
Abstract
This paper reports the findings of a qualitative study on lean implementation viewed as an organisational learning process. By using a scaffolding framework, we investigate the ways in which human resource development facilitates learning among clinicians. This study contributes to the temporary role of human resource development in learning processes within multi-disciplinary professional groups. We identify scaffolding activities from which we have identified three human resource development practices: phase 1 – cognitive scaffolding, in which human resource development acts as a ‘mindsetter’ that aims to motivate the learning of lean in relation to the clinicians’ practices; phase 2 – peer-to-peer scaffolding through ‘doing’ lean, in which human resource development performs the role of an ‘experience creator’ who creates knowledge engagement between peers – in order to put lean into practice; and phase 3 – fading of the scaffolding, in which human resource development performs the role of a ‘delegator’ who transfers the responsibility to the clinicians to promote learning. This contributes to our understanding of how knowledge is negotiated in a multidisciplinary context. We contribute to the learning literature by emphasising how learning trajectories are initiated by learning initiatives, highlighting the role limitations of human resource development in this context, and demonstrating how a new learning tension arises between different versions of ‘lean’ in the organisation.
Introduction
Official efforts to contribute to innovation, change and organisational learning are a key characteristic of current organisations (Corradi et al., 2010; Strønen et al., 2017). This is a study of the role of Human Resource Development (HRD) in the implementation of lean thinking in a hospital setting. By HRD we mean HR staff facilitating learning (Hamlin and Stewart, 2011). We use this definition as the facilitator of lean implementation is part of the HR department working with training, coaching and facilitating the learning processes, all key characteristics of HRD (Hamlin and Stewart, 2011). Lean management is a popular improvement philosophy stressing five principles: Identifying customer values (in this case, the patient), mapping processes that create value (e.g. the value stream), refining work processes to create a (better) workflow, producing the value that is actually needed and nothing else and, finally, achieving perfection by constantly practicing the principles (Alagaraja, 2014).
Elkjaer (2022) suggests that more studies should make connections between learning and other organisational processes. In this case, we link organisational learning to lean management, although they barely mention each other (Stimec, 2020). This connection of literatures is of particular interest because it addresses temporary learning activities between the individual and the organisation. While organisational learning theories stress organisational control, adult learning theories emphasise the needs of the experience oriented learners (Knowles et al., 2014).
This study contributes to our understanding of the temporary role of HRD in organisational learning processes in multidisciplinary professional groups. A specific gap is addressed concerning the ways in which HRD develops a shared ‘lean mind-set’ in relation to adult learning (Knowles et al., 2014). Adult learning theory emphasises purpose in order for learning to be useful. The learning itself must make use of the learners’ personal experiences and make sense in relation to these. In HRD, organisational control takes priority in the learning environment; conversely, individual control is emphasised in adult learning theories (Knowles et al., 2014).
The role of HRD in this article is seen from a social view of knowledge and learning (Vygotsky, 1978). Social learning theories applied to adults integrate the concept of behaviour modelling with cognitive learning in order to strengthen the understanding of task performance (Mukhalalati and Taylor, 2019). In such cases, HRD works with autonomous clinicians who might resist or take control of the learning process when engaged in this multidisciplinary lean learning process (Mäkinen, 2022; Mørk et al., 2010; Thompson, 2005).
Our research question is as follows: What is the role of HRD in the lean learning processes of hospital clinicians? To discuss this research question, we identify scaffolding activities from which we further identify HRD roles. This contributes to our understanding of how new and existing experiences are used to motivate learning (Knowles et al., 2014) and how knowledge is negotiated in a multidisciplinary context (Mäkinen, 2022; Mørk et al., 2010). The framework we call scaffolding is adapted from social cultural learning theory (Vygotsky, 1978) and the extension made by Wenger (1998) in his work on communities of practice. Scaffolding is a metaphor that describes HRD’s temporary learning activities. The clinicians in the hospital are viewed as needing temporary support in the same way that the construction of a complex structure requires the use of scaffolding to support each successive phase of a building project (Roberts and Beamish, 2017).
In the following we introduce a ‘third way’ of seeing organisational learning (Elkjaer, 2004) that combines a cognitive and practice perspective. Building on this, we elaborate on the concept of scaffolding (Vygotsky, 1978) and, in doing so, we highlight the ways in which this framework can address cognitive, social and practice-based elements in an adult learning process, including the role of emotions in learning. The main part of the paper, however, is devoted to our methods and empirical findings on HRD in relation to learning in this study. In the conclusion section, we summarise our contributions and limitations.
Literature review
In the following, we will account for the theoretical perspectives related to HRD as a scaffold and how this function assists in the lean and organisational learning process.
Organisational learning
In relation to lean thinking, learning can be thought of as ‘the detection and correction of error’ (Argyris and Schön, 1978), where an error is anything that prevents clinicians from taking effective action when working. The successful implementation of lean requires clinicians to be effective problem solvers and learners (Mazur et al., 2019) on behalf of an organisation. The cognitive perspective on organisational learning uses the concept of ‘theories of action’ to point to mental representations, often called mental schemes of actions, as the most important phrase for understanding organisational learning (Argyris and Schön, 1978; Elkjaer and Brandi, 2014). Seen from this perspective, learning is related to individuals’ abilities to change their theories of actions accordingly. In the work of Argyris and Schön (Elkjaer and Brandi, 2014), understanding organisations as ‘learning systems’ frames organisational learning and can be viewed through the ‘acquisition metaphor’ (Elkjaer, 2004; Sfard, 1998). This emphasises the role of individuals in the learning organisation, individuals who acquire skills and knowledge so that organisations can learn. From the perspective of adult learning (Knowles et al., 2014), existing knowledge, experience and of learner motivation are crucial, as it shapes the learning experience.
The practice-based perspective on organisational learning focuses on ‘doings’ and organisations as communities of practice (Brown and Duguid, 2001; Corradi et al., 2010; Gherardi, 2017; Gherardi and Nicolini, 2002), and can be viewed using the ‘participation metaphor’ (Elkjaer, 2004; Sfard, 1998). This means that knowing is a social and organisational activity – socially constructed through interactions in particular contexts (Newell et al., 2009). Practice has primacy in the social construction process, since practice produces organisational reality (Feldman and Orlikowski, 2011) and is the curriculum for learning (Hawkins et al., 2017). HRD from this perspective is about helping learners access practice. Other scholars have tried to combine the two perspectives. The mutual constitution view (Cook and Brown, 1999) regards knowledge and knowing (working knowledge) as ‘things’ that are complementary, and these two dimensions of knowledge can be used at different organisational levels (i.e. knowledge is possessed by individuals; knowing is socially created in practice). One criticism of the cognitive perspective from a practice-based perspective is that if learning begins with a change in mental models, how then is it possible to learn from practice and practising, that is, from the body and emotions? (Cook and Yanow, 1993). There is a renewed interest in how emotions affect organisational learning (Filstad, 2010; Gherardi, 2017) that emphasises that emotions are an inevitable part of learning, both as a product and as part of the process. Elkjaer (2004) suggests a ‘third way’ in which the content of the learning process is the development of experience, thinking and reflection, which may result in relevant organisational knowledge, where both individual and organisations are products and producers of human beings and knowledge. Based on this, the purpose of HRD is to develop experience in relation to problems or issues at work, while also stimulating thinking as a tool for acting (Kim and Ko, 2014).
Tensions between organisational learning and professional learning
The literature describes a tension between professional learning and organisational learning, in which the professional can hinder the learning capacity of the organisation (Elkjaer and Brandi, 2014). The problem is that these two learning processes are not the same and sometimes not linked. Cognitive learning theories solve this problem by linking them as single-loop and double-loop learning, such as when nurse practitioners employ existing structures and systems of care delivery and challenge existing systems (Elkjaer and Brandi, 2014). This is achieved by emphasising the needs of the patient instead of only following system procedures (Dewan and Norcini, 2019; Swan et al., 2007). The last form of thinking, which corresponds to double-loop learning, is the reconceptualisation of patient care and services.
As HR is an ongoing process, in line with the learning process, attention to HR can have an important place in learning organisations, because HR must exercise different roles to respond to the varied needs for support in the learning processes (Tanjung, 2020). The literature on communities of practice underlines that organisational learning takes place in informal arenas in which HRD attempts to influence the learning processes through different roles (Hwang, 2019). HRD activities that promote learning could negatively impact these informal learning processes if uncontrolled (Thompson, 2005). However, the processes and structures of a community of practice are emerging (Hawkins et al., 2017), and official initiatives could be good vehicles for developing structures within and across communities that can improve organisational learning (Pyrko et al., 2019). Elkjaer (2004) suggests that organisational learning should be viewed as learning that takes place in different organisational arenas: professional and/or community arenas, and other arenas – managed or formal arenas such as a lean process and those where clinicians interact with patients.
Organisational learning through lean in health care
The concept of ‘lean’ has its origins in Toyota’s success with efficiency and quality production. Those companies that adapted these improvement methods to contexts beyond manufacturing tended to use the term ‘lean’ to describe its more extensive application (Plsek, 2013). Lean is a process improvement tool to solve problems with quality, capacity and efficiency and is applicable to many organisations including the health sector (Ruiz and Ortiz, 2016). Lean aims to improve quality by reducing waste and facilitating value flow. Examples include value stream mapping, which focuses on mapping and eliminating activities that do not add value. This means that change takes place continuously, where new solutions to existing problems are identified. This relates to our understanding of knowledge or knowing, whereby knowing is something you use and therefore reshape (Andersen and Røvik, 2015).
However, the health sector context offers many barriers, the most important of which comprise a lack of commitment and support from top management, multidisciplinary collaboration, training and communication (Ruiz and Ortiz, 2016). At the same time, the health sector has its own institutional modus, driven by distinctive clinical service demands, regulatory requirements and close political and public examination (Bresnen et al., 2017). When lean has been introduced to processes in this context, it has been noted that tension often arises between the medical mind-set and the lean approach (Mazur et al., 2015). Lean thinking in a medical environment can therefore be challenging as clinicians require evidence before taking action (Andersen and Røvik, 2015). This is because the medical mind-set is research based, whereby validity, reliability and proof of results are crucial to implement new changes (Plsek, 2013). In comparison, lean methods are largely experience based, thus research has less influence on methodological development. This different approach may result in resistance to change, which makes it particularly difficult to use in convincing doctors, who have traditionally had a greater focus on research (Stanton et al., 2014).
Nevertheless, social science research has shown that the lean philosophy provides principles and practices that can rejuvenate innovation capability (Lins et al., 2021). Research also shows that lean thinking in the health sector can deliver extraordinary savings in terms of lives and ‘dollars’ (Stanton et al., 2014). From an industrial perspective, lean thinking can be suited to the hospital sector. For example, in the automotive industry, different components must be used to create a product; the same principle applies to patients in hospital. They are admitted and subjected to several stages in order to receive the help and treatment they need – before being discharged from the hospital (Mazur et al., 2015).
For lean methodology to work, a bottom-up approach is emphasised (Stanton et al., 2014). This is because lean methodology is based on the employees having the solutions; therefore, they must own the process (Plsek, 2013). However, when it comes to clinicians, they often become too close to their own profession and subject area (Hamlin, 2002), meaning they lose the holistic focus that is necessary to support the entire innovation process (Dewan and Norcini, 2019; Mufeed, 2006). Change processes in the health sector needs actors who manage to be the centre point where strategy, culture and management overlap (Oborn et al., 2013) These areas are the particular focus of HRD and therefore offer interventions such as coaching, mentoring and specific developmental processes (Iles et al., 2010). Based on this, HRD can play an important role in helping managers and employees recognise and appreciate external and internal knowledge (Currie and Kerrin, 2003; Trullen and Valverde, 2017). This is also emphasised by Stanton et al. (2014), who argue that HRD can play an important role in motivating employees to use the lean technique. This is because HRD is a resource that exists outside a department yet understands the operation of the entire organisation. By using HRD as an up-front man, management plays a more background role, creating more leeway for employees – which contributes to increased commitment and a sense of belonging to the process. Thus, it is emphasised that HRD can and will play a useful role in the initial phase of lean implementation (Stanton et al., 2014). HRD can be regarded as an organisation’s facilitator that connects people and their knowledge with organisational goals. The scaffolding concept offers ways of seeing HRD activities that can help us to better understand HRD’s role in organisational learning processes; hence, we will now explore it in greater detail.
‘Scaffolding’ organisational learning
A key idea in Vygotsky’s (1978) social learning theory is ‘the zone of proximal development’, which describes the distance between what a learner is capable of doing without support and what they are capable of doing with support. This support is used synonymously with the term scaffolding (Bruner, 1990), which entails helping learners complete only those elements that are within their range of expertise. Scaffolding works best when learning participants share and experience intersubjectivity, working together towards the same goal, helping each other to develop new knowledge. The learning takes place both individually and through social interaction and dialogue, which results in new understandings and further learning. Vygotsky’s (1978) ideas are developed further in Wenger’s (1998) community of practice, where the apprentice gradually learns from receiving new tasks, accomplishing them and receiving more difficult tasks when ready, supported by a supervisor.
Scaffolding was originally a pedagogical framework that focused on expanding the possibilities for learning. Cognitive scaffolding, more specifically, takes place when the learners’ perceptions are changed by enactive representation (Bruner, 1990). The activity facilitates hands-on experiences and real-world applications, which make the knowledge more understandable. Analytically, the framework is used in this article to clarify the interplay between cognitive ideas and practice-based experiences in learning processes through the concepts of cognitive (idea) scaffolding and peer-to-peer scaffolding (experience, practice). It also includes emotional scaffolding such as giving emotional support or creating a positive atmosphere (Meyer and Turner, 2006). Moreover, scaffolding reduces anxiety and guides learners to interact with their peers and provide feedback (Roberts and Beamish, 2017; Vygotsky, 1978).
The scaffolding concept offers ways of seeing HRD activities that can help us to better perceive HRD in organisational learning processes. When we use the term scaffolding, we look at facilitation as a learning process that involves building a “space” that promotes new understanding (Roberts and Beamish, 2017), although this understanding is not so far removed from the recipient (in this case, the recipients are the medical professionals involved in the lean project). Ideally, it is entirely within the recipient’s ability to recognise and value knowledge, but it is also unfamiliar enough to seem challenging (Vygotsky, 1978). Thus, the facilitator’s role in such a perspective is to frame the understanding closely enough to the recipients so that they can understand and integrate their existing skills or experiences. For scaffolding to take place, it must be possible for HRD to identify the participants’ skills and knowledge, so that HRD has the opportunity to help the participants at their current level (Jin and Navare, 2010). In other words – facilitation regarded as scaffolding means a link between two constantly changing conditions – the understanding that is developed among the participants and the understanding of the participants that is developed by the facilitator (Warford, 2011). This approach is comparable with situational leadership (Blanchard and Hersey, 1996) that builds the confidence of employees and the necessary skills to be ready, willing and able to meet the expectations of a task and also facilitate positive employee perceptions of experienced meaningfulness, responsibility and knowledge. On the one hand, soft scaffolding comprises the facilitation of interactive discussions and guidance from, in this case, HRD, and such soft scaffolding comprises dynamic, situation-specific aid given to help with the adult learning process (Knowles et al., 2014). Scaffolding requires HRD to continuously diagnose the understanding of learners and provide timely support based on the learners’ responses (Weber and Feintzeig, 2014). This type of assistance is generally provided “on the fly”, and comprises support or guidance that is given when needed. Soft scaffolding also has some normative statements, such as promoting a form of collaboration that respects the participants’ rights to autonomy and discretion, while ensuring the effective exercise of those rights as a part of an interactive and supportive process. Hard scaffolding, on the other hand, is static support that can be anticipated and planned in advance based on the typical difficulties of a task (Brush and Saye, 2002). In an organisational context this could be learning activities that are more structured by narrowing the discussions to include certain tasks and issues in relation to the organisational goals that promote more disciplined arguments and interactions among the learners (Hawkins et al., 2017).
Fading of the scaffold for organisational learning
The last but no less important aspect of scaffolding is the fading of the scaffold. The nature of scaffolding indicates that fading can be problematic. If the scaffold is removed too soon, everything could fall apart, but if it is removed too late, there is a danger that the learners are unable to control their own learning (Tawfik et al., 2018). Fading starts early. The way in which the process is set up is often hard first and then softened later when the participants are mature enough to take the work further themselves. What is fading about? Noroozi et al. (2018) state that fading is a dynamic activity in which the scaffolder adjusts the degree of fading based on the needs of an organisation’s members. This means that fading is about distinguishing between the wishes of an organisation’s members and their need for support – and the scaffolder must allow for failure without assisting. This fading activity is called ‘adaptive fading’. In the context of this study, it can be about not discussing lean so much and not providing existing examples or tools, only encouraging clinicians to find their own solutions with lean – handing over responsibility to them. This can be a smooth process in which the clinicians take responsibility and practice lean in a way that supports their needs, a ‘crash landing’ for those clinicians who are unable to put new ideas into practice since what previously seemed clear now seems more complicated, or a passive process in which the non-presence of interaction and dialogue describes the process further (Molloy et al., 2014).
Methodology
This paper is based on a single case study. By obtaining in-depth insights into data through interviews, observation and archival data, we provide a more nuanced perspective on HRD’s temporary role in a distributed innovation process (Gerring, 2004; Yin, 2017). The research case was selected according to two criteria: first, HRD had to have a role in the research case in order to highlight how HRD assists in the innovation process, and second, the research case had to give us important insights into the role of HRD in scaffolding learning and innovation. Thus, the selected research case had to be described as a success.
Empirical context
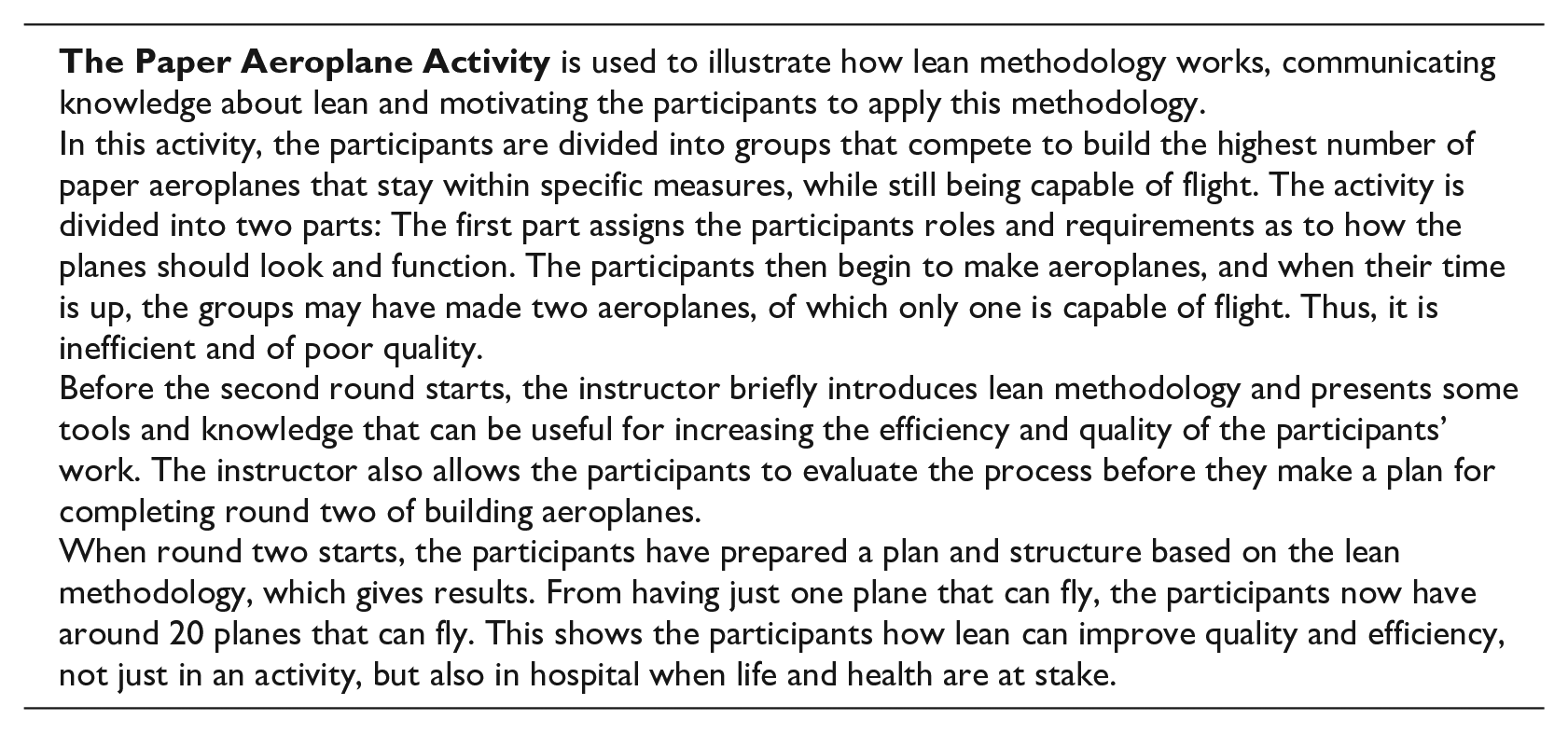
We used a hospital to obtain the empirical data. This is a hospital with 10,000 employees divided into 9 divisions, each with its own budget and located in approximately 40 locations in 2 different counties in Norway. The organisation has a centralised HR structure with around 60 employees; some divisions have locally located HR, while in other divisions HR is geographically dispersed. Due to this centralisation, HR becomes an important link between divisions and departments, particularly in terms of spreading ideas and knowledge between actors, as well as knowledge creation and the development of new practices. We have chosen to focus on one specific lean project at Lillehammer Hospital. The project was selected because it is regarded as a great success and has the potential to assist us in better understanding how HRD can play an important role in organisational learning in hospitals. Initially, a paper aeroplane activity was chosen due to its ability to illustrate how effective learning processes can change medical practice. This research case is particularly interesting since hospitals are staffed by various professions who might resist any change in practice.
Lean was introduced at the hospital in 2009, and HRD was involved from 2012 to ensure better training. Over the years, lean has been introduced to several medical fields such as back problems, cancer treatment and the treatment of femoral neck fractures. In 2016, the hospital received an award for excellent lean implementation. Around 50 people from the hospital were involved in the lean process, and several of them were trained in lean methodology. Managers, doctors, nurses, porters and other staff participated in this training, meaning that the whole value stream was included. Initially, two pilot projects from the surgery department were selected for this project: one was a back operation, called the ‘back pilot’; the other was emergency surgery for a thigh fracture, called the ‘thigh fracture pilot’. These two pilot projects were successful since the waiting time for the patients was significantly reduced as it was important to operate quickly in these cases. Thus, the quality was also improved. A project that resulted in the hospital winning a lean award on a recognised lean forum was thrombolysis, the process of treating stroke patients. In the case of stroke patients, every second counts to reduce severe side effects and even avert death. After this project, the hospital succeeded in reducing the waiting time for surgery for stroke patients by more than 50%, from an average of 74 minutes to 20–30 minutes, which means months of less rehabilitation and, for some patients, survival.
Data collection
The data consist of 10 qualitative interviews, 5 observations and the analysis of 91 documents. The first author initially engaged in the learning process in 2017, when he observed the paper aeroplane activity and subsequently participated alongside clinicians, gaining a practical understanding of this activity. In 2018, he participated in lean meetings as an observer and followed up with five interviews in 2019 and a further five in 2020. The HRD facilitator and head of a medical unit were interviewed twice, in 2018 and 2019, to better grasp the processes of learning.
The process of interviewing gave us the opportunity to understand the perspectives of the participants in the study. The observations were also used to gain a thorough understanding of the research setting and the participants in the study. The document analysis, in turn, contributed to a deeper understanding of certain aspects of the empirical research and helped to verify some of the findings.
Interviews
We used semi-structured interviews because this is a flexible design that allows for detailed descriptions of practice (Gubrium and Holstein, 1997). The interviews lasted between 70 and 90 minutes. When selecting the informants, we chose Marshall’s (1996) principles, which focus on selecting informants who can illuminate the research case to the greatest extent. Based on this, interviews were conducted with 10 informants with different backgrounds in the hospital: one from HRD, one HR director, one project manager, three doctors, three nurses and one line manager. As these individuals have different backgrounds both professionally and organisationally, they will be more capable of providing a full picture of the complex lean project and how HRD affected the process.
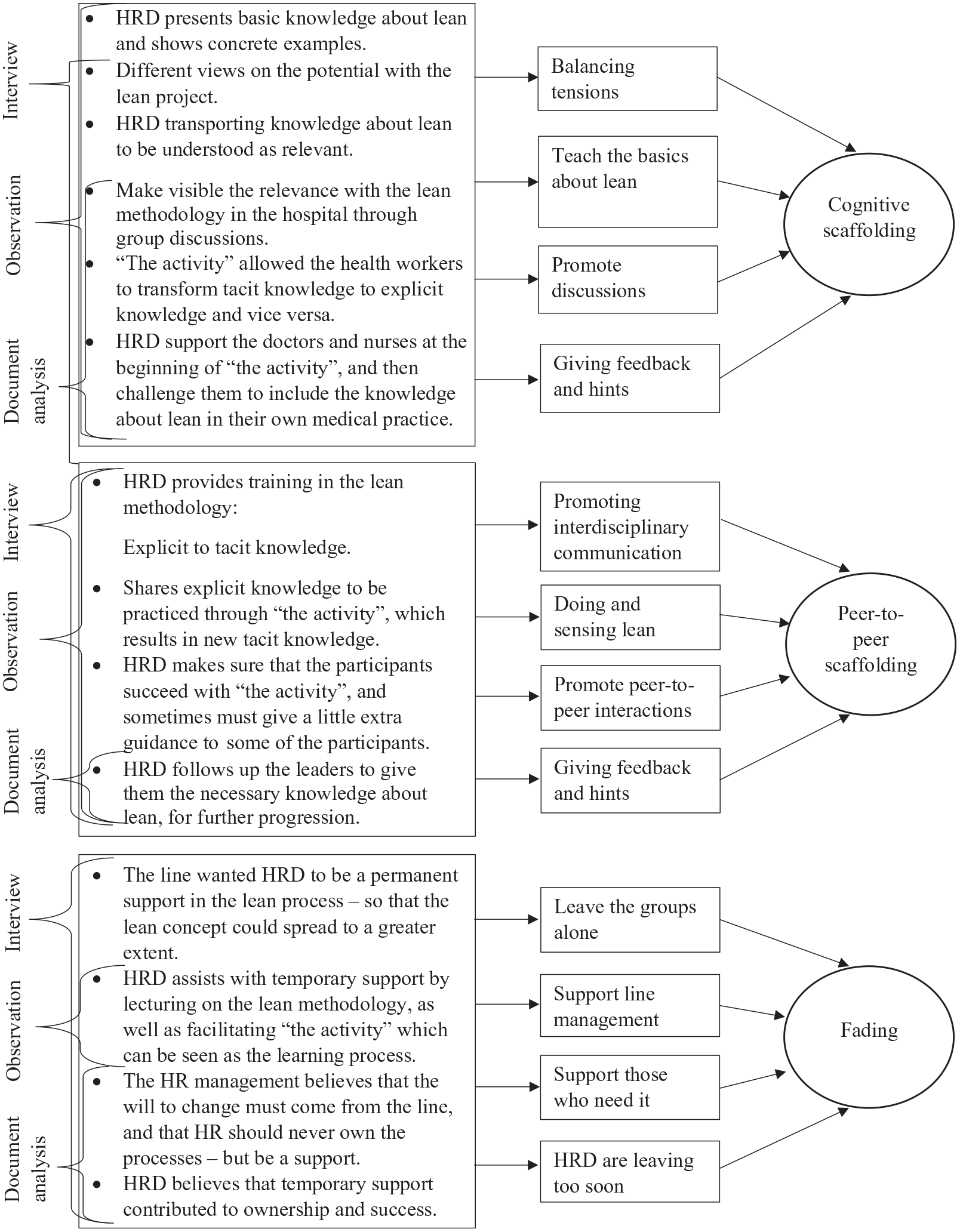
The interviews were transcribed verbatim, and we read through the transcripts and conducted individual analyses. We then compared the findings to find overlapping ideas. Next, we coded the material using a step-by-step process in which we gradually reduced our focus to three codes: cognitive scaffolding, peer-to-peer scaffolding and fading (see Table 1). In this way, our theoretical contributions are closely related to the data.
Categorisation.
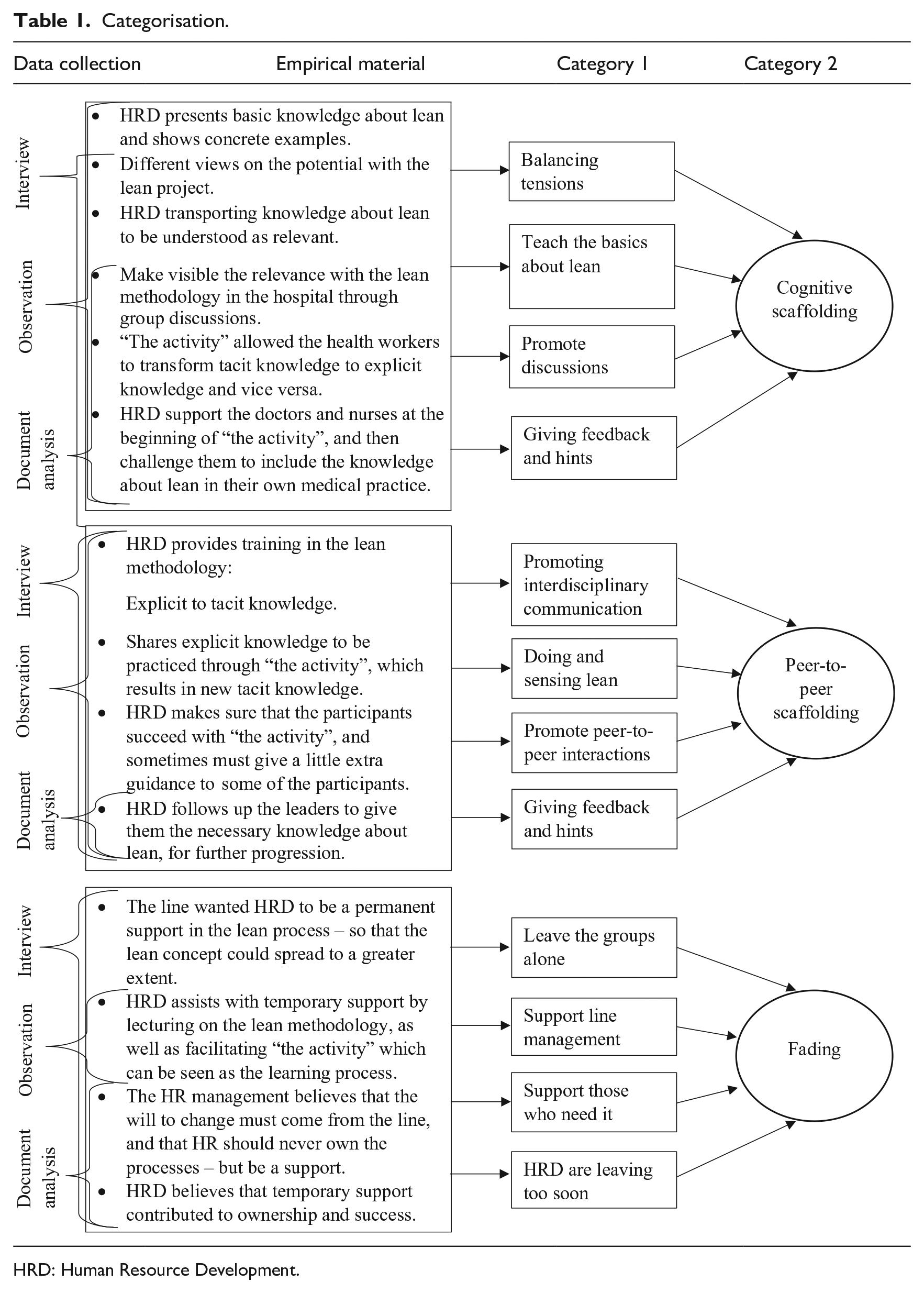
HRD: Human Resource Development.
Document data
In order to ensure the validity of the findings, document data were used to gain in-depth insights (Pershing, 2002). The document data consist of project documents, paper aeroplane activity documents and presentations. This document review provided deeper insights into certain areas, which supplemented the interview data.
The document data were read and roughly sorted based on what the individual author regarded as necessary background material. We then made a joint assessment of the document data and divided them into different topics. After we had achieved an overview of the document data, we were able to code the material. This coding was initially conducted by the first author, after which the second author looked over the codes and provided input and his assessments – thereby ensuring the validity of our findings.
Observation
Through the data collected from interviews and document analysis, we noted that HRD played an important role in collecting and developing knowledge about lean and its ideals, demonstrating this through something HRD called the ‘paper aeroplane activity’. To gain better insights into this activity, and to understand how HRD assisted in sharing knowledge, participant observation was used as an additional methodology (Tellis, 1997). HRD was observed in collaboration with other managers and through interaction with clinicians during lectures and discussions, the paper aeroplane activity and follow-up meetings, in which the number of participants could vary from 8 to 15. These observations provided additional in-depth insights into the study’s process.
Analysis technique
The process of data collection and analysis was conducted iteratively and allowed themes to emerge from the empirical material which could then be examined in greater depth from a theoretical perspective (Corbin and Strauss, 2008). This means that we have developed our categories from the empirical data but used the literature on scaffolding to reflect on our data when labelling the categories (see Table 1).
Overall, the interviews, document analysis and observations helped to strengthen the breadth and depth of the data, which has provided us with an increased understanding of HRD in the learning process. As can be seen from Table 1, the interviews were a most important methodological technique because we had the opportunity to challenge the informants’ responses to gain more in-depth insights into the learning process. The interviews have also given us several questions that emerged during the document analysis. Regarding the document analysis, it provided us with increased insights into the contextual factors of the learning process. The document analysis was also important in verifying certain findings, while in other areas it provided fewer insights. For example, many documents confirm that HRD was involved in the learning process and assisted with operational and strategic tasks. However, few documents were able to verify how HRD as a scaffold manages these operational and strategic tasks. Thus, observation was a useful tool for uncovering the informants’ habits, tacit skills and practices (Zahle, 2012). In this way, we gained more insights into how HRD was used as a scaffold. In particular, observations have been important to understand how the paper aeroplane activity influenced the motivation and support for the lean project. The observations also helped us ascertain how HRD must adapt to the motivation, skill level and academic weight of the different participants.
Taken together, the methodological techniques have provided a complex picture of the contextual frameworks that we have researched, as well as provided deeper insights into how HRD can assist in complex medical innovation processes.
Findings and analysis
As Table 1 shows, we have reduced the content of our empirical data to three categories or practices: cognitive, peer-to-peer by using embodied knowledge, and, finally, the last stage of scaffolding – fading – in which HRD fades its support and the processes. While the two first phases can be regarded as a success, fading demonstrates that there is a learning tension between learning at the individual and group level and organisational learning. We will now elaborate on the findings in each category.
Phase 1: cognitive scaffolding – creating a lean mind-set
The first practice identified, which covers phase 1, is creating a lean mind-set among the participating clinicians through a lecture on lean methodology followed by a discussion among the participants who attended the lecture. This phase describes the planning, initial meetings and training activities in 2017.
The first scaffolding activity in this practice is about reducing the doctors’ influence and creating a positive atmosphere for discussing the lean mind-set by structuring the meetings. To achieve this, HRD organised the groups of clinicians comprising doctors, nurses, ambulance workers, line managers and porters into groups numbering 10–15 people. HRD also carefully assigned the medical doctors to different groups in order to avoid the doctors becoming too dominant in defining lean in each group. One informant stated,
It was a puzzle that had to be pieced together before we could complete the game [paper aeroplane activity]. We knew there were a number of sceptics among us, so it was important to particularly focus on the doctors. Why? Because they have professional integrity, influence and power in the organisation. Moreover, they were the ones who were most skeptical. (Head of Department)
The second activity in this practice involved teaching the basics of lean. HRD used a PowerPoint presentation to describe lean. The presentation was made to each group for 60 minutes. One of the informants stated,
[HRD] was very educational and good at explaining the knowledge and mindset regarding lean and they [HRD] did a great job with the managers and employees. Because of [HRD], people quickly understood this lean thinking. I was responsible for the evaluation forms and it scored quite well. (Divisional advisor)
In order to convince the doctors, it became important to focus on how lean contributes to quality improvements. As doctors are primarily concerned about the medical profession, it became important to focus on how lean contributes to increased quality, patient safety and professional development. This activity combined various efforts that attempted to persuade the doctors to change their minds about lean. First, HRD presented lean methodology used by well-known and highly rated organisations. However, management-like terms such as finances, efficiency and savings were avoided. Instead, HRD focused its attention on how lean could promote patient safety rather than finances. Based on our observation data from the meetings, we could tell that this approach was adopted to make the doctors more positive about lean.
Nevertheless, the doctors showed resistance, which manifested itself in various ways. Some doctors looked at their mobile phones, some sat cross-legged and shook their heads, while others asked critical questions. However, other participants, such as the nurses and managers, clearly responded differently than the doctors, leaning forward, nodding, asking questions and showing their interest and eagerness to learn more about the opportunities of lean. They made it clear to everyone that they saw lean as an opportunity to improve a system that they regarded as inefficient and costly.
The third activity in the scaffolding practice during this phase was to combat the doctor’s resistance to this lean project. By resistance, we mean a lack of willingness to engage themselves with lean. This resistance was based on a preconception that lean was a management project that was only aimed at reducing costs. This resistance was resolved by getting other clinical peers, who understood the opportunities offered by lean, to talk to the sceptical doctors. This was because HRD had little professional authority and influence among the doctors, and it was therefore crucial to use these group discussions in which the doctors could receive input from other health professionals who were able to influence them. In this way, the group discussions helped to reduce the doctors’ resistance to lean:
At first I was sceptical, and I also stated this during the lectures. However, during the group discussions I understood my colleagues’ views about lean and how much waiting was involved with a patient who had a femoral neck fracture. This probably helped reduce some of my resistance, but my scepticism was still there. I didn’t realise at the time that someone was waiting for me. Instead of operating on a patient the day after the fracture, I was now able to operate only hours after the fracture. So, in retrospect, I’m glad I changed my views about lean. I must admit that I was quite resistant in the first weeks of the project. When I saw that lean could provide added value for the patient, I became more involved in the process. (Doctor)
HRD had pedagogical skills, which were highlighted as an important factor in the participants’ evaluation forms. Several of our informants told us that HRD received high scores on the evaluation after the lean sessions. HRD played an important role in this first phase of the innovation process in which HRD’s most important task was to unite the professional groups in a mutual understanding of the lean concept:
The tension between the medical mindset and the lean philosophy can be described as follows: “Show me the figures, but don’t tell me how I should manage my day. (Head of Medical Unit)
This quote illustrates the doctors’ research-based mind-set (Plsek, 2013), but the doctors also emphasise their autonomy. However, by focusing on treatment, HRD was able to focus the doctors’ attention on workflow and the value for the patient. A doctor stated the following: ‘The medical treatment issues were focused and I therefore think it was easier for HR to get our attention’ (doctor).
In our view, HRD contributed to success by allowing the doctors to emphasise their professional knowledge of patients at the centre and therefore promote learning about the work of other health professionals in order to better integrate treatment activities.
Table 2 summarises the key activities uncovered in phase 1 and its implications for learning about lean.
Cognitive scaffolding.
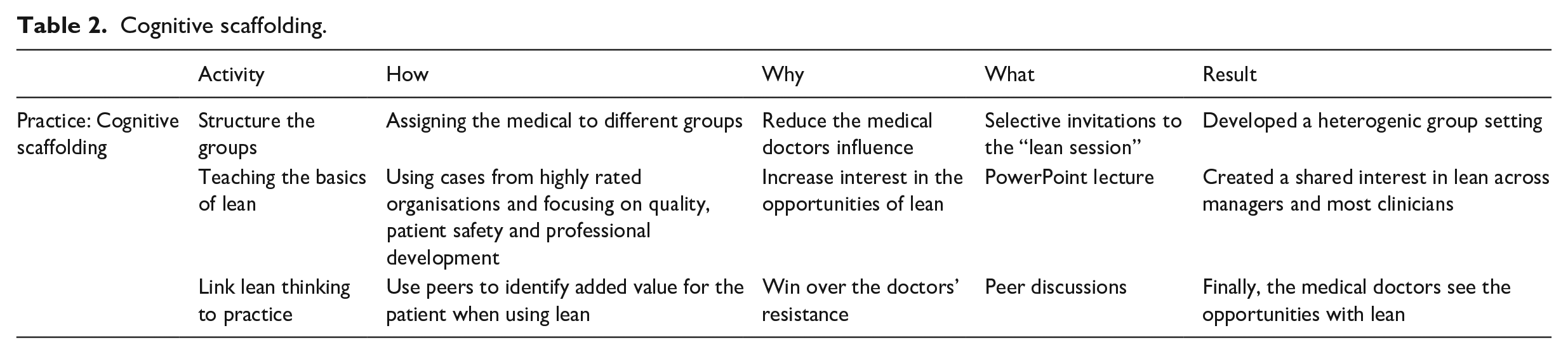
We have labelled the scaffolding in this phase cognitive scaffolding since HRD in this phase focused on creating a ‘cognitive space’ (Roberts and Beamish, 2017) and a lean mind-set. To create this ‘cognitive space’, HRD had to deal with the doctors’ resistance to facilitate the learning. Lean’s focus on reducing costs and efficiency created a tension that HRD had to reduce to make the clinicians willing to learn. Situated in this context, HRD was an active actor attempting to influence the micropolitics of scaffolding lean into clinical practices at the hospital. HRD had to develop a common knowledge interest among the clinicians in providing better treatment for the patient.
After phase 1, lean was no longer a remote management term but an idea that the clinicians could recognise and value, although it was still unfamiliar enough to represent a challenge for the clinicians, which stimulated further learning (Vygotsky, 1978). However, the clinicians were not ready to put lean into practice just yet, so HRD adopted peer-to-peer scaffolding, transferring lean through a bodily experience of lean. In phase 2, the clinicians had to ‘do lean’ through a collaborative task, building paper aeroplanes that take flight – first without lean, then using lean.
Phase 2: peer-to-peer scaffolding through ‘doing’ lean
The second scaffolding practice we identified in our material is ‘doing’ lean – an interactive learning process, namely building paper aeroplanes that can fly. Initially, the paper aeroplane activity was chosen due to its ability to illustrate the role of flow in effective processes. It was regarded as useful for hospital treatment that follows a step-by-step process, such as the treatment of thrombolysis and femoral neck fractures. This phase describes the time from the paper aeroplane activity in 2017 and follow-up meetings until 2019. In this category, HRD helped the clinicians to understand the relevance of lean in practice. This was conducted through the paper aeroplane activity, in which HRD acted as a coach who helped the participants see how lean could be utilised in a clinical practice.
Three separate paper aeroplane activities were held. Each meeting comprised 10–15 participants and lasted for around 60 minutes.
The first scaffolding activity in this practice was about convincing the doctors, this time to take part in the construction of paper aeroplanes. Our observations of the paper aeroplane activity (see Model 1) show that there was a great deal of scepticism among the doctors at the start: ‘Instead of operating today, should I be making paper aeroplanes? This is verging on the comical. I’m a doctor, not a kid at kindergarten’ (doctor). This quote, which is taken from our observation notes, shows the scepticism that HRD had to address even before ‘the activity’ had started. HRD addressed the scepticism in the group by explaining the purpose of ‘the activity’, and that the time would be an investment in the future. Here, it can be noted that HRD must justify why the clinicians should spend their time making paper aeroplanes instead of working.
At first, the chief medical officers sat with their arms crossed looking at me. I spent a lot of time explaining the purpose of the game [aeroplane activity], and when they uncrossed their arms and people started nodding, you realised it was not so stupid after all. I don’t think it’s about people being reluctant; it’s about the clinicians being busy, and that they are critical of the time you are taking when they could otherwise be with their patients. And I think that’s all right. My job was to convince them that the time they spent was an investment in the patient. (HRD manager)
The above quote states that HRD spent considerable time introducing ‘the activity’ to convince the participants that the time spent is an investment for themselves, their colleagues and, not least, their patients. HRD approached the sceptical doctors during the break between the lecture and the aeroplane activity. We also observed that HRD used examples from other hospitals that have succeeded with lean, in which HRD pointed out how all these hospitals had started with similar activities.
The second scaffolding activity is about setting up the paper aeroplane as an interactive learning process and creating a failure. The participants were divided into three groups comprising four to five participants in each group. They were then assigned different roles to play, before HRD explained the rules of the aeroplane activity. Through the document analysis of the rules, we note that the activity was set up in such a way that made it virtually impossible to achieve effective and quality results.
The third scaffolding activity was about creating a sense of success – building a high-quality paper aeroplane that could fly, but this time using lean methodology. By using lean, the participants were able to understand why they were unable to deliver the desired quality of the paper aeroplanes. We also noted that HRD coached the participants to ensure success. This had a substantial impact on the participants:
The paper aeroplane activity is nothing more than a way of introducing the lean mindset, to understand the culture and methodology The most important message of the game [paper aeroplane activity] is that it is the employees who have the best conditions for development and further growth. My role was to help the participants to make their own experiences, while I also had to help them understand how these experiences could be applied in practice. (HRD manager)
The above quote underlines that lean must be put into practice by the clinicians because they are the ones who can utilise it, not management or HRD:
This game [aeroplane activity] introduced us to lean methodology and demonstrated how lean contributes to the desired change. It was important to show the need for lean, and what lean could result in – to motivate the employees to use this method. That’s why [HR] had such an important part, as [HR] succeeded in arousing curiosity about lean methodology. (Medical Head of Unit)
The informants used words such as ‘contributor’, ‘guidance’, ‘introduced’ and ‘demonstrated’, which can be interpreted as an explanation of how HRD changed the participants’ orientation towards the practical implication of lean. The quote makes it clear that HRD demonstrates how lean methodology can be utilised, but also that the participants themselves must harvest the experience. In this way, HRD supports the group members in helping each other to see the relevance of lean knowledge. Through the aeroplane activity, participants accumulated their own experiences and knowledge about lean, and HRD challenged them to help each other find solutions. In this way, HRD helped the participants to discover how lean could be put into practice across distributed units. One informant stated,
The game [aeroplane activity] HR introduced was also important for creating a mutual understanding across the units. This mutual understanding was essential for the future, as it gave us an equal view of what could be improved (medical head of unit).
In the section above, it appears that HRD, with the help of the aeroplane activity, contributes to a ‘common understanding’ of the lean concept – which was also emphasised by several informants. We have also analysed the evaluation forms that the participants completed after the aeroplane activity. It appears that HRD helped to create a common idea, feeling and understanding of what lean could contribute to in the participants’ everyday work. This was described as an important milestone in the project as it represented a turning point for several of the sceptical participants, especially the doctors. Thus, HRD became an important player that managed to unite the distributed units to work towards a common goal. One informant elaborated:
The aeroplane activity is a simple ‘game’ that I thought was a waste of time. However, it still had a positive effect on me. I see that in retrospect. I must admit that. You learn that something works, with relatively basic tools. I was in a positive group. For me, that’s what rescued the situation. If everyone had been like me, the project would have come to a rapid halt. (Doctor)
Here, the informant shows that the aeroplane activity created motivation and commitment to join the project. The fact that the informant says that they ‘experienced that something works’ demonstrates that the aeroplane activity contributed something more than just knowledge about lean, namely a sense of what lean can contribute to. Here, we see that the aeroplane activity affects the individual’s senses and emotions associated with lean which, in turn, helps to influence their learning capacity because they become more receptive to impulses, information and knowledge. Even though the paper aeroplane activity may be perceived as ‘simple’, it still had an important impact on the participants’ perception of lean.
The fourth scaffolding activity in this practice was about facilitating discussions regarding how lean ideas can be put into practice in the hospital. Meetings were organised from 2017 to 2019. Here, HRD helped to create positive discussions so that they could link the lean knowledge they acquired to their clinical context. An informant elaborated:
Challenging the employees with the idea that it is them who hold the answers and showing a certain humility that they do not necessarily have insight into everything that moves – I think that is an important quality that HR managed to master. There were useful discussions that transformed the game [aeroplane activity] from a game into something more concrete and serious. (Divisional advisor)
Table 3 summarises the key activities uncovered in phase 2:
Peer-to-peer scaffolding.
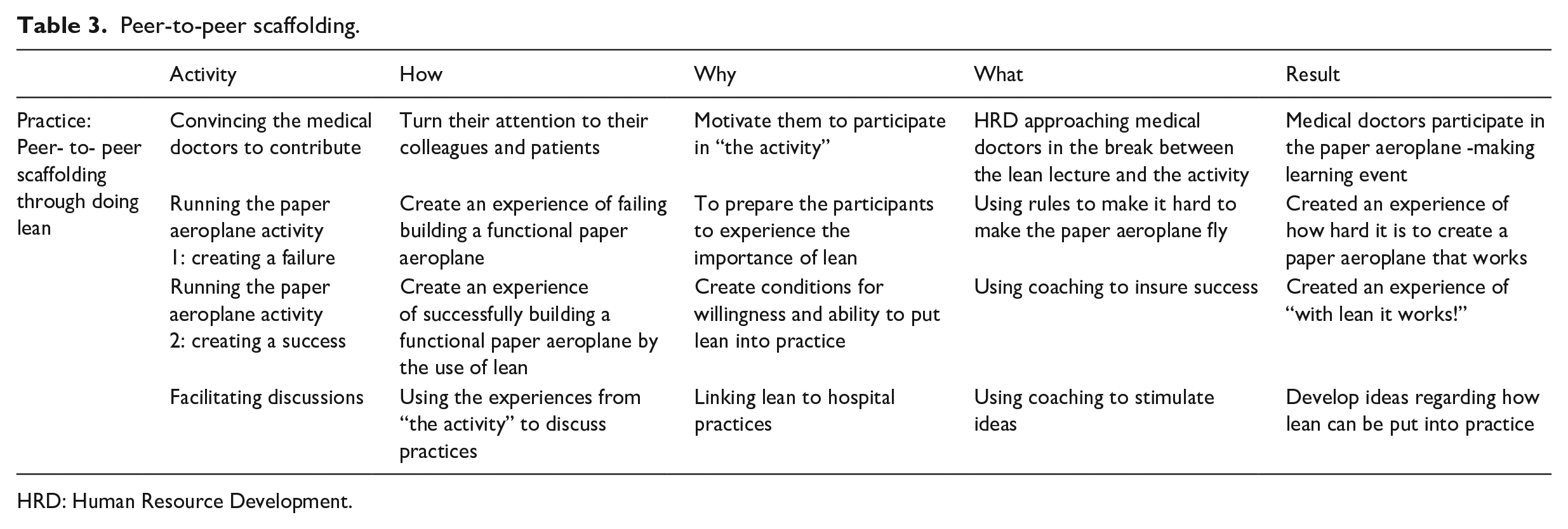
HRD: Human Resource Development.
We have labelled the scaffolding in this phase peer-to-peer scaffolding since HRD in this phase focuses on peer interactions during the paper aeroplane activity and when discussing lean ideas to innovate hospital practices. Phase 2 can be characterised as a strongly HRD-controlled learning process for the clinicians, in which HRD pre-planned a failure and a success in order to promote learning. By using the aeroplane activity, HRD was able to progressively frame lean closer to the clinicians by teaching lean (phase 1) and through creating a mutual experience of lean (phase 2). The role of this ‘inflicted’ shared experience and, in particular, embodied knowledge in relation to peer learning, will be discussed in the discussion section of this paper.
Phase 3: fading of the scaffolding: lean turned from something HRD knows to something the hospital units know
Phase 2 revealed the importance of having a mutual experience in the paper aeroplane activity, in which HRD offered coaching and supported peer-to-peer scaffolding among the clinicians who linked lean with clinical practices. In phase 3 (2019–2020) of the project, HRD challenged the hospital units to own the process itself, where HRD was in the background and answered the questions from the hospital units. In the first activity of this phase we observed the value stream analysis of the treatment of stroke patients. The participants were the same groups that participated in the aeroplane activity. Each group had to perform the same value stream analysis before everyone gathered to compare the results. By mapping all the stages the patient had to go through before receiving treatment, they found that if ambulance personnel transported the patient directly to the MRI examination room, this would reduce the waiting time by 15–20 minutes. They also found several time ‘thieves’ when all the results were compared, and together they managed to reduce the waiting time for thrombolysis treatment, which saved the lives of several patients. Following this, it was decided that the results from the value stream analysis would be implemented in practice. This was an extensive and time-consuming process, insofar as many of the clinicians had to change their daily work procedures. Despite this complexity, HRD believed that their most important contribution was to hand over responsibility to the hospital units. The HRD manager elaborates on this:
It’s not difficult to create change. What’s difficult is maintaining change. If I’d assisted in the same way in this phase, participants would not have gained the necessary experience that the medical units needed to maintain the changes. Thus, it’s important that the hospital units have ownership from the start, and the best way to get ownership is simply to work with it (HRD manager).
The above quote shows the importance of giving temporary and calibrated support, in which HRD must challenge the hospital units to take ownership of the process. No one talks about the scaffolding when the cathedral is completed, and the same applies to this situation. If it had been HRD who went on stage to receive ‘this year’s lean award’, they would not have done their job as a scaffold. Thus, it was important to withdraw from managing the process, so that the hospital units gained the necessary experience to ride out the storms that are guaranteed to appear after the innovation process. This temporary support can be regarded as the second activity in this phase, which also became a focus for the hospital units, albeit with a different view:
HR is important, but I felt we were left alone, yet we managed to complete the process. I experienced that HR failed to intrigue us. HR supported us, but not as much as we wanted. It would have been good if HR had been more involved in the processes. We were a department that saw opportunities and not limitations, and we were positive. But imagine what we would have achieved if HR had assisted – not just stood on the sidelines and cheered on us. HR were good at cheering us on, but I feel they withdrew a bit too soon (head of medical department).
An important aspect of the above quote is that HRD played an important role at the start of the lean project. As the staff gained enough insights about lean, HRD withdrew. Thus, the informants did not credit HRD for the success they achieved, since the clinicians and their managers did most of the hard work of changing practices using lean.
HRD was criticised for withdrawing too soon, which indicates that HRD did not manage to effectively master the fading process. This different perception of the role of HRD emerges in these two quotes:
The job began and HR was gone. There are probably other actors besides HR that should be credited for the success of this project. HR knew what they were doing; we did not. So why they left us so early in the process, I’ll never know. We did well, although much of the lean thinking stopped with us. HR could have helped us to spread the ‘good news’ – so to speak. (Doctor)
Why HRD withdrew early is explained here:
HR is not supposed to own the process. HR is a support and guide in the process, and if we start to pull all the load then we have done the hospital units a disservice. HR must withdraw to strengthen the hospital units’ position and competence, and if HR was supposed to be responsible for driving the entire process, we would not build a solid foundation, but a house of cards (HR director).
The above quotes show that the hospital units had a different view of how HRD should assist in the learning process. This tension becomes even clearer when HRD fails to create a seamless transition from being the actor responsible for the driving process to becoming an actor who ‘cheers’ from the sidelines. HRD may have failed to clarify its expectations with the units, but it succeeded in its role as scaffolder by supporting, motivating and guiding the process of implementing lean methodology in some hospital departments. In a hospital that is located in many different areas, HRD, with its centralised position, could contribute to sharing lean knowledge further in the organisation. Perhaps HRD could have been faded out more gradually, so that the lean methodology gained a foothold in several parts of the hospital. Nevertheless, all in all, the project has been a success that saved many lives, and HRD has been an important temporary support during the process. This hospital won the lean award in 2016 for the same-day surgery project that involved several hundred employees. However, as the findings suggest, it is difficult to involve other units in the hospital with lean. Also, the perception of who is familiar with lean in the organisation has changed. Currently, the hospital units think that lean is something HRD knows, whereas HRD thinks lean is something the hospital units that participated in the lean project know. The implications of this dilemma of HRD fading its scaffolding for organisational learning will be discussed in the discussion section of this paper.
Table 4 summarises the key activities uncovered in phase.
Fading of the scaffolding.
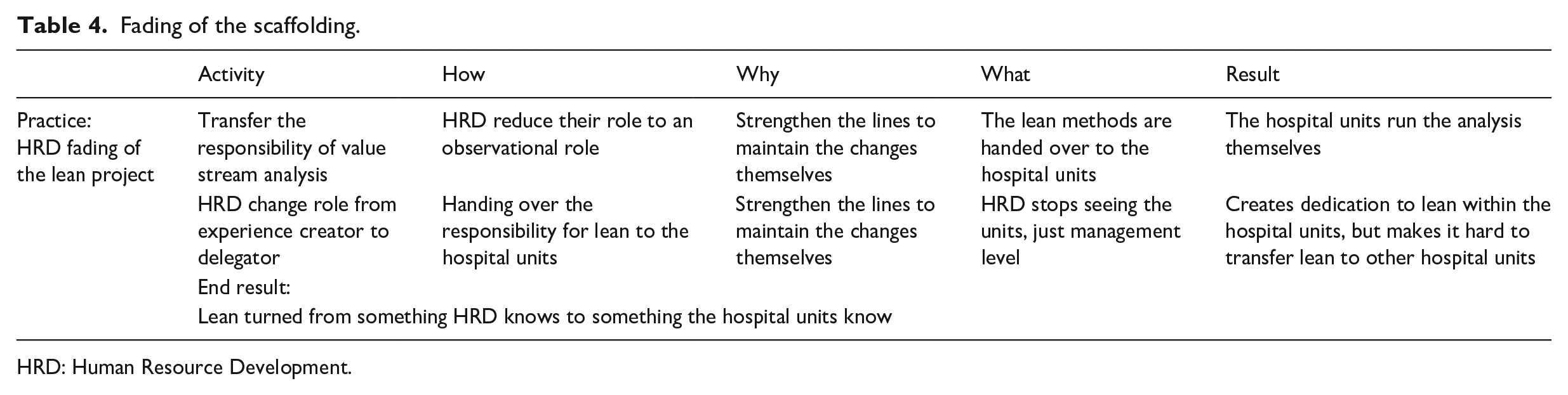
HRD: Human Resource Development.
Discussion
What can the three identified HRD practices tell us about learning in organisations? In the following, we will discuss this in order to answer our research question. Our research question asks ‘what’ is the role of HRD in the lean learning process of hospital clinicians?
Phase 1: cognitive scaffolding – creating a lean mindset
We called phase 1 cognitive scaffolding. Cognitive scaffolding takes place when the learners’ perception of their work or practices is changed by enactive representation (Bruner, 1990; Elkjaer and Brandi, 2014; Roberts and Beamish, 2017), changes which are meaningful and developed in interaction with others. The HRD practice in phase 1 involves teaching activities containing the new perspective, lean, its terminology and ‘system thinking’, accompanied by examples of real-world applications that make lean more understandable. We find that HRD is able to frame lean close enough to the clinicians, which makes them interested and motivated to learn more in relation to their clinical practices.
However, there is more going on. Our study highlights a tension between organisational learning and professional learning in which doctors do not see the need to engage themselves in this ‘lean double-loop learning process’. In relation to this tension, phase 1 reveals the skilful work of HRD in re-structuring the power factors of learning.
A ‘cognitive space’ (Roberts and Beamish, 2017) is achieved by HRD using several tactics: First, by ensuring that only a few doctors are present at each meeting; second, by sensing who is opposed to lean by noticing who has made critical comments and by interpreting the body language of the participants, and then informally trying to convince them; and third, by making use of other clinicians to convince the sceptics. In doing so, HRD brings in existing knowledge and experience that motivate the clinicians to learn (Knowles et al., 2014). To some extent, we can also argue that HRD makes use of other clinicians to compensate for HRD’s lack of professional legitimacy (Trullen and Valverde, 2017). However, we also uncovered a shared interest in lean and an ‘alliance’ across HRD, managers and nurses as opposed to the more sceptical doctors, who were initially less willing to change their practices.
From this cognitive scaffolding activity, we see that HRD acts as a ‘mindsetter’ that aims to motivate the learning of lean in relation to the clinicians’ practices.
Phase 2: peer-to-peer scaffolding through ‘doing’ lean
The second phase reveals another scaffolding practice in ‘doing’ lean – an interactive learning process among peers, building paper aeroplanes that take flight. This phase we have labelled peer-to-peer scaffolding since HRD in this phase focuses on peer interactions during the process of building paper aeroplanes and when discussing lean ideas to innovate hospital practices. Phase 2 can be characterised by hard scaffolding (Brush and Saye, 2002) in which HRD controls the learning process for the clinicians and has pre-planned failure and success to promote learning.
In our view, the paper aeroplane activity is fundamental to this adult learning process since it generates interest, excitement and in-depth learning by using a planned failure followed by a planned success. The collective experience creates intersubjectivity (Vygotsky, 1978), that is, a common ground for further learning. This is achieved through the use of bodily senses, material (paper) and targeted coaching by HRD. This guided discovery process (Vygotsky, 1978) helped the clinicians to develop a practical understanding of lean in their own practices (Gherardi, 2017; Mazur et al., 2019). Here, by doing lean together during the paper aeroplane activity with peers and then discussing lean in relation to work activities, we find that the paper aeroplane activity creates a shared experience that is valuable for developing new practices. As well as showing how lean can be put into practice, this paper suggests other more fine-grained contributions to the literature on organisational learning. Our research case reveals how HRD as a temporary support can play an important role in assisting managers and employees in recognising and linking external and internal knowledge. Currie and Kerrin (2003) and Stanton et al. (2014) also underline the importance of HRD in the learning process, and how HRD can help an organisation overcome the influence of sceptics and non-believers. This is particularly relevant in the health sector in which the various professions protect their subject areas (Dewan and Norcini, 2019; Hamlin, 2002), making them sceptical of the changes caused by lean (Andersen and Røvik, 2015; Mazur et al., 2015). Although these studies demonstrate the potential benefits of knowledge engagement, they fall short of showing how HRD can encourage knowledge engagement between peers. Thus, this study’s contribution is that it specifically describes how an organisation can firmly create knowledge engagement between peers.
Like Knowles et al. (2014) argue, we find that HRD can play an important role in adult learning processes by motivating the learners to shape their own learning. Our insights from phase 2 clarify how HRD uses peer-to-peer scaffolding that creates conditions for the willingness and ability to put lean into practice. Specifically, we show how HRD uses the paper aeroplane activity as a positive moderator in the relationship between different professions to create a mutual interest and promote knowledge sharing. In turn, this is crucial to change practice (Corradi et al., 2010; Hawkins et al., 2017 Lins et al., 2021).
From this scaffolding activity, HRD performs the role of an ‘experience creator’ who creates knowledge engagement between peers – to put lean into practice.
Phase 3: fading of the scaffold. Lean turned from something HRD knows to something the hospital units know
Since we find that ‘lean is something that the hospital units know’, it would appear that this group of multi-professional clinicians has successfully controlled their own learning (Bruner, 1990), and therefore we could say that HRD has accomplished the tasks of phases 1 and 2.
However, the fading has not been sufficiently adapted to the individual learner (Noroozi et al., 2018). From the perspective of a learning trajectory (Elkjaer and Brandi, 2014; Tawfik et al., 2018), this means that the individual learner does not acquire the necessary support to interact with those in other collaborating hospital units to promote lean thinking in the intersection of their practices. While official initiatives can be good vehicles for developing structures within and across communities, which can improve organisational learning (Pyrko et al., 2019), it seems in this case that new structures only develop when all the learners have been subject to the same HRD scaffold process. Then the organisation will have two versions of lean – HRD’s version and the clinicians’ version – who have gone through the lean process, creating a learning tension regarding which version should be the starting point for other units to be included in a two-step learning process.
Although this fading reduced the spread of lean thinking in the hospital, the fading and experience of failure contributed to increased learning among the clinicians. Noroozi et al. (2018), on the other hand, emphasise that failure can have a positive effect on the learner, because failure can contribute to showing the importance of some knowledge. From the perspective of adult learning theory (Knowles et al., 2014), the failure helps the clinicians to see the relevance of lean–and their motivation for applying the principles in their own practices grows.
Organisational learning theories have long emphasised the importance of knowledge sharing across professions and cultures (Corradi et al., 2010; Filstad, 2010; Kauppila et al., 2011). We argue that a focus on fading provides a new perspective on organisational learning, and a dilemma, in which our findings provide a two-part answer. By fading out, HRD succeeded in handing over responsibility to the clinicians which, in turn, contributed to the identification of successful innovative solutions. Nevertheless, it was not possible to spread the lean knowledge further in the organisation. This can be explained by a lack of support from HRD, but also because health clinicians’ returned to their uni-professional learning activities (Molloy et al., 2014).
In the scaffold activity of fading, HRD performs the role of a ‘delegator’ who transfers the responsibility and control over the learning to the clinicians in order to increase learning among the clinicians.
Conclusion
Our research question was as follows: What is the role of HRD in the lean learning process of hospital clinicians? Based on our findings, HRD make use of cognitive, peer-to-peer scaffolding and fading to promote learning. We have identified three types of roles that HRD plays.
First, through the activities of cognitive scaffolding, HRD assumes the role of a ‘mindsetter’. In this role, HRD influences power relations to promote knowledge negotiations (Mørk et al., 2010) by approaching one doctor at a time and by convincingly proving the usefulness of lean through the paper aeroplane activity. This study also has a broader relevance for how problematic relations for learning can be reduced in a context with autonomous professionals. While previous research underlines that a specific group may take control of a multidisciplinary group and prioritise its knowledge (Mäkinen, 2022), this research highlights how HRD is able to create a shared purpose by teaching lean thinking, create shared experiences of the usefulness of lean, and include the voices of several professions. When HRD has established the purpose for learning among the participants, the participants gradually take control of their learning, as recommended in adult learning theories (Knowles et al., 2014).
Second, through peer-to-peer scaffolding, HRD are ‘experience creators’ who promote new shared experiences among learners through the paper aeroplane activity. HRD additionally use existing knowledge, experience, and motivation of learners to form the learning experience as recommended in adult learning theory (Knowles et al., 2014). In this way, the learners overcome and make use of the tensions between professional learning and organisational learning (Elkjaer and Brandi, 2014).
Third, through the scaffold activity of fading, HRD are ‘delegators’ who leave the process of further learning to the participants – which increase the learning among the clinicians. However, since the HRD role is limited in time and space, the clinicians’ return to their uni-professional learning activities – and the lean project – ends.
We also contribute to the role of emotions in organisational learning (Filstad, 2010; Gherardi, 2017) where, in this case, emotional scaffolding fuses knowledge engagement for lean and, in turn, the lack of emotional scaffolding harms it. By examining the implications of a lean implementation process, we have gained insights into how fragmented organisational learning can be. This fragmented learning creates a tension that can trigger further learning (Elkjaer and Huysman, 2008). However, in this particular research case it would appear that it makes it difficult to move forward in the learning process.
The findings and implications of this paper also need to be reflected in light of its limitations. We would therefore like to highlight the weakness of not retrieving the data from the same period. We carried out the observations before we conducted the interviews. In this context, the time frame (six months) should have been less. This is because the informants may have forgotten and/or added facts about the lean process, which confuses the empirical basis. Finally, we have identified a potential research area for further development of this study. It would be desirable to analyse the ways in which HRD can operate in and make use of the different versions of ‘lean’ as a trigger (Elkjaer and Huysman, 2008) for further learning and link this to other variables such as organisational strategy, change and innovation processes.