
Abstract
Traditional understandings of care-giving assume care practices are clear to others and unambiguously altruistic, reflective of the selfless and humane bearing of care professionals. However, a range of organisational research has noted the complex and often contradictory ways in which enactments of care are interwoven into organisational relations of power and control. Through a narrative analysis of interview data, our paper focuses upon practices of inaction and concealment as ‘veiled’ care set within the power-laden complexities and contested meaning-making of organisational life. Our notion of veiled care extends debates about care as a social practice in everyday work relations in two ways. Firstly, it provides a greater focus on the less discernible aspects of care-giving which are significant but possibly overlooked in shaping subjectivities and meanings of care in work relations. Secondly, it develops the discussion of the situated ambiguities and tensions in enacting care that involves overcoming care-recipient resistance and an arguably less heroic but nonetheless important objective of non-maleficence, to avoid, minimise or repair damage.
Introduction
Care for clients, customers and employees is becoming an increasingly important concept in organisational and management research (Fotaki et al., 2019; Rynes et al., 2012), with research into sites of professional care-giving (e.g. Molterer et al., 2019) as well as scholarship on caring leadership (Tomkins and Simpson, 2015), managerial care (Kroth and Keeler, 2009) and compassion (e.g. Dutton et al., 2014; Kanov et al., 2017). Interpersonal care-giving is acknowledged as relationally complex, involving different practices and different goals, for instance to provide direct assistance but also to nurture autonomy and independence (Kroth and Keeler, 2009; Mumford et al., 2019). Yet the literature on care in the workplace has so far tended to emphasise particular performative qualities of ‘doing’ (Gherardi and Rodeschini, 2016) care, highlighting the intervention of care-givers and the co-construction with care-recipients of outcomes based on shared, ‘certain’ (Kanov et al., 2017) understandings of the personal needs, goals and interests in play. The problem with this emphasis is two-fold. Firstly, it has not yet fully taken into account the empirical difficulties of negotiating meanings and interests within the messier, power-laden situated social terrain in which care is enacted (Simpson et al., 2013). Therefore, secondly, it has not yet fully appreciated the less discernible practices (e.g. Frost, 2003, 2004; Kahn, 2001) that are involved. In summary, there is more to care-giving than meets the eye.
In this paper, we stake out a perspective on care practices at work that weaves in a discussion of power relations, complexity and ambiguity and that shows some of the hidden work of enacting care. Our argument emerges from a narrative analysis of interview texts about being gentle at work. On the face of it gentleness is a positive quality of social relations. Yet the analysis raised questions about ambiguous and instrumental undertones in the narratives as interviewees construct practices, goals and meanings that remain veiled, or hidden, from the other characters within the narratives, although still beneficial to them. The research question posed in this paper therefore is: how might we theorise the care effects that emerge not from clear interventions of support and solidarity but from care-giver inaction and concealment? The answer we offer is through the concept of ‘veiled care’. We define veiled care as self-reflexive practices that hold back from action and that obscure or create ambiguity in social meaning in order to avoid, repair or minimise damage to others. Our use of the metaphor of the veil calls attention to ‘muffled’ (Mazzei, 2003) subtexts that pass unnoticed or that create other ways of reading meaning into comments and actions. It points to what is not shared explicitly or openly between care-giver and care-recipient, as workers navigate local power relations to support care-recipient autonomy but also to overcome their resistance.
Our approach is informed firstly by scholars who promote care as an important phenomenon in work relations (e.g. Frost, 2011; Rynes et al., 2012), particularly from the perspective of Positive Organisational Scholarship (see Cameron et al., 2003), and secondly by scholars who argue from a critical perspective that relational power dynamics need to be noticed in organisational life (Clegg, 1989; Clegg et al., 2006; Fineman, 2006; Simpson et al., 2013, 2014a). We make two theoretical contributions to the literature on care as social practice in everyday work relations. The first contribution is to extend the literature by advancing an understanding and appreciation of care-giving which includes practices that are not openly shared between care-giver and care-recipient. Self-reflexive practices of inaction and concealment contribute to shaping emergent subjectivities and meanings of care as social relations unfold. The second contribution extends the literature by reinforcing how a theory of care in work relations involves conflict, ambiguities and tensions and an arguably less heroic goal of non-maleficence, to avoid, repair or minimise damage to others, amid the compromised and complex arena of organisational life. Our analysis highlights less straightforward understandings of care that address the situated ‘struggle for meaning’ (Simpson et al., 2013: 387) and a broader landscape of multiple and potentially competing interests, focusing on strategy rather than altruism.
In this paper, we use the terminology of ‘care-giver’ and ‘care-recipient’ to describe the different subject positions in care relations. However, this is for clarity in writing, since we do not assume that these positions are fixed. Indeed, the argument that veiled care may be especially important in downplaying static subject positions and contributing to a dynamic fluidity in care relations (see Tomkins and Simpson, 2015) is one that we return to later in the paper.
We set out the paper as follows. The next section summarises the organisation and management literature on interpersonal care relations, the debates about care and power, and how the complexities of care-giving, care practices, and practices of inaction and concealment have been depicted. We then outline our research design and methodology. In the subsequent section, we use extracts from our empirical data to illustrate how interviewees talked about practices of inaction and concealment as veiled care within narratives of being gentle at work. In the discussion, we elaborate how inaction and concealment can be appreciated as veiled practices of care, and the implications of this for our understanding of care in everyday work relations. Concluding comments point to the importance of recognising the concept of veiled care in developing more complex and indeterminate accounts of enacting care in organisational life.
Depictions of care practices and care relations at work
In the following discussion we draw on writings on compassion (Dutton et al., 2014; Frost et al., 2006; Kanov et al., 2017; Lilius et al., 2008; Simpson et al., 2013, 2014a, 2014b, 2014c; Way and Tracy, 2012), particularly on compassion as interpersonal work (Frost et al., 2006), as well as managerial care (Kroth and Keeler, 2009), caring leaders (Gabriel, 2015) and caring leadership (Ciulla, 2009; Tomkins and Simpson, 2015), ethics of care (Gilligan, 1982; Lawrence and Maitlis, 2012), holding environments (Kahn, 2001) and emotional toxicity (Frost, 2003, 2004). We characterise the social relations in these literatures overall as relations of care due to their other-oriented concern, paying attention to and addressing the specific interests or needs of others (Fotaki et al., 2019; Tronto, 1993, 2010) albeit in different ways and with different focus. For instance, compassion aims to alleviate others’ pain and suffering (Dutton et al., 2014; Frost et al., 2006; Kahn, 2001; Kanov et al., 2004), managerial care prioritises attending to the unique and changing personal needs, development and growth of employees (Kroth and Keeler, 2009), and caring leadership pays self-reflexive attention to the embodied effects of one’s action upon others (Tomkins and Simpson, 2015). It is worth noting that the organisational and management literature on care relations draws significantly on studies of work in professional care settings, such as hospices (Way and Tracy, 2012), care homes (Gherardi and Rodeschini, 2016; Molterer et al., 2019) and social services (Kahn, 1993), on theory derived from ‘caring’ professions such as nursing and education (Kroth and Keeler, 2009), as well as on philosophical and religious writings on ethics and morality (Rynes et al., 2012). In these contexts altruistic motivations and dispositions towards others are emphasised.
A significant and important push around workplace relations of care has emerged from Positive Organisational Scholarship (POS). POS ‘seeks to understand what represents the best of the human condition’ (Cameron and Spreitzer, 2012: 1) and contrasts to scientific Taylorist prioritisations of economics rather than humanity in the workplace (Frost et al., 2006). As part of the POS agenda, care and compassion have been promoted overwhelmingly as positive concepts (e.g. Frost, 2011; Rynes et al., 2012) with organisational benefits (Dutton et al., 2002) that are worth fostering and understanding in different contexts (e.g. Dutton et al, 2006; Lilius et al., 2008).
In the last few years, a set of papers by Simpson, Clegg and colleagues have applied a critical lens to POS scholarship and have argued that compassion is a relation of power in which particular ‘subjects and objects’ (Simpson et al., 2014a: 353) are constructed and through which particular interests are supported (Simpson et al., 2013, 2014a, 2014b, 2014c). They suggest that the POS discourse of compassion has been framed and promoted largely from a heroic and altruistic perspective of a powerful compassion-giver, as magnanimous bestower of support to those deemed sufficiently deserving, but that it has not yet adequately addressed the more problematic experience and subjectivity of the compassion-recipient (Simpson et al., 2013, 2014c). Before proceeding further, we outline the relational theory of power that this scholarship draws on and that we use subsequently to develop the concept of veiled care.
Care and power relations
The notion of power as relational highlights the situated, dynamic and contingent aspects of everyday social relations in which meaning, conflict and resistance are negotiated (Clegg, 1989, 1994; Clegg et al., 2006). The notion contrasts with static understandings of power as being somehow held or possessed by particular people, particular job roles or via access to certain resources. Taking certain aspects of social life for granted, non-decision-making (Bachrach and Baratz, 1963) and a lack of resistance are all noted as significant effects of power relations (Foucault, 1977; Lukes, 1974), so that situations of conflict may be seen as atypical settings for power relations rather than the epitome (Clegg, 2009). Drawing on Foucault’s and Machiavelli’s writings (see Cunha et al., 2013), power encompasses both productive and disciplinary aspects (Clegg, 1989, 2009). These aspects are played out, and made manifest, in local events through relations between workers who are positioned within socially structured, multiple, and fragmented ways of acting, thinking and feeling in the form of self-disciplinary (Foucault, 1977) subject positions or subjectivities.
The relational view of power raises issues of agency, resistance, strategy and the struggle for meaning in local contexts (Simpson et al., 2013). Outcomes are indeterminate and contingently accomplished in unfolding social relations. Meaning is unstable and open to contest. Agency is constrained and shaped by others’ response and resistance (Clegg, 1994; Ladkin, 2018; Ladkin and Probert, 2019). Social effects are produced through ‘strategic ambiguity’ and ‘deniability’ (Davenport and Leitch, 2005) and through ‘external subjectivities’ enacted by those who are ‘cynical’ about their work (Fleming and Spicer, 2003) just as much as through attempts to produce clear and shared meaning.
For our purposes, a relational theory of power brings attention to the struggle for meaning in care relations. One person’s subjective intention of care may be misread, responded to and resisted by others applying a different set of ‘rules of the game’ (Clegg, 1989: 209–11). For instance, ‘care’ may be interpreted as ‘control’ (see Sewell and Barker, 2006). Explicit interventions of support may be benevolent but also infantilising and paralysing (Gabriel, 2015); they may evoke feelings of gratitude from the care-recipient, but also feelings such as shame, indebtedness or being patronised (Simpson et al., 2014a). Care-recipient resistance may therefore emerge from the power dynamics of unfolding social relations and the social constitution of particular subjectivities that position them as vulnerable, weak and in need of assistance (Simpson et al., 2013). Care-givers are shown as caught in webs of relational interdependence, needing to work out how to accomplish care effects in the face of competing meanings and possible resistance (Simpson et al., 2013).
In the next section we summarise some of the dilemmas and tensions in care-giving to which a strategic response is required, and how care practices as well as practices of inaction and concealment have been portrayed across a range of literature.
The complexity of situated care-giving and the struggle for meaning
Much has been written about the complexities, tensions and skills required to negotiate the relationship between care-giver and care-recipient (see Gabriel, 2015; Kahn, 1993; Kroth and Keeler, 2009; Tronto, 1993, 2010) so that the latter is ‘appropriately receptive’ to care-giving ‘without running too far away or jumping too close’ (Kahn, 2001: 268). Contrasting goals of interpersonal care have been described, for instance to provide direct support and a sense of connection with others but also to build self-reliance and autonomy (Kahn, 2001; Kroth and Keeler, 2009; Mumford et al., 2019). One of the complexities of care-giving is how to provide support and direction to care-recipients without damaging them by limiting their autonomy and personhood (Simpson and Berti, 2019; Tomkins and Simpson, 2015; Tronto, 1993). Another complexity is that enacting care for one person may impact negatively upon others, including the self and the organisation (Fotaki et al., 2019; Tronto, 1993). As Gabriel (2015: 328) points out, a relational ethic of care is not by itself a sufficient ‘compass’ for caring leadership: if it fosters nepotism and discrimination, it clashes with an ethic of justice (Gilligan, 1982) as a fair treatment of all based on universal standards and rules. Ethical complexity is introduced into considerations of what counts as ‘legitimate’ (Simpson et al., 2014b) care-giving.
While acknowledging this complexity, most descriptions of care practices focus not upon themes of inaction and concealment but upon love, authenticity, visibility, active intervention, clarity, understanding, solidarity and reciprocity between care-giver and care-recipient, where the care-recipient’s needs and interests are central. For example, while emotions can be ambivalent and complex, Gabriel (2015: 321) points out that ‘love is the sine qua non of the caring leader’. Meanwhile, ‘empathy’ is at the heart of compassionate acts (Kanov et al., 2004); and ‘maternal’ feelings that prompt nurturing and personal growth are the exemplar of an ethic of care (Lawrence and Maitlis, 2012). Kroth and Keeler (2009: 521) argue that both care-giver and care-recipient must be ‘active agents’ to build the managerial care process together. In the compassion process, built upon notice-feel-respond stages (e.g. Kanov et al., 2004), it is the clear expression of pain by a sufferer that leads to active intervention in response (see Dutton et al., 2006; Lilius et al., 2008); ‘uncertainty’ (Kanov et al., 2017), about whether someone is suffering and whether assistance is necessary, hinders the process. Moreover, compassionate interventions are described as creating a shared ‘felt connection’ between people, whereby care-recipients ‘feel seen and known’ and ‘less alone’ (Kanov et al., 2004: 809). Similarly, in their discussion of how an ethic of care might be enacted in work teams, Lawrence and Maitlis (2012) outline the role of narrative practices that build team members’ ‘shared realities’ (p. 648) and beliefs about the team and its resilience. In short, in many perspectives on care relations, altruistic concern for the other, active intervention, shared understanding and unambiguous meaning become the basic conditions for care-giving. The care-giver seeks to convey clearly her concern for, and action on behalf of, the care-recipient’s interests; and the care-recipient responds, acknowledges the care-giver and confirms eventually that their needs have been met (Tronto, 1993).
There is some recognition in the literature of the part played by less active, less visible practices in the process of enacting care. For instance, open listening builds empathy and gains information about the care-recipient’s pain before compassionate alleviating action is taken (Frost et al., 2006; Way and Tracy, 2012). Way and Tracy (2012) also discuss ‘strategic inaction’ in their study of hospice work, that gives from hospice staff to patients ‘the gift of quiet, time, and space’ that is ‘subtle’ and ‘[moves] beyond what can be seen by receivers or outsiders’ (Way and Tracy, 2012: 306). Meanwhile, references to ‘compassion work’ and ‘compassion labour’ (Frost et al., 2006) point to some of the hidden effort involved in care relations.
Meanwhile, Tomkins and Simpson’s (2015) paper on caring leadership also advocates for an awareness of the limits to care-giver intervention, a tolerance of ambivalence, and the importance of an ‘organisation of the self’ within an ongoing process of care. They describe two contrasting modes of intervention, ‘leaping-in’ and ‘leaping-ahead’, based on Heidegger’s philosophy of care, that have different impacts upon others. ‘Leaping-in’ provides a direct substitution for the care-recipient when she is struggling, with the care-giver taking over control and directing the solution. ‘Leaping-ahead’ paves the way for the care-recipient to act for herself, through the care-giver facilitating or pointing out possibilities or options for action with which the other can engage in her own way, on her own terms.
Kahn’s (2001) paper on holding environments arguably provides an illustration of ‘leaping-ahead’ and some of the limits to intervention. Kahn describes holding environments, developed from psychoanalytic theory, as temporary safe psychological spaces in which to process anxieties and insecurities that can arise in ‘boundaryless’ organisations. Here it is care-recipients who authorise another person to hold them in temporary shelter so that they can feel ‘safely overwhelmed’ (p. 268) and engage in a process of recovery. During this time, the care-giver pushes away other roles and tasks in order to be available as a resource to the care-recipient, with ‘phones [. . .] not answered; computers [. . .] not glanced at; papers [. . .] not shuffled; other topics [. . .] not randomly introduced’ (2001: 270). Nevertheless, with some ambivalence about the need for holding environments, Kahn (2001: 276) describes them as spaces of ‘collusion’ that enable people to withstand difficult working conditions that might otherwise provoke resistance and change.
In similarly difficult organisational settings, Frost (2003, 2004) describes ‘toxin handling’ (Frost, 2003, 2004) where organisational members disperse emotional toxicity before it can harm others. Frost describes how emotional toxin handlers provide ‘buffering’ (2004: 116) by glossing over and reframing organisational messages in order to deflect or prevent anger, fear, or demoralisation that might arise from the original version of statements. These practices draw on themes of the ‘quiet manager’ (Mintzberg, 1999) who deals in non-disruptive ways with the ‘messy patterns of daily life’ (Mintzberg, 1999: 30).
The kind of quiet, concealing practices highlighted above attend to goals of care-recipient autonomy, self-reliance and the dignity of personhood (Kostera and Pirson, 2017). They enact ‘invisible’ rather than ‘perceived’ support (Zee and Bolger, 2019: 315). However, they raise certain issues. Simpson et al. (2002) point out that ‘negative capability’ – the ability not to do something, to sustain ‘reflective inaction’ – is problematic within dominant discourses based on positive action and performativity. Moreover, as practices of care, they may be deemed too insubstantial, merely applying a bandage to pain and suffering without challenging the organisational roots and causes of it (see Liedtka, 1996).
This raises the question about the purpose of care and its relationship to other goals and other work tasks. The literature on care relations is ambivalent on this point. For instance, care has been proposed as instrumentally useful to organisations, serving to reinforce team resilience for example (Lawrence and Maitlis, 2012) or to avoid burnout (Kahn, 1993), with care as ‘managerial strategy’ (Kroth and Keeler, 2009) for productivity benefits. Alternatively, it has also been proposed as an impediment to organisational performance, posing a challenge to extant power relations and injustices (Liedtka, 1996), requiring care-giver courage to intervene actively and visibly on behalf of, and in solidarity with, the care-recipient, to put their interests first in the face of competing interests and organisational risk (Kanov et al., 2017).
If we step outside of the literature on care relations, the problem with considering inaction and concealment straightforwardly as care is illustrated by referring to scholarship on organisational change as ‘oblique engagement’ (Chia, 2014: 8) or strategy as indirect action (Chia and Holt, 2009). A strategic judgement of timing, tactics and situational contingencies generates a subtle impetus for change that goes virtually unnoticed by others and that hence does not disturb them (Chia, 2014). Oblique engagement may avoid disturbance and anxiety; however, it may also be framed as a Machiavellian, strategic way of achieving primarily organisational ends while outflanking resistance through ignorance (Clegg, 1989). The subjectivities associated with Machiavellian strategy are not usually those of virtuosity and care-giving but rather more questionable and ambivalent ethics (see Cunha et al., 2013).
The literature above highlights the complex range of goals involved in care and some of the difficulties in enacting and defining what counts as legitimate care-giving amid the power-laden complexities of organisational life. While much scholarship tries to solve these difficulties by promoting the unambiguous centrality of care-recipient interests and emphasising the care-giver’s active involvement in the care process, the literature raises the possibility that other self-reflexive, inactive and concealing practices also play a role in care-giving. This has not yet been fully elaborated in the literature on care as social practice.
In the next section we set out our research design, data collection and data analysis methods before turning subsequently to our empirical data.
Research design and methodology
Our interview data were generated as part of an exploratory study of the significance and practice of gentleness in the workplace (see Holman et al., 2017). The exploratory research arose from our sense that gentleness was an important concept to which little attention had been paid in organisation and management studies: the research intention was to investigate whether the terminology and its associated practices inspired new insights into the theme of care in workplace settings. In the research design therefore, we pursued a strategy of theoretical sampling (Glaser and Strauss, 1967) across work contexts in order to contribute to evolving theory (see Creswell, 1998: 56, 118). The contexts included sites where practices of care would be immediately relevant and meaningful to interviewees’ work, such as in health and social care, as well as where they were not directly or obviously connected to it, such as in commercial and industrial settings.
Data collection
Interview methods were used for data collection in order to generate narratives of being gentle that were meaningful to research participants. We conceptualise the interview as an active site (Holstein and Gubrium, 1997) of narrative meaning-making, where interviewees attempt to construct coherent narratives of themselves and their actions and to reconcile conflicts between alternative plots (Czarniawska, 2004: 47–60).
Our sample of 27 interviews was assembled from two different but related sources connected via the second author’s close involvement with both. One set of seven interviews, with people employed specifically in health and social care sectors, was collected as one initial stage of the wider research study into employee gentleness. The interviews were conducted by David Holman, Maurice Nagington and Laurie Dunn. This set of interviews enquired about being gentle with clients and patients. The other set of 20 interviews was generated for a postgraduate research dissertation by a student of David Holman. Her interview transcripts are used in this paper with permission. Interviewees were recruited via the student’s personal contacts across public, private and voluntary sectors, and include people employed in a wide range of sectors. They were interviewed about being gentle with other employees within their organisation. Both sets of interviews were conducted using semi-structured interview schedules that encouraged interviewees to narrate up to two examples of themselves being gentle, generating 50 narratives in total. Interview questions prompted interviewees to provide details about key characteristics of being gentle, the limitations and barriers to being gentle, motives, descriptions of the other person with whom they were interacting, verbal and non-verbal behaviours and emotions. In the interview we did not explicitly connect gentleness to the theme of care, nor suggest that it was either desirable or undesirable at work. Instead we sought to invite the interviewee to direct the narrative as they wished.
The authors who were involved in the interviewing stage of the research met frequently to discuss emergent themes and the ongoing approach to data collection. We continued to conduct interviews until we sensed that no significantly new patterns in the narrative data were being generated and that theoretical saturation had been reached. Interviews were audio-recorded and professionally transcribed.
Data analysis
Our analytic framework draws on narrative theories that alert the analyst to the ways in which research participants socially construct phenomena as appropriate, plausible and acceptable in social context, in narratives that are populated with certain types of characters, relationships, themes and intentional actions that can be accounted for within the plot (Czarniawska, 2004). In the first pass through the data, the first author concentrated on narrative coding (Saldaña, 2009) for the descriptions of being gentle in order to ‘enter into’ the text and produce an internal analysis of it (Silverman, 2006: 166). She coded for the characters in the narrative and the structural relationship between them, the quality of the relationship, the motive driving the plotline, and the interests being pursued (see Table 1).
Summary of narrative coding.
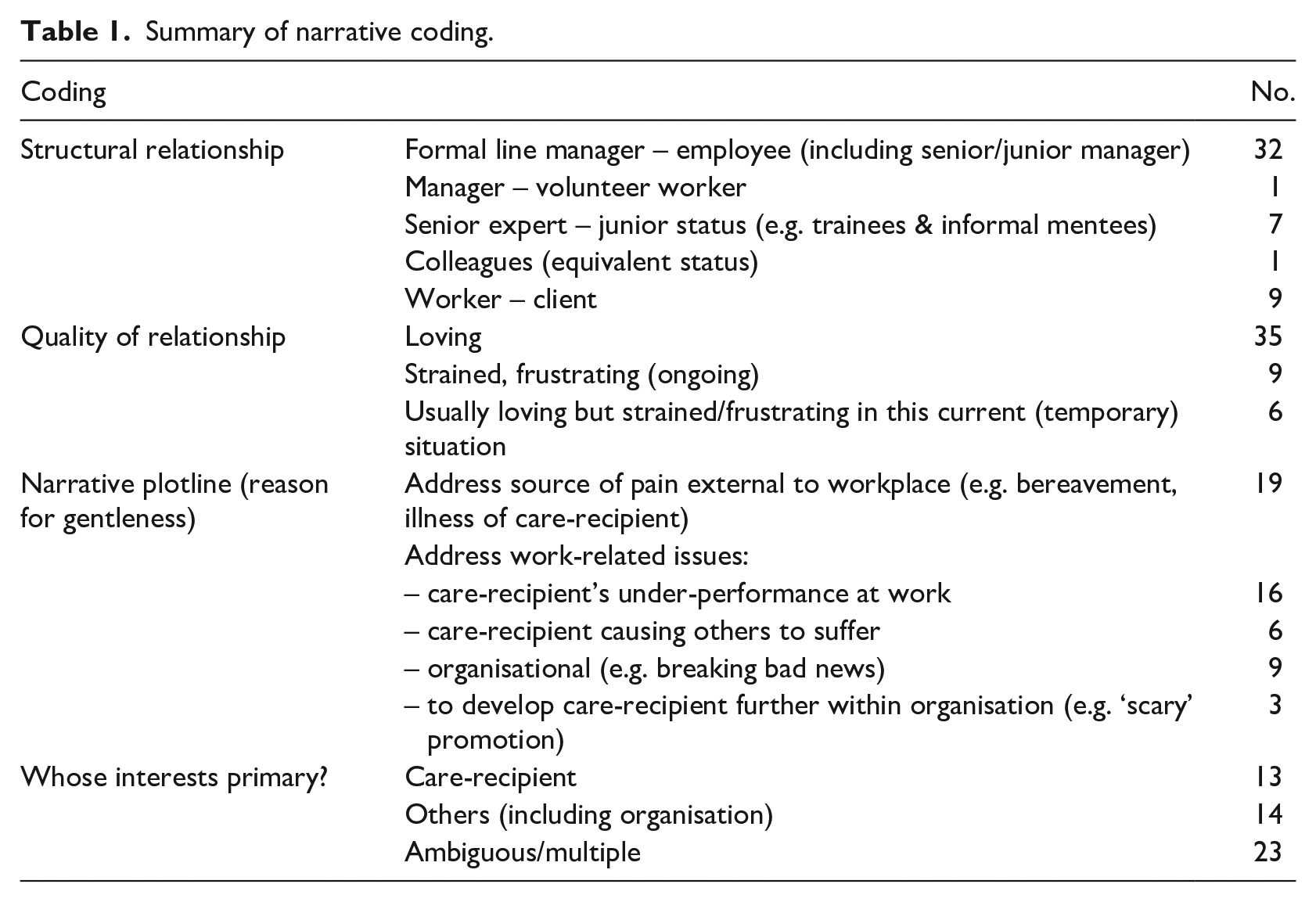
Through iterative readings, interviewees’ narratives were all classified as ‘good stories’ (Squire et al., 2014) to tell, where the association between gentleness and a stance of care becomes central to the plot. In all of the narratives the narrator as ‘hero’ (Gabriel, 2000) held a more powerful position, in terms of either formal authority, local knowledge or expertise, in relation to another character as the ‘object of care’ (Simpson et al., 2014a). While the examples are wide-ranging, in all the interviews being gentle was narrated as part of a positive personal strategy in an ‘epic’ (Gabriel, 2000) tale where it led to better outcomes in situations where damage might otherwise potentially have been caused or further extended to others.
In the narratives, we noticed the value given to practices that held back from active intervention (e.g. ‘being patient’, ‘waiting’, ‘going slower’ ‘going softer’), that avoided certain effects or meanings (e.g. ‘not shocking’, ‘not upsetting’, ‘not overpowering’, ‘not forcing’) and that obscured or created ambiguity about what was going on, particularly in relation to end goals (e.g. ‘taking small steps’, ‘letting people work something out and learn for themselves’, ‘prompting’, ‘letting the other lead’). We further noticed how these practices were sometimes described in ambivalent and complex ways, where suffering could not be simply alleviated, and where multiple and/or competing objectives had to be negotiated and balanced simultaneously. Narrators depicted themselves not as straightforwardly good characters (see Kociatkiewicz and Kostera, 2012) but also as compromised and/or misunderstood, in situations where their agentic intervention was somehow hidden and could not be fully and openly appreciated by others.
From the first round of narrative coding, we engaged in second rounds of focused coding (Saldaña, 2009) alongside an iterative, in-depth reading of selected literature in order to explore where narratives overlapped or broke down in relation to existing theories (see Table 2). Based on the tensions and contradictions we identified, we also reviewed other literature on organisational change, leadership and power relations to consider the potential usefulness of concepts other than care.
Comparisons and contrasts between data and extant theory.
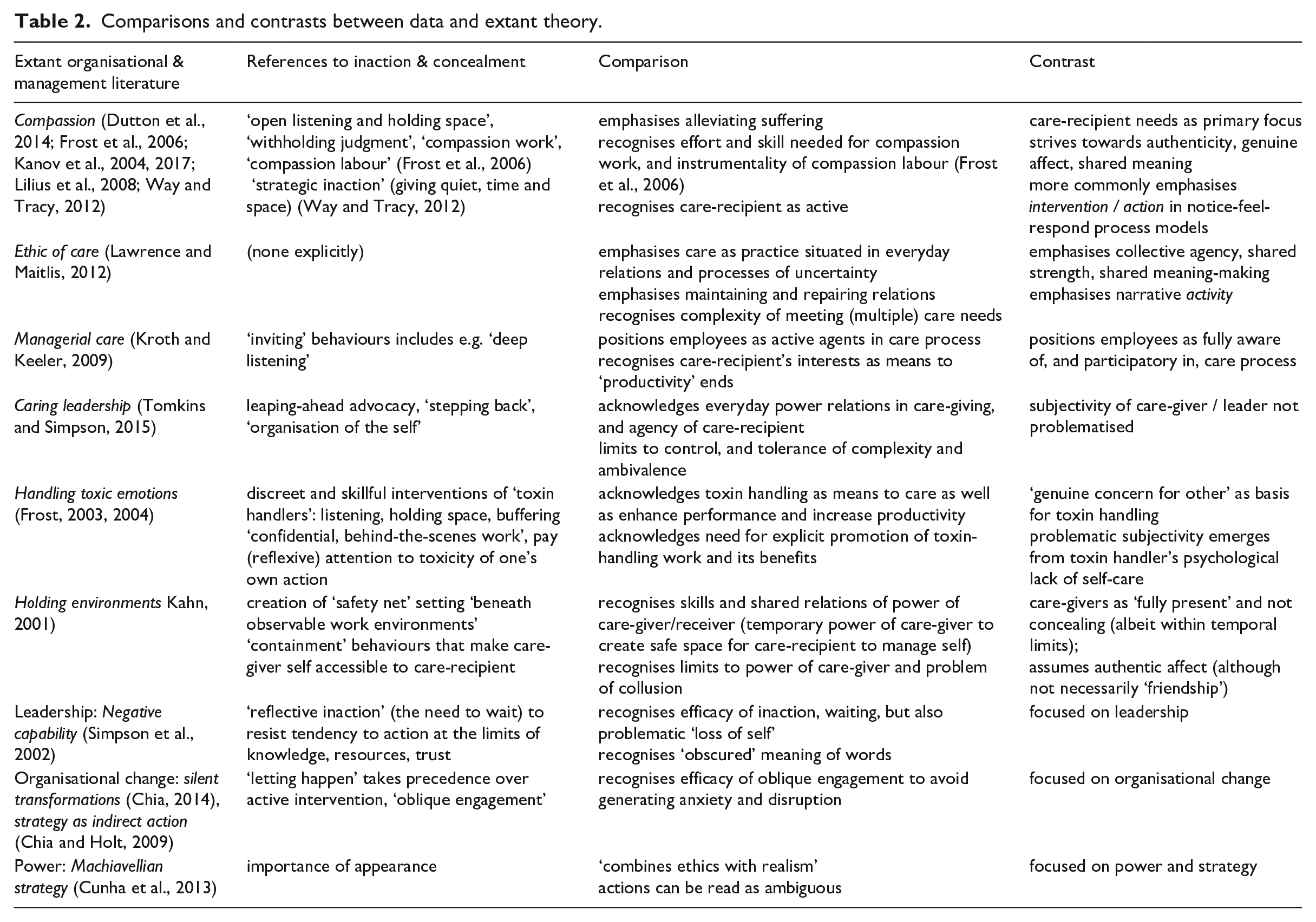
The concept of ‘veiled’ care emerged through interacting with this range of literature, where the social effects and the subjectivities generated cannot be read in simplistic ‘either/or’, good/bad dualities but rather in terms of more complex ‘and/and’ shifting interpretations (Collinson, 1994; Cunha et al., 2013). It was also informed by papers on qualitative research methodology and analysis, where what is left out of performance also creates meaning (see Mazzei, 2003; Morison and Macleod, 2014), to capture the sense of intentionality and action that the narrator constructs in the interview conversation but that is hidden from the characters within the narrative being told. We tested emerging interpretations in team conversations to explore their validity against each researcher’s readings of the dataset. The first author used NVivo computer software throughout the analytic process to store, code and analyse the data.
In the next section we summarise the data and provide illustrations to show how interviewees constructed self-reflexive practices that hold back from action and that obscure or create ambiguity about meanings as practices of veiled care. The interview extracts have been anonymised where necessary.
Narratives of veiled care
Some interviewees constructed narratives that work straightforwardly towards the other person’s best interests; others produced more complex narratives entailing more difficult, compromised goals and subjectivities, where they were working towards care-recipient interests but in more limited and constrained ways. We deal first with the more straightforward version of care that compares easily with the extant literature. A succinct example occurs in a narrative from a regional fundraising manager for a charity, who talks about being gentle with an employee who was ‘feeling particularly vulnerable’ after having been diagnosed with bipolar disorder. In the narrative, the manager emphasises how she takes time to chat, provides space for the employee to ‘open up’, and avoids being ‘gung ho’ and ‘slamming down’ with her immediate solution that the employee go on sick leave. Finally they ‘com[e] to a conclusion together’ whereby the employee will work for a while from another location where she feels ‘safer’. In our research interview, the manager describes what she was doing:
‘Listening, not over-reacting when you hear things, so trying to be quite sort of neutral but sympathetic, so not sort of raising your voice and being willing to hear what they are saying whether you agree or not. But trying hard not to show on my face how I am feeling in my head.’
The interaction with the employee arguably involves the type of care practice envisaged by Lawrence and Maitlis (2012), where shared meanings and ongoing commitments to each other are jointly co-constructed within an ethic of care. While Lawrence and Maitlis (2012) emphasise the active doing of narrative practice, here the emphasis is on the non-intervention – the lack of offering up a solution, ‘not over-reacting’, ‘not show(ing) on my face how I am feeling in my head’ – which provides space and time for the employee as care-recipient to open up in her own chosen way. She becomes positioned as an active and equal participant, with autonomy and independence, who can determine for herself the support she needs in order to be able to carry on working.
Other descriptions across interviews, such as ‘not pushing’, ‘going slowly’, ‘waiting’, listening’, ‘just sitting quietly’, and ‘not filling in the silences in order not to assume the answer’, highlight similar practices that resist intervention. They draw on negative capability (Simpson et al., 2002) to invite the care-recipient to reveal more about the issues of concern to them and to participate fully in the discussion to develop better solutions and outcomes together.
Narrators often entwine these practices of holding back from action with practices that obscure or conceal a particular social meaning and invite an alternative reading of what is going on. In particular, these soften the relational framing of the situation to obscure social cues of hierarchy, formality, control, imposition or direction. Embodied as well as linguistic resources are drawn on in the narratives, for example using ‘softer body language’ and performing emotional labour such as ‘hiding frustration’ or ‘anger’, or appearing ‘friendly’ rather than ‘frustrated’. Sociomaterial props, such as offering cups of tea or moving out of the regular workplace to a nearby cafe, invite meanings of having a break and of time away from work concerns. They invite a change in the type of conversation that might take place as workplace relations and asymmetrical hierarchies are played down.
For instance, a manager in an oil company talks about encouraging an employee to open up about her struggles at work by discursively transforming himself in the narrative from a suit-wearing ‘boss’ into a more informal and personal subject – ‘me’ – outside the usual time, dress codes and relational hierarchies of the workplace:
‘ok, I’m in shorts and a t-shirt - it’s Saturday; I’m not even at work. So, this is [interviewee’s own first name], this isn’t the boss. This is me here.’
Through these practices he invites the care-recipient to respond to him in a way other than she might have done if she were positioned more overtly as subordinate to him. He moves her struggles away from his performance evaluation of them as workplace failure.
Nevertheless, while downplaying their agentic, knowledgeable or superior positioning in the narrated interaction, many narrators still emphasise in the research interview that they remained in charge, for instance providing ‘steering’ while ‘letting [the client] have ownership’ or ‘letting [the other person] lead’. An interviewee working in a charity to support substance abusers describes using ‘questions rather than commands’ to prompt a young man into identifying and voicing for himself the solution that she had identified privately to herself beforehand: to go to a sexual health clinic for a check-up. The interviewee suggests that the client might have refused to attend if she had been more direct with her advice even though attendance would be in his best interests. The use of questions rather than commands obscures her own expertise and her guidance in the process as she leads him to arrive at the solution without explicit discussion about it.
We have focused so far on fairly straightforward narratives of care in which the goal is clearly constructed as that of furthering the interests of the other person. What is veiled here is the care-giver’s agency, authority, expertise or guidance. The veiling, produced by self-reflexive practices of inaction and concealment of particular meanings, generates space and time for the care-recipient to reveal more about the problems facing them, reflect further and more deeply upon the issues, and come to a conclusion ostensibly by themselves. It avoids socially undermining their autonomy or demeaning them as ‘objects’ of care to be directed or controlled by others.
However, there are more complex narratives where practices of inaction and concealment work towards more complex ends. For instance, a psychiatric nurse reprimands a new trainee who has acted ‘disrespectfully’ and ‘inappropriately’ (although unintentionally so) towards patients on a hospital ward. In the narrative, the nurse’s actions are driven by the need to correct the trainee’s unacceptable behaviour on the ward. It is primarily the interests of the patients and the organisation that she is addressing. However, she reconciles these with the trainee’s own interests through the way in which she seeks to correct his behaviour and repair the damage caused to others: she steps back from imposing overt disciplinary measures or punishment, and instead provides indirect ‘prompts’ for him to ‘figure out himself’ what he has done wrong, encouraging him to recognise and rectify his own mistakes:
‘He just needed the right prompts really to be able to figure that problem out for himself and I think that maintained our relationship. [. . .] It could have been a very awkward conversation but he managed the conversation with himself really, just with a bit of prompting from me.’
The trainee becomes positioned as someone capable of self-directed, voluntary learning rather than someone who needs a strong figure to direct him more overtly. The ‘prompts’ avoid the social embarrassment of ‘awkward conversations’, soften what might otherwise be interpreted as harsh, punitive and obligatory commands, and help to ‘maintain the relationship’ between the two of them.
In these more complex narratives of care, the interpersonal focus is not always on loving relations but rather relations that are more fraught. Narrators conceal negative feelings such as frustration or dislike of the other person in order to remain non-judgemental. One employee of a religious organisation, for instance, constructs himself as ‘suppressing exasperation’ as he coaches a colleague with little self-confidence who is acting incompetently. Through what he suppresses, he seeks to avoid undermining her confidence while he instructs her and helps improve her performance. Another interviewee, a senior consultant in an engineering firm, constructs a narrative that downplays a command and control style of engagement in favour of creating an interpretation of dialogue – ‘talking’ rather than ‘telling’ – with a new recruit who was not listening to what was required of him, where the consultant had to ‘keep checking’ herself as she became ‘more frustrated’ with him over time:
‘I had to choose my words very carefully and hide my true feelings and thoughts of the situation. [. . .] I stopped myself interrupting him, thought carefully before I responded and tried not to blame him, but looked at how we might resolve the issues together.’
She describes the objective for such practices:
‘I wanted to reach an amicable solution that worked for us both, I needed him on side to complete the tasks, but also because I didn’t want to offend or cause upset. [. . .] It would just have got his back up. We wouldn’t have got anywhere. There was no point going in to do battle with him.’
The self-oriented interest of the interviewee is clearly constructed within the narrative: she, as senior consultant, needs him, as junior, ‘on side to complete the tasks’. He is the means by which these ends are to be achieved. However, she is also finding a careful way of engaging with this employee, who she finds frustrating and whose performance needs to improve. The veiled practices of care are those that emerge as ‘choosing her words carefully’, ‘hiding her true feelings’, and ‘stopping herself from interrupting him’. She conceals aspects that may harm their ongoing working relationship together as she seeks to avoid a ‘battle’ with him while she tries to manage organisational tasks that are potentially about to go awry.
In summary, the narratives of being gentle highlight a set of self-reflexive practices that hold back from action and that obscure or create ambiguity about meanings in order to avoid, minimise or repair damage to others. In the next section we elaborate further on the particular subjectivities and social relations that these practices shape and the care effects they produce. We then discuss how this takes forward our understanding of enacting care in organisational life.
Discussion
With explicit reference to enacting care amid the power dynamics of everyday organising, our analysis points out that care is enacted through practices that shape social meaning, subjectivities and social relations. A key contribution of this paper is to highlight that these are shaped not only by care-giver practices that are discernible to care-recipients but also by practices that are veiled: that is, not visible to, easily recognised by, or shared with others.
Generating veiled care effects through inaction and concealment
Self-reflexive practices of veiled care produce ‘reflective inaction’ (Simpson et al., 2002: 2), where ‘doing nothing’ also produces social effects, and direct attention away from certain interpretations towards alternative readings of what is going on. These veiled practices emerge as an enactment of care when recognising the potential for damage, conflict and resistance to arise from situated struggles for meaning.
We do not suggest that practices of inaction and concealment always produce effects of care. Our data illustrates three specific ways in which they do so: by veiling negative judgements and feelings towards the care-recipient that might otherwise harm social relations; by veiling control and direction that might otherwise undermine the autonomy of the care-recipient; and by veiling the multiplicity of interests that are being played out, that include but are not necessarily limited to those of the care-recipient, and that might otherwise move the focus away from the care-recipient.
By noticing these practices, we highlight the self-reflexive techniques that shape and sustain the subjectivities that are offered as normative templates in relations of care, where care-givers are constructed as loving, attentive and standing in solidarity with others. The veiling effects invite the care-recipient to interpret the care-giver as available, seeking to pursue their best interests, and aiming to build shared futures together, while at the same time sidestepping relational issues of domination, dependency and obligation. Practices of inaction and concealment downplay knowledgeable, authoritative and interventionist dimensions of care-giver subjectivity and subordinating and instrumentalist dimensions of the care-recipient’s relationship to them.
Rather than being built from shared understanding and certainty, veiled care emerges from conditions of ambiguity and from the potential to generate alternative meanings before conflict and resistance arise. Although the care-recipient might be interpreted by the care-giver as vulnerable, failing or in need of support, this interpretation does not require open expression in social interaction. Care-recipients are not obligated to confirm some suffering status before support is provided; nor to display gratitude or indebtedness to care-givers subsequently. Instead, care-recipient subjectivity is constructed as agentic, as capable of engaging in self-directed activities of learning and recovery and of shaping their own futures without the more forceful intervention of others. As such, the practices contribute to a dynamic fluidity within care relations by avoiding fixing care-giver subjectivity as strong and agentic and care-recipient subjectivity as weak and dependent.
Power-laden ambiguities and tensions in care
The second contribution of our paper is to develop a more complex and indeterminate account of care as social practice set in power relations. This account involves conflict, tensions and an arguably less heroic goal of non-maleficence. Enacting care becomes not always entirely philanthropic, altruistic and selfless. The line between the work of caring for one person’s interests and the work of accomplishing other goals and serving other interests becomes blurred. It illustrates not a simple ‘either/or’ binary opposition – either pursuing a person’s interests or not – but a more complex and interdependent ‘both/and’ perspective, in which notions of care and power, control and delegation, one person’s interests and others’, overlap and coincide. In this account of care, both care-givers and care-recipients are agentic but they are also relationally interdependent and embedded in situations in which wider and multiple interests play out.
Veiled care presents a paradox for care-giving and for care-giver subjectivity, highlighting both the presence and the absence of power simultaneously. Successful effects of care are, at least partly, produced through the care-giver surrendering strategic control, downplaying agency, authority, expertise or knowledge, through doing nothing, allowing for a more agentic and autonomous subjectivity for the care-recipient. Yet this surrendering produces care effects by outflanking the resistance of the care-recipient. Overcoming resistance becomes part of enacting care, even while engaging with care-recipient autonomy.
Moreover, veiled care practices produce care effects only if they pass unnoticed (or at least not explicitly and openly commented on within the social interaction) 1 by the care-recipient. Care-givers cannot claim the effects as their own agentic doing: their successful negotiation of power relations, to generate situated meanings of care, may not be socially recognised, acknowledged and reciprocated since their efforts remain veiled to others. Distorting Clegg’s (1989) paradox of power, 2 the care-giver’s power (as agency) is augmented by delegation (by creating the conditions of autonomy for the care-recipient to act), but in this case the ‘rules’ of delegation (that the care-giver has the authority to grant autonomy in the first place) are not recognised.
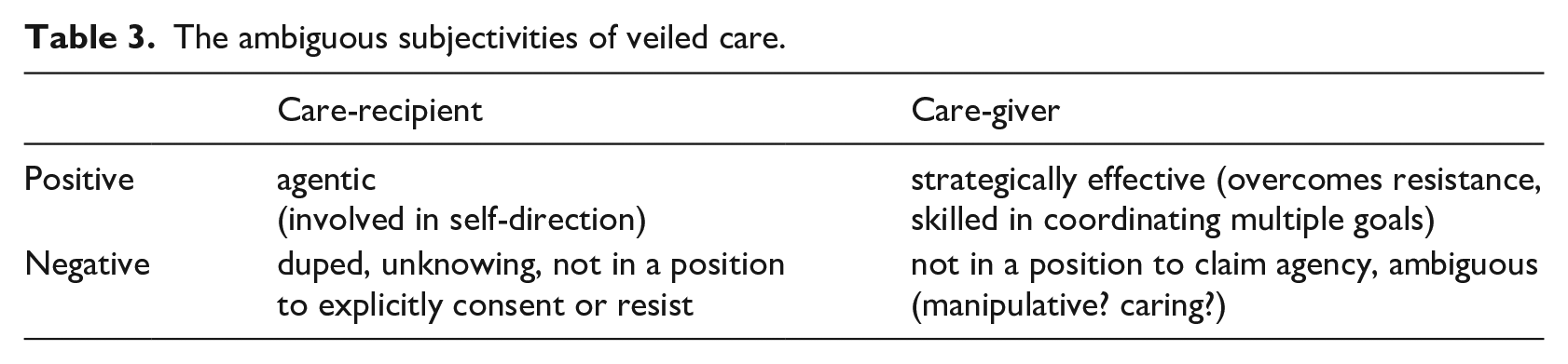
Veiled care generates difficulties for care-giver subjectivity: either the care-giver’s skilled accomplishment of care effects is not recognised, or else it produces disquiet either about its adequacy (inasmuch as it does not put first clearly the needs of the care-recipient) or about its lack of transparency or authenticity (that dupes the care-recipient and bars them from open debate about their interests and needs) (see Table 3).
The ambiguous subjectivities of veiled care.
Ironically, veiled care may fit well with the subjectivities of care-giving professionals in sites such as care homes or hospices: in these sites, pursuing the other’s interests is assumed as one of the organisational goals to be accomplished, and social constructions of professional expertise are more closely predicated upon, and entwined with, producing care effects for others. However, subjectivities in other occupational settings, where care is not such a central focus, risk emerging not only less clearly as caring but also less clearly as agentic.
Some might argue, importantly, that the concept of care here is compromised since the sole reference point is not the care-recipient. The focus is not solely upon their own determination of their needs and interests, nor their own responsiveness (including resistance rather than consent) as the means to determine if these needs and interests are met. Nevertheless, our analysis raises what might be deemed a less worthy, less heroic but nonetheless important goal of care, of avoiding maleficence (Molterer et al., 2019). Veiled care highlights the importance of non-maleficence – to avoid, minimise or repair damage – as much as beneficence as a goal of care in work relations. This situates care in activities that simply seek to do no harm in difficult circumstances, through seeking the ‘practical wisdom’ (Bardon et al., 2017) to navigate everyday organising carefully. Care-giving practices become important precisely through recognising the tensions that workers are navigating, that might otherwise cause damage, as they seek to reconcile various interests and work goals. Now enacting care brings together an ethic of care that attends to individual care-recipients with an ethic of justice that aims to treat everyone fairly and with respect. It engages with difficult social relations and emotions, not just with others who are loving or deserving. The essential skills now required to accomplish care overlap with those of the type identified by Fineman (2006: 275): skills to ‘steer through’ the dilemmas of ‘competing possibilities and differing voices’ in ‘emotionally ambiguous circumstances’.
Concluding comments
In this paper, we have been inspired by interview narratives of being gentle at work to develop the concept of veiled care as self-reflexive practices that hold back from action and that conceal meaning in order to avoid, repair or minimise damage to others. The concept extends and develops the understanding of care as social practice enacted in everyday organisational life.
Our focus on veiled care highlights some strategic aspects of care-giving – that is, how to accomplish care in local context. It points out that what is not shared between care-giver and care-recipient creates care effects, and how negotiating contested meaning and overcoming resistance are involved in enacting care. This extends a consideration of care into situations where workers must address multiple needs and interests, and where other people as colleagues and subordinates are not only an ends in themselves but also a means to achieve other goals.
While this account shows care as ambiguous and sometimes compromised, it is important to consider self-reflexive practices of inaction and concealment within a framework of care in order not to praise the potentially ideal at the expense of what is hidden in plain sight in everyday work relations. The personal skill of avoiding, repairing or minimising damage in organisational life is too easily unnoticed if done well through subtle, non-disturbing means. Veiled care is easy to miss but would be missed if absent.
Footnotes
Acknowledgements
We would like to thank Raza Mir and two anonymous reviewers for their helpful and constructive comments that have shaped this paper in its final form. An early version of the paper was presented at the EGOS conference (sub-theme 11), Copenhagen, 2017. We acknowledge the part played by Katie Balling, a postgraduate student at the Alliance Manchester Business School (AMBS) who conducted some of the interviews upon which the paper is based. We would also like to thank the other interview participants from a range of health and social care and other settings.
Funding
The study on employee gentleness was supported by Lord Alliance funding at AMBS, University of Manchester.