
Abstract
Hemostasis in nail surgery requires its own specific set of skills due to the small size and unique anatomy of the nail unit. This structured review uses the most up-to-date evidence to outline the current tools and techniques to manage bleeding before, during, and after surgery in this special group of patients.
Introduction
Bleeding is a reality of surgery that requires skill to manage. Nail surgery is unique in that neither ligation of vessels nor electrical hemostasis is used given the small and delicate nature of the nail apparatus. The nail unit has a rich vascular supply with extensive anastomoses so excessive perioperative bleeding can contribute to psychological distress 1 both for the surgeon and patient, failure of the procedure due to poor visualization of small anatomic nail structures, traumatic dressing removal, and infection. We searched the English and French language literature from 2004 using the Ovid Medline and Embase databases. Our strategy included the keywords “fingernail,” “toenail,” “hemostasis,” “blood loss, surgical,” and “nail surgery,” which yielded 69 articles of which we kept 33. Articles were rejected if they referred to the use of nails as fixation devices in orthopedic surgery, discussed traumatic finger injury, or if they were articles that involved basic science or animal research. The retained articles as well as information from three reference texts2 -4 were reviewed to extract key evidence-based principles to manage bleeding before, during, and after nail surgery.
Before Surgery
Assessment of the potential for excess bleeding begins pre-operatively. Two important questions guide further care:
“Do you have a bruising or bleeding problem?”
“Do you take any medications, supplements, or natural products?”
If patients report a bruising or bleeding problem, they are best co-managed with hematologists, especially when larger nail surgeries are planned. These patients may have conditions such as hemophilia or von Willebrand disease, which significantly increase the risk of perioperative bleeding.
If patients take medications such as anticoagulants or antiplatelet agents, management should follow those of dermatologic surgery, 5 as there are currently no nail surgery-specific guidelines. Supplements/natural products, such as Ginkgo biloba, vitamin E, and ginger, may increase bleeding risk.5 -8 Because patients usually don’t consider these to be medication, careful questioning is a must prior to the procedure.
During Surgery
Injecting a commercially manufactured local anesthetic that contains epinephrine induces hemostasis chemically. Despite a deeply ingrained belief to the contrary, this practice is safe in nail surgery and has over 50 years of experience as well as a vast evidence base9 -11 to support it. Indeed, as Jellinek argued over 10 years ago, the traditional dogma of epinephrine contraindication in digital surgery should be relegated to the past. 12 That being said, there are some reports of digital ischemia in patients with Raynaud’s13,14 who received epinephrine-containing local anesthetics. It may be prudent to avoid this combination in patients with Raynaud’s and others with significant peripheral vascular disease. 13
Tranexamic acid (TXA) has been increasingly reported to be safe and effective in dermatologic surgery.9,15 Lidocaine 2% and TXA 100 mg/mL mixed in a 1:1 ratio reduced bleeding during Mohs micrographic surgery, especially in those patients on anticoagulants. 16 This deserves further study, specifically with larger nail surgeries.
A tourniquet is by far more effective than epinephrine in creating a bloodless field. This is especially valuable in order to visualize important anatomic landmarks in the small nail apparatus and for nail procedures that require a completely bloodless field, such as chemical matricectomy with phenol for onychocryptosis. The reason for this is that phenol acts by coagulating tissue proteins. If blood is present, the procedure will fail because phenol will destroy blood proteins and not those of the matrix. 17 Tourniquets mechanically compress the digital arteries. Since these arteries are paired and run on either side of the digit, a tourniquet may theoretically be placed at any position proximal to the surgical field; in practice, most apply it to the base of the digit. Advantages include the surgeon’s ability to directly control when hemostasis starts and stops. Reperfusion after the procedure should always be visualized, eliminating the concern of prolonged ischemia. 12 Various tourniquets can be employed. A simple Penrose drain secured with a hemostat is a commonly used option. 18 Another is a sterile glove with the fingertip pierced, as described by Salem. 19 When the glove is rolled back, it not only acts as a tourniquet but also causes a degree of exsanguination. Disadvantages of tourniquets include pressure injury to the digital vessels. It seems that pressure-induced shearing forces on vessels may be more of a determinant of ischemic injury than the duration the tourniquet is applied.12,20 This means it is important to use the minimum tourniquet pressure to achieve hemostasis. The evidence does not provide a maximum time that a tourniquet may be applied safely. Since upper limb surgeries with tourniquet times of 2 hours don’t result in ischemic finger injury, 20 it may be reasonable to use this as an upper limit until further data can guide us. Another disadvantage of a tourniquet is the potential for digital ischemia/gangrene if the tourniquet is not removed after surgery. An excellent habit is to mandate that the surgeon who places the tourniquet be the one to remove it, without exception. Some commercially available tourniquets include T-Ring™ (Precision Medical Devices LLC, San Clemente, CA, USA) and Tournicot™ (Orthotic-Lab Limited, Middlesex, UK). These devices have the advantage of enabling hemostasis without exceeding the pressure that has been demonstrated to cause nerve injury, regardless of digit circumference. 21 Studies that compare tourniquets highlight differences in cost, ease of use, and potential for pressure injury due to the device itself or if accidentally left in place.20 -24
After Surgery
Blood flow is re-established following tourniquet removal. In the case of chemical cautery, this is reassuring as it signals the neutralization of excess phenol. In other surgeries, bleeding might be a source of stress for the surgeon as it may be significant in larger surgeries, such as total nail unit removal. Easy techniques to control excessive bleeding that all nail surgeons should know involve the use of topical hemostatic agents and mechanical maneuvers.
Topical hemostatic agents are excellent options for light bleeding such as that following plate avulsion without replacement or shave biopsy of the bed. Aluminum chloride rubbed vigorously with a cotton-tipped applicator works well. Another option is Monsel’s solution (ferric subsulfate), though iron deposits risk staining. Monsel’s may also cause melanocyte activation 25 which can interfere with the management of patients with longitudinal melanonychia. More recently reported options include topical vasoconstricting agents, such as oxymetazoline (Afrin®), which have helped manage bleeding in sinus surgery.9,26,27 This can be sprayed onto gauze and applied to the nailbed with pressure. Another option is brimonidine in a 0.33% gel (Mirvaso®; Galderma Laboratories; L. P., Fort Worth, TX, USA) as published by Lipner. 28 In this case series, hemostasis was achieved in under 2 minutes, and 40% of patients were even taking aspirin at the time of surgery. 28 Because of its capacity for vasoconstriction and ability to penetrate the blood–brain barrier, this option is best deferred in patients with cardiac and neurologic conditions as well as in infants.9,26 -28 Kaolin is an aluminum-based inorganic product that activates the coagulation cascade. When applied to the nail unit with firm pressure, kaolin-impregnated gauze has been found to be safe and effective. 29 Similarly, calcium alginate (Kaltostat®) is a non-resorbable dressing that can accelerate hemostasis when applied to the wound. 30 Lastly, oxidized regenerated cellulose, such as Surgicel™ (Ethicon, a subsidiary of Johnson & Johnson) is a resorbable sterile fabric mesh that acts as a scaffold for thrombus formation and concentrates hemostatic factors. 31 This fabric is particularly useful after removal of a lesion leaving a cavity that may fill up with blood or serum, as with surgery for glomus tumor or exostosis (Figure 1).

Defect post-extirpation of a glomus tumor filled with Surgicel™.
Mechanical maneuvers include simple pressure—this often-underappreciated technique is effective and available. Up to several minutes of uninterrupted pressure is often all that is needed. 25 For larger procedures, such as removal of the entire nail unit, as for melanoma-in-situ or keratinocyte carcinoma, traditional sutures may be the best option for hemostasis. A running locked suture (Figure 2) will decrease post-operative bleeding significantly. 32 A final, seemingly magical, approach is the volumetric tourniquet. A 0.5 mL bolus of fluid may be injected to each lateral aspect of the digit, causing mechanical compression of the digital arteries (Figure 3). This fluid may be saline but the surgeon may consider using a longer-acting local anesthetic, such as bupivacaine or ropivacaine, making the post-operative course even less painful. 33

A running locked suture, with big bites all around the defect, following total nail unit excision for melanoma-in-situ.
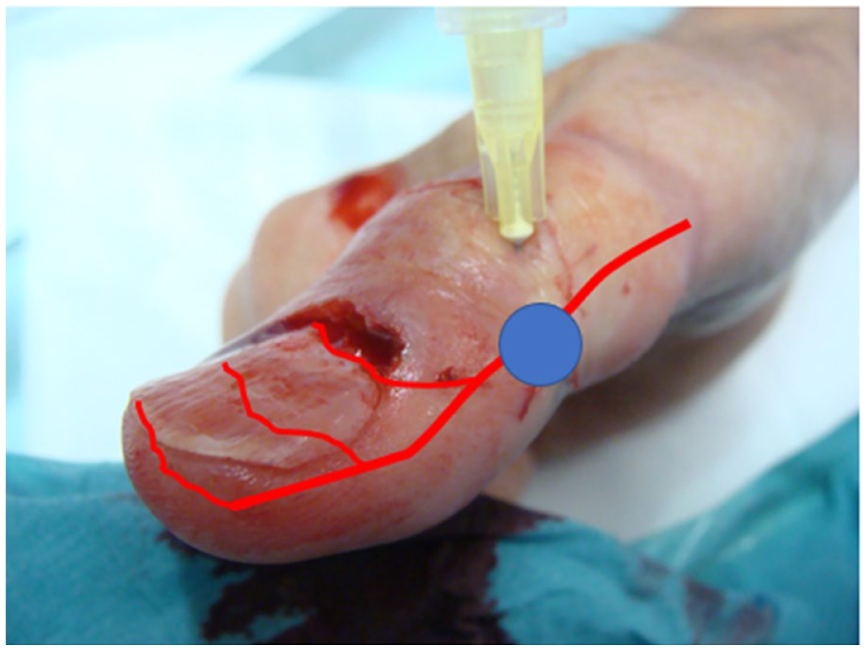
Use of a volumetric tourniquet for hemostasis. A small bolus injection of saline or a long-acting anesthetic (illustrated by the blue dot) compresses one of the paired digital arteries (illustrated in red) at the lateral aspect of the digit.
Various dressings have been used for hemostasis and simultaneously offer wound protection. Because there will be some bleeding after nail surgery, even with the above-mentioned techniques, applying a non-adherent, greasy dressing will ensure that removal is a non-traumatic experience (Figure 4a). Following this, a bulky dressing is applied to ensure light pressure for hemostasis, absorption, and protection (Figure 4b). A common example is a gauze wrap, such as Kerlix™ (Cardinal Health). Caution is advised when using dressings with more elastic fabric, such as cohesive tape (Life Brand™; Loblaw Companies Limited) or Coban™ (Solventum (formerly 3M Health Care), St. Paul, MN, USA). Post-operative bleeding and swelling may induce pressure injury (Figure 5). Worse, digital necrosis resulting in amputation has been reported. 34 If these fabrics are used, it would be safest to allow the roll to unwind first and apply without stretching. 34 If there is extensive bleeding, the dressing should be removed to identify the source. Re-injecting a small fluid bolus on the lateral aspects of the digit, as mentioned above, usually solves the problem. If bleeding persists, a compressive dressing may be applied while the patient waits in the room for an additional 15 to 20 minutes. When this is successful, the dressing should be replaced with one that has minimal pressure.
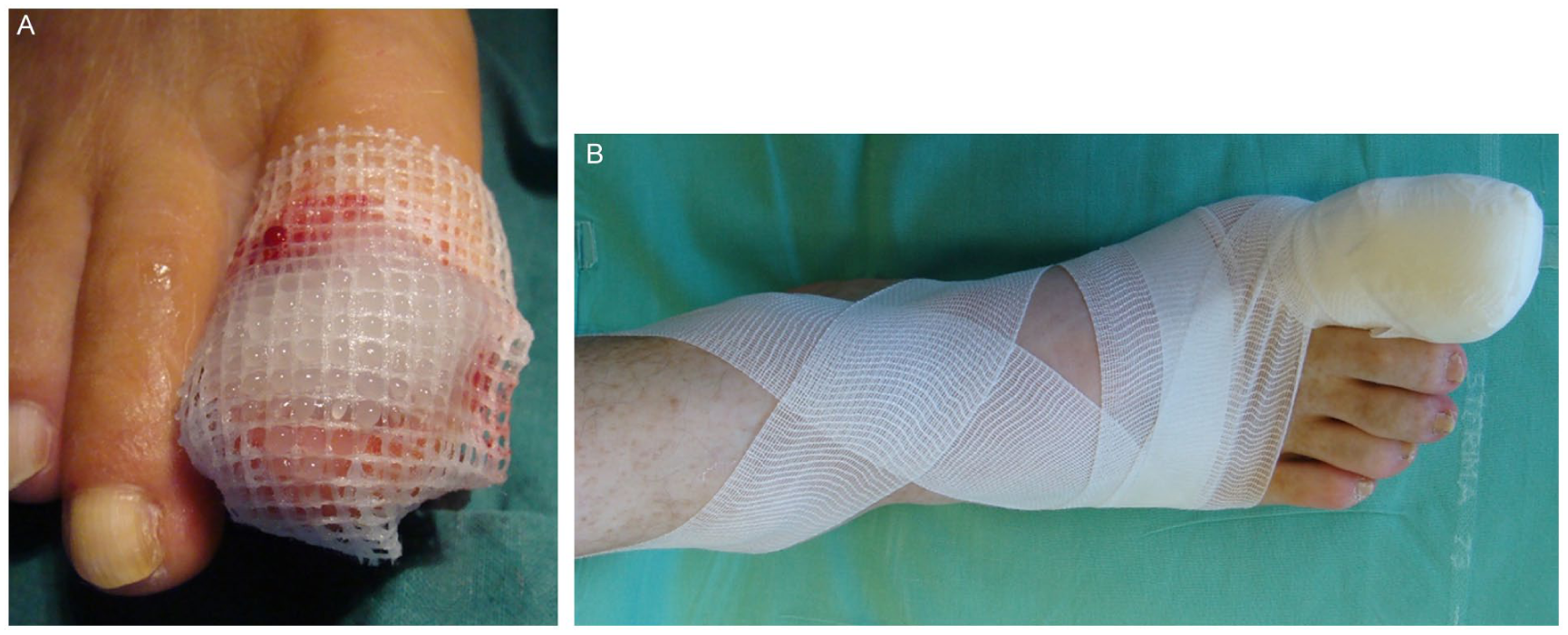
(a) A greasy dressing protects the wound and ensures non-traumatic removal. (b) A bulky dressing protects the wound and helps with hemostasis.

(a) Pressure injury after the use of cohesive tape following glomus extirpation. (b) Pressure injury after use of cohesive tape following excision of longitudinal melanonychia.
Limb elevation above the level of the heart for 48 hours is a simple and very effective technique to control bleeding. It has the added benefit of decreasing post-operative pain. Lastly, surgeon follow-up at 48 hours post-procedure is a sound practice to help assess and limit bleeding-related complications.
Conclusion
Effective management of peri-operative bleeding is an essential skill of the nail surgeon. A concise pre-operative assessment is mandatory to avoid unexpected bleeding. Epinephrine-containing anesthetic, even if safe, is much less likely to offer a bloodless field than a tourniquet. For post-operative bleeding, pressure and the lateral injection of a small fluid bolus (saline or a long-acting anesthetic), are the best options.
Footnotes
Acknowledgements
The authors wish to thank Noa Vigny Billick for technical editing.
Author Contributions
Drs Kendall Billick and Bertrand Richert contributed equally to this manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
Not applicable.
Consent to Participate
Not applicable.
Consent for Publication
Informed consent for publication of images in the figures was provided by the participants.