that was used against me [. . .] It’s unfortunate that when you come from an ethnic minority background, you have to do the extra mile. You have to prove yourself a lot more. It’s the way it works. It’s the way the world works. It’s not acceptable by all means. We all do the same thing in that hospital. But when you come from my background, it’s [. . .] entrenched that you’re not good enough because of your colour.
Alisha’s symptoms are difficult to accommodate against the temporal demands of working in a hospital. Her experience of endo time casts her outside of shared time with colleagues, but this is intensified by her racial identity. In order to conceal her Otherness, she must “do the extra mile” and “carry on regardless.” Minority social groups have different expectations placed upon their time in an additional form of “temporal bullying” (Fazeli, 2016). Such expectations often exceed those of normative temporalities in economic regimes of inequality, exclusion, and exploitation (Acker, 2006). As such, Alisha feels unable to embody the full precarity of her endometriosis in the workplace because of racial discrimination that already stereotypes ethnic minorities as inferior and lazy. Such cultural messaging is only confirmed by her manager.
By applying this intersectional lens to the embodied precarity of endo time, we can better identify the oppression resulting from the intersection of gender, race, ethnicity, and disability. In doing so, we can “counter the centrality of relatively privileged white bodies in disability discourse” (Shildrick, 2019: 598) and locate specific inequalities within neoliberal precarization which extends to greater and greater reaches of the population as a result of biopolitical governance through insecurity (Lorey, in Puar, 2012). Our analysis contributes to knowledge on the intersectionality of precarity by arguing that the challenges for different groups of people experiencing the embodied precarity of long-term conditions, such as endometriosis, can be precarizing in the labor market in different ways.
Trade-offs and time traveling trajectories
To manage the embodied precarity of endometriosis, some of our participants transitioned between full-time employment, part-time work, under/unemployment, and precarious work. Specifically, this section explores participants’ experiences of precarious work through gig-work, self-employment turned side-hustle, and temporary work. Endo time, then, is also time travel between various forms of employment to balance earnings against managing symptoms, and can involve significant trade-offs. For some participants, precarious work filled gaps between employment or became a route to work with greater autonomy. Hani, for example, explains her reasons for becoming a freelancer: I created this lifestyle because the office environment doesn’t really serve me, like the nine to five doesn’t really serve who I am, and it was really hard to manage my endo.
Hani chooses precarious work drawn by the flexibility it offers. She engages in a process of “self-precarization” (Lorey, in Puar, 2012: 164) because the traditional working environment and calendar do not suit her endometriosis. Precarious work might therefore be more appealing to people with endometriosis because of how embodied precarity makes the standard working structure challenging. However, the initial “financial strain” of moving into precarious work made Hani’s “endometriosis worse [. . .] because I was constantly stressing, I couldn’t buy the things I needed to buy [. . .] I was taking certain gigs to get by, which weren’t actually healthy for my endo.” At first, then, she found freelance work just as problematic as a traditional organizational environment, having traded flexibility for the security of a regular wage. This had a detrimental effect on her symptoms and increased her embodied precarity.
Indeed, the supposed benefits offered by precarious work can be a double bind for people with endometriosis given the absence of stable contracts, loss of employment benefits (e.g. sick pay, pension contributions etc.) and the financial impact of having to take time off for flare ups or surgery (often multiple surgeries). The individual may also need to be more available than ever in order not to miss out on opportunities to earn a living. Hani explains there is “nothing really as a support mechanism for freelance,” instead “you just fall through the cracks.” This was especially so for her during COVID-19 where UK freelancers were initially overlooked and offered no financial support. This exacerbation of common gig economy dilemmas really exemplifies Snyder’s (2016) “Faustian bargain” between life and work.
However, Hani says she now “actually prefers [freelancing] because even though I’m not protected I still have control.” She has the freedom to take as many sick days and as much time off as she needs to, without the limits imposed by an employment contract. This allows her to schedule “a month off or two weeks off” if she wishes to, which she identifies as her “recalibration moments.” It was especially important for Hani to take “control” over her working life, because of the uncontrollability of her condition. She did this by taking a “big jump” and an “emotionally calculated decision.” She initially had to accept any project “to get by,” in the hope of reaching a trajectory with greater autonomy, which illustrates our observations about trading off and full availability. Searching for flexibility through precarious work in endo time can therefore be a temporal drag (Freeman, 2010), since Hani initially experienced a downturn in the quality and type of projects she was working on, to be able to move forward toward a more emancipatory route. She was eventually able to “turn it around and [get] bigger gigs and more sustained income” as well as to: curate a schedule that works [for] me [. . .] that included travelling, but also included working with incredible people around the world but was really based on my menstrual cycle and how I felt [and to be] able to flex when I worked from home.
Through finally reaching flexibility on her own terms, Hani’s “endometriosis is a lot better than it was” which illustrates our argument about how rigid working practices can force the need to take sick leave. Hani functions in a deviant “chronopolitics” (Freeman, 2005), with a particular orchestration of time that is unique to her. Engaging in precarious work allows her to reframe her working trajectory around health and flexibility, but at the same time this “choice” was driven by unaccommodating workplace environments. Therefore, without flexible workplace practices, individuals may be driven to find more versatile ways of earning a living such as through precarious work—with all of its challenges.
Many participants highlighted the affordances of other flexible working options for individuals orientated in non-normative ways. They particularly referred to working from home which became the new norm for the majority of non-key workers in the UK during the COVID-19 pandemic, when this research was conducted. This period symbolized the destabilization of normative time—the precarizing of us all. It signified a step away from the “highly meritorious regime of ‘correct time’, a kind of hypernormative time’” that prevents the full inclusion and participation of some disabled people (Loner and Rosenau, 2022, p.45). Rhiannon, for example, expressed her ability to respond to the embodied precarity of endometriosis more “comfortabl[y]” at home because of “less pressure” to “mask symptoms” and “physically present” herself “as feeling fine” even within rigid temporal schedules. Rhiannon’s experience highlights how temporality influences performativity. The performativity of looking and feeling well at work is learned, because it is an expectation imposed by normative ableism (Bend and Priola, 2023). To be recognized as a worker requires complying with certain norms, whilst “non-compliance calls into question the viability of one’s life, the ontological conditions of one’s persistence” (Butler, 2009: iv). Performativity then becomes inextricably linked with precarity, and who is recognized and counts and who is not and does not in the workplace (Priola et al., 2018). Rhiannon’s experience of working at home during COVID-19 reduces the need for a particular kind of performativity, and subsequently makes her endometriosis easier to manage.
Choice aside, combining work in the gig economy with managing endometriosis can be challenging when it also operates on normative time regimens built around the “able body” (Loner and Rosenau, 2022). Sourcing regular work may mean expending energy one can ill afford, for example. Contractual obligations may make it impossible to take the extra time required to manage a flare up, creating delays in delivering projects, or waiting for the effects of medication may hinder the ability to get somewhere on time. The embodied precarity of endometriosis symptoms can therefore create even greater insecurity in precarious work.
Jasmine knows this tension. She stopped creating her textile designs as a freelancer after becoming “overwhelmed” by the competing demands of a business that was not “working super well” and her “health [which] wasn’t that good again.” She relied on under-employment at a supermarket in order to “have the right balance” to create again, another trade-off. With limited governmental financial support for precarious workers, however, Jasmine still fears of “los[ing] my business just because I’m not well”: let’s say you have a really good year, and then you can put like, you know, you can contribute and have like [money] put on the side. That’s great. And then some things happen and you have six months really bad. If you’re on your own, you’re going to just completely eat all your years of good stuff during your six bad months, and you go back to zero. And I mean, emotionally, hello, that’s so terrible.
Here Jasmine highlights the insecurity of building up a financial safety net whilst working independently with the embodied precarity of endometriosis. What she amasses in terms of financial savings, contributions to society and the development of her creations is diminished during periods of bad symptoms. This situation displaces and disorientates Jasmine in time. Her body and space are out of alignment. There is no financial cushion to prevent her from falling back to “zero.” In a time when the state would be expected to “take charge,” Jasmine’s partner carries the supportive role and financial responsibility, which changes the dynamics within their relationship, as Jasmine explains: I can’t do that any more because it’s hurting the other side of life to be dependent [. . .] it wasn’t a boyfriend and a girlfriend. It was a nurse and a patient. And it was a bank and a creditor [. . .] the tension about my health is always there.
In this way the relationship between the embodied precarity of endometriosis and precarious work can represent a type of “strange room,” where there is uncertainty about which way to turn, because someone doesn’t know which way they are facing (Ahmed, 2006: 7). Precarious work can therefore complicate the promise of futurity—of building enough resources, equal relationships and certainty around one’s future life - for precarious bodies, increasing instability, and insecurity.
Anna also feels insecurity around the embodied precarity of her health which is intensified by her temporary post in a museum. Her employers “rolled [my position] over and [. . .] over and then they stopped it so that they weren’t obliged to offer me a permanent job and then they started it again.” This precarity made her fear taking “a formal physical health problem to HR [in case] they won’t renew my contract.” She withholds information about her condition at work to stand a chance at securing her future. Anna is searching for stability to manage her endometriosis symptoms but is temporally at the mercy of her employers until her contract becomes permanent. She works through pain and annual leave waiting for the promise of permanence, but in a system of “flexploitation” coupled with an unrecognized health condition, her organization continues to extend her insecurity with the resulting detriment to her health. Here we can vividly see the demerits of “flexible” work that is entirely driven by the employer’s needs. Our concept of endo time, therefore, illuminates the requirement for supportive organizational interventions for people whose embodiment orientates them in non-normative ways to enable them to contribute to the labor market without exacerbating their health conditions.
Discussion and conclusion
This paper contributes the concept of endo time to crip theory by highlighting how the embodied precarity of endometriosis generates considerable challenges for cis women working with the condition. Endo time not only genders crip time but also encompasses the challenges caused by highly variable symptoms. In addition, it extends knowledge of the impact of embodied precarity in relation to long-term considerations for women’s identities within and outside of work, including extended diagnostic delays. Further, it demonstrates how this affects self-esteem, self-confidence and a sense of full citizenship and futurity. Endo time also recognizes that gendered conditions are especially badly misunderstood, even amongst health professionals. Diagram 1 brings together these strands of endo time to illustrate how intersectionality and organizational reactions to endometriosis transpire, in a process of precarization.
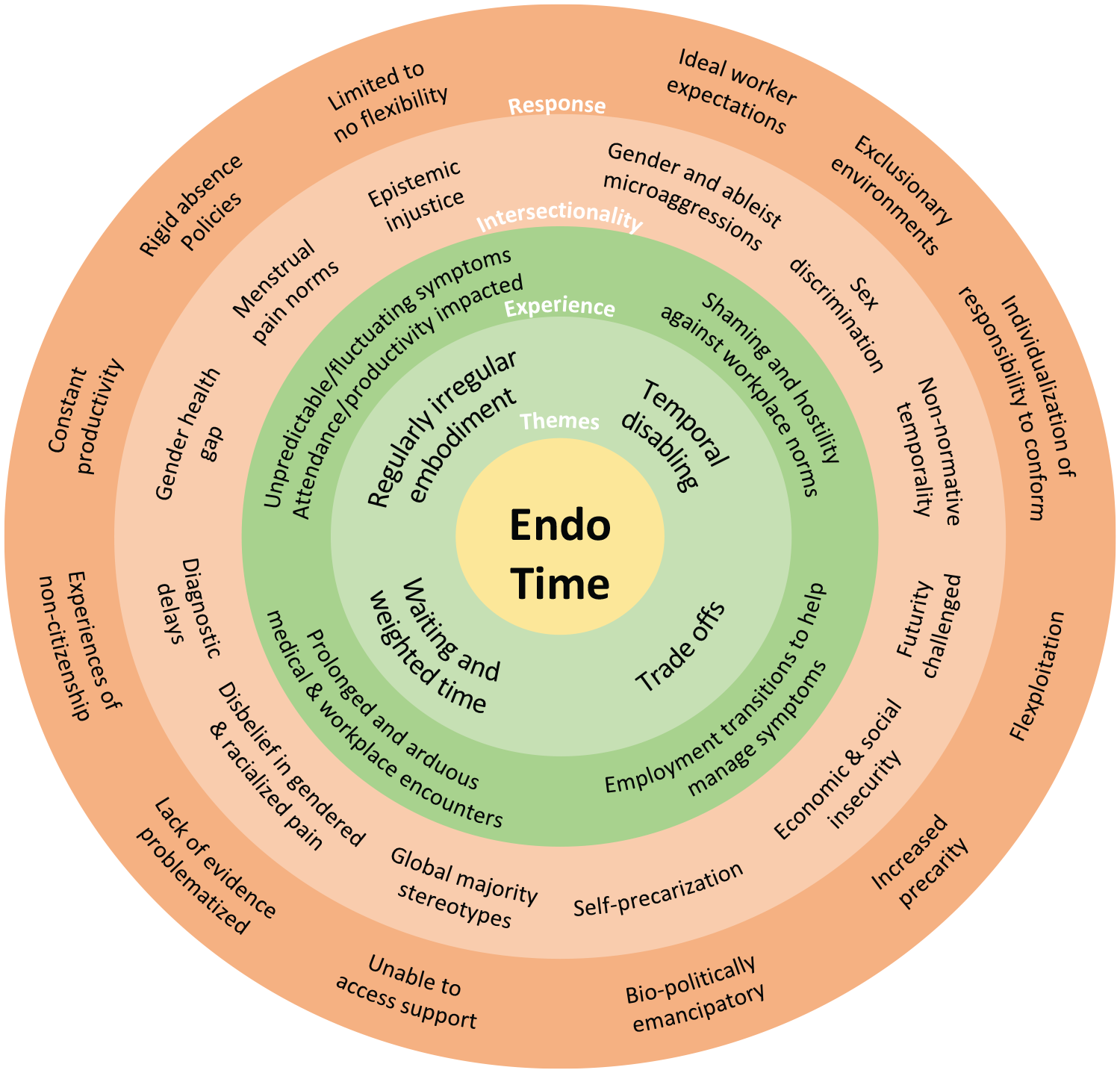
Endo time: theoretical interconnections between themes, experiences, intersectionality and organizational responses.
As the diagram suggests, we connect the four themes of endo time with: participant experiences of non-normative temporalities; the intersectional dynamics of gender, disability, race and ethnicity; and organizational responses to embodied precarity, in order to highlight the intersectional layers of gender inequality at work for individuals working with a condition like endometriosis. In doing so, we unravel and connect the significant challenges of:
(a) Regular irregular embodiment - these shifting temporalities are problematized by organizational responses based on androcentric and ableist narratives of constant productivity, rigid absence policies and limited to no flexibility. As such, experiences of endo time are particularly and increasingly precarized by the intersectional layers of epistemic injustice surrounding gendered and unpredictable long-term health conditions.
(b) Waiting and weighted time, characterized by prolonged and arduous encounters both with the medical establishment and within work environments, can mutually reproduce processes of precarization. Diagnostic delays impact the evidence so often required to prove one’s suffering and seek support at work. This disbelief in gendered and racialized pain intensifies precarization by increasing the burden experienced in everyday living and working and by distinguishing which bodies can and cannot be accommodated at work.
(c) Temporal disabling = the experiences of shaming and hostility driven by workplace norms and the myth of the ideal worker are infused with intersectional dynamics of gender and ableist microaggressions. The consequent discrimination is embedded in discursive representation of women’s bodies as leaky, unpredictable and fragile and upholds temporal narratives that foster exclusionary workplace environments.
(d) Trade-offs may make self-precarization as an ever-more attractive prospect as it offers freedom and flexibility when managing an unpredictable long-term condition. Whilst this trade-off can be biopolitically emancipatory in some instances, the requirement for freedom and flexibility can be exploited for certain social groups, thereby intensifying processes of precarization and challenging an individual’s sense of futurity.
Endo time highlights the significant temporal challenges of finding options that protect individuals from going “back to zero.” Individuals with fluctuating and gendered long-term conditions within precarious labor contexts, we suggest, risk going “back to zero” in configurations of socioeconomic exploitation, losing everything in terms of financial resources and labor market participation, progression and performance. This is against a background of increasingly poor welfare provision and exclusionary workplace practices and policies. Still, some people “choose” precarity, risking going “back to zero” to create a new flexible economic lifeline that permits them to better respond to their non-normative embodiment and temporality. Going back to zero and labor precarity in this sense may be biopolitically emancipatory from the rigid temporal neoliberal working constraints for individuals with fluctuating long-term conditions—but equally it may not, as our data also suggest.
We relate these findings to broader discussions regarding the complexity of labor precarity and processes of precarization. Particular precarities can be welcomed in order to have control and the freedom to choose a rhythm of living and working (Lacerda, 2024), whilst at the same time such choices are entangled in systems of exploitation and oppression hidden behind these constructions of freedom (Peticca-Harris et al., 2020). As such, although some participants described their feelings of liberation whilst engaging in processes of self-precarization, the ability to remove oneself fully from the temporal trappings of capitalism intensified by the dismissal of irregular, gendered symptoms remains highly nuanced.
The disruption of the COVID-19 pandemic is likewise notable in relation to experiences of embodied precarity. Those already in precarious labor contexts experienced increased precarity, whereas in a more standard employment context it helped to destabilize the rigid temporal structures of work allowing some individuals to thrive through greater flexibility to respond to their symptoms while working remotely. Precarity and processes of precarization therefore are not only complex, but context- and temporally dependent.
Endo time, as a subset of crip time that focuses on the gendered experience of fluctuating long-term health conditions like endometriosis, helps us to theorize more adequately about this experience. As an activity, a verb, endo time also extends Seear’s (2009) work on the third shift done to mask symptoms and learn to manage endometriosis in, around or for employment specifically. Indeed, the precarious subjectivities of people operating in endo time are exacerbated by the epistemic injustice surrounding menstrual health and menstrual conditions in society. This form of injustice is identified by Fricker (2007) as having two key facets: testimonial injustice, where what someone says is routinely disbelieved because they are seen to have a “credibility deficit”; and hermeneutic injustice, where there is a lack of discursive resources to make sense of some social groups’ experiences. Here we extend the work of Remnant et al. (2021) on disabled academics including gynecological conditions and Reid (2020) on the healthcare experiences of women with endometriosis. Endo time thus advances feminist theorizing of precarity by shedding light on how lived experiences of endometriosis have been excluded and denied epistemic authority at work and elsewhere, and accordingly how external and embodied precarity is shaped and intensified for those living with the condition through the organization of work.
Implications for organizations and suggestions for further research
The study offers important implications for organizations to support the work and careers of people with fluctuating long-term health conditions, particularly where these are gendered. For example, given the long-time frame for diagnosis, employers can (and should) put in place accommodations for those experiencing problematic periods without requiring a medical diagnosis. Accommodations such as flexible working can support people with endometriosis to respond to the multifaceted demands of health, work and life. Similarly, workplace cultures that foster an open dialog about gendered long-term health conditions create an environment where individuals feel safe to discuss their condition and how it affects them at work. This stimulates conversations of appropriate adjustments that are unique to each person experiencing symptoms as opposed to blanket offerings.
Likewise, training and education for line managers especially may help to reduce the epistemic injustice of people experiencing gendered long-term health conditions at work by replacing the individualized burden of the condition and responsibility to conform to cultural norms with greater understanding and supportive workplace arrangements. For example, we found rigid workplace practices and policies to be a major source of gender inequality, disability and discrimination for people working with endometriosis. Furthermore, employers with the facilities to do so may wish to include women’s health conditions in their occupational health provision. Trade unions are increasingly adopting proactive approaches to women’s health at work (see e.g. the Trade Unions Congress, 2023). Our research offers the opportunity for employers and trade unions to work collaboratively to help overcome the challenges faced by those managing endometriosis in workplaces designed around a cis male able-bodied norm.
Our research has also suggested some intriguing possibilities for future research in the area. For example, whilst the process of securing ethical approval for the study necessitated exclusion of anyone who did not have a formal medical diagnosis of endometriosis, the extended delays in securing such a diagnosis mean that, as we argued earlier, considerable numbers of women are in the weighted waiting time of seeking this confirmation. We might have also systematically excluded individuals from minority groups who experience longer diagnostic waiting times (Bougie et al., 2019). The experiences of employment of those who do not have a formal diagnosis deserve proper consideration, especially given the standard (albeit very problematic) expectation that any accommodations for health conditions in organizations be supported by a formal diagnosis. Future research should also ensure a wider representation of people of color to further explore the intersections of race, ethnicity, gender, and disability. It should, further, explore the experiences of those who become unemployed because of their condition who were excluded for methodological reasons. Further, all our respondents were cis women. Future research should aim to understand the working experiences of transgender, intersex, and gender nonconforming people with endometriosis whose stories are wholly missing from the literature.
Moreover, whilst there are marked similarities between endometriosis and other gynecological conditions like adenomyosis, dysmenorrhea and menorrhagia, there are also differences. We would therefore strongly recommend not only more research into how people with endometriosis navigate work but also scholarship which explores the experiences of combining employment with these other common gendered health conditions. Equally, we were struck by Rice et al.’s (2023) analysis of episodic disabilities [sic], a concept which is likewise under-traveled in organization studies to date, but arguably paves the way for more intersectional work focusing on individuals with gendered episodic disabilities like endometriosis but also those which disproportionately affect people from certain heritages, like sickle cell anemia. We wonder if experiences of crip time at work vary amongst these groups of people, connecting back to our central concept of endo time. This would allow for an examination of how gender and racial pain gaps, epistemic injustice, embodied precarity, “choice” of employment, and futurity play out in these instances.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.