
Abstract
Stop the Bleed™, the education program created by the American College of Surgeons to address life-threatening bleeding, came from concepts of combat casualty care in tactical settings in the US military. Tourniquet control of exsanguinating extremity injuries dates from its first recorded use in the French military in the 17th century and its general issue to ships of the Royal Navy during the Napoleonic Wars. Wound packing and pressure dressings, specifically in junctional sites and head and neck, also date from the 16th century, illustrating the priority of hemorrhage control throughout the history of military medicine.
Tourniquets
The 3 main skills of Stop the Bleed™ are direct pressure, wound packing, and the use of a tourniquet. Directed at immediate responders to a scene of injury, the course also teaches lay bystanders how to recognize and control dangerous bleeding in injured patients. 1
Tourniquets were used for amputations in the 16th century by such surgeons as Hans von Gersdoff, Guy de Chauliac, Ambrose Paré, and Wilhelm Fabry. The first documented military use was a windlass tourniquet created in 1674 by Etienne Morel, a French military surgeon, who used a stick to twist a bandage until bleeding stopped from a thigh wound. 2
In 1718, Jean-Louis Petit reported his invention of a device that used a twist screw to force a leather pad onto major vessels, avoiding the painful abrasion of the skin and soft tissues from constricting the entire circumference of the limb (Figure 1).
3
The design was favored by surgeons of the Royal Navy. Six Petit tourniquets and 20 yards of cloth tape were among the contents of standard instrument chests provided to the ships’ surgeons during the Napoleonic Wars (1793-1815).
4
Petit tourniquet, from his original communication (Ref. #4). Public domain.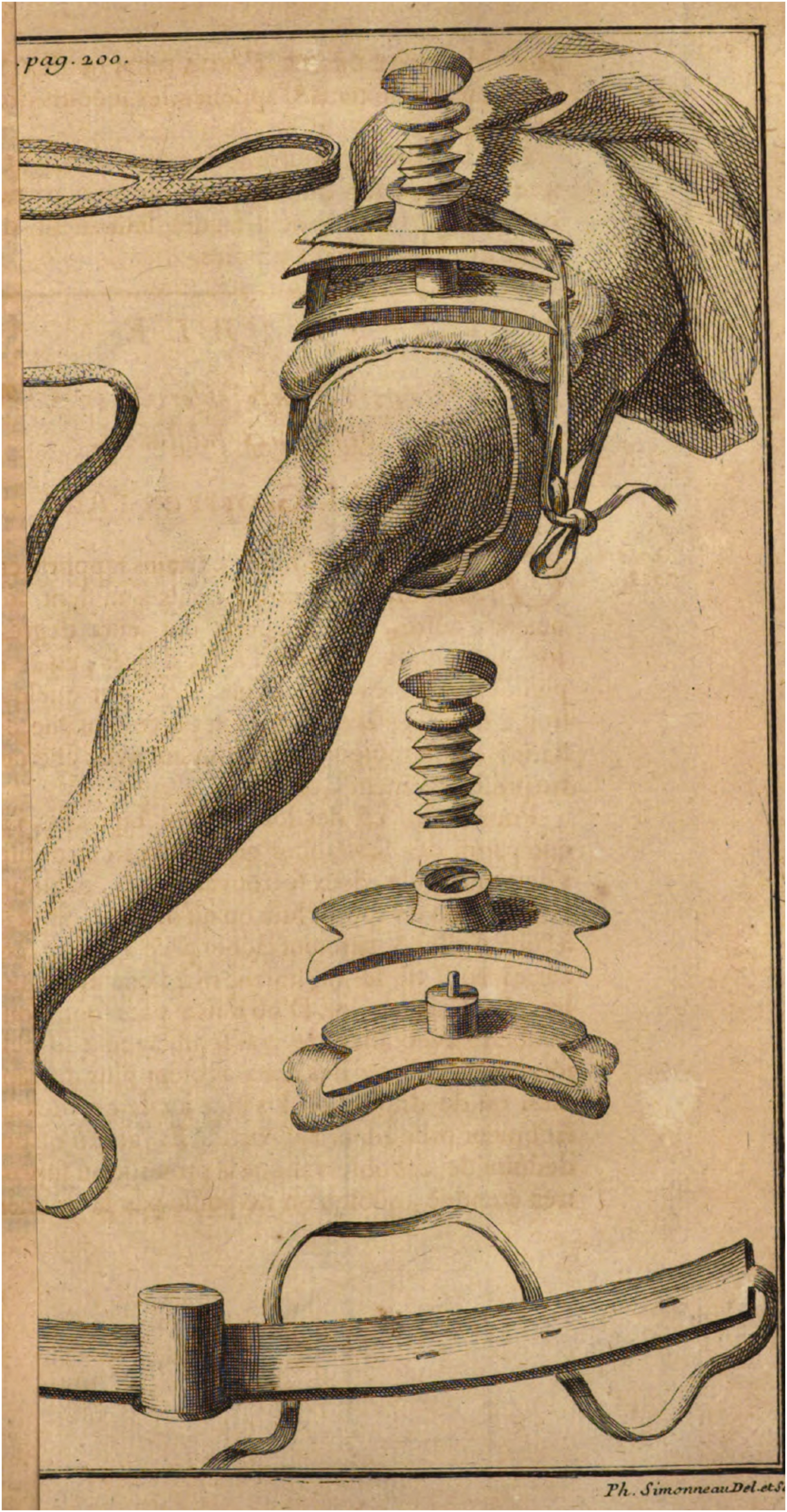
Stop the Bleed™ on Deck
The current foundations of Stop the Bleed™ came from a 1993 directive from the Commander of the Naval Special Warfare Command to study combat casualty care in a tactical setting. While there may be one or two corpsmen or medics assigned to a special operations force, they may be themselves incapacitated. Care at its earliest stages then must be delivered by non-medical patrol personnel. 5
There were no knowledgeable corpsmen or medics during the Napoleonic Wars. Surgeons attended the wounded below deck in the relative safety of the rear of the orlop known as the cockpit. Whoever was nearby and could be spared from direct action took an injured mate below, a task that was arduous and dangerous. Fully exposed to enemy fire, the victims were dragged through the wreckage on deck and lifted down the hatch, an especially hazardous task when the steps were destroyed. Left undressed, without immobilization, fresh injuries continued to bleed. 6
The danger was recognized by Gilbert Blane (1749-1834) in his first year in service to the Royal Navy in the Windward Islands. 7 In 1782, as a medical doctor without experience in surgery and not needed treating the wounded casualties, he was on the quarterdeck as an observer during action off Martinique.
He had the foresight to have some tourniquets with him in case they were needed. The occasion did not arise, but the mayhem he witnessed convinced him of the benefit of tourniquets and the readiness to apply them. Would it not be advisable at all times that some intelligent person, a warrant or petty officer, quartered on the quarter-deck, should carry in his pocket some [tourniquets], particularly in large ships, on account of the distance of the cockpit? He need not be a medical officer; and the only instruction necessary would be to point out to him the situation of the great artery in the thigh and arm: or with this information alone, the blood might be stopped by a handkerchief tied tight.
7
The commonsense wisdom of such a policy was verified in 1797 when Lord Nelson’s right elbow was shattered with grapeshot as he led the attack on Tenerife in the Canary Islands. His stepson, Josiah Nesbit, quickly fashioned a tourniquet from a handkerchief and saved Nelson’s life. 8
Blane never served as a ship’s surgeon, despite his service as commissioner on the Sick and Hurt Board (1795-1802) that oversaw the health of seamen. 6 He was credited for significant medical reforms, including the general issue of lemon juice to fight scurvy, nearly a half-century after James Lind’s discovery was published in 1753. His recommendations on tourniquets, however, were not implemented during his term on the board. 6
William Turnbull was an experienced naval surgeon who wrote an authoritative book on practice at sea, published in 1806.
9
He seconded Blane’s idea on tourniquets and had them distributed to His Majesty’s warships. As loss of blood is the principal cause of the number of deaths which take place at sea during an engagement, every ship should be provided with a certain number of tourniquets of the simplest construction, for ready and immediate application. To save the lives of wounded as much as possible is also a proper step that the crew themselves should be taught the use of this instrument.… This plan I communicated to the late Mr. Bird, then Surgeon to the Arrogant, and afterwards surgeon to Lord Hood; and the practice in consequence became general through the fleet.
9
Dossils of Lint
For junctional hemorrhage and bleeding from the head and trunk not amenable to tourniquet control, Stop the Bleed™ recommends direct pressure and packing. Turnbull also outlined these procedures in his text. In those parts of the body where a tourniquet cannot be used, as in the head and trunk, pressure with the hand must be applied; or where it cannot be made, the application of pieces of sponge, or dossils of lint, may be pressed upon the mouths of the bleeding vessels, till a more effectual restraint of the bleeding can be procured.
9
Pressure dressings have a history as old as the tourniquet. In the Oxford English Dictionary, “dossil” is an archaic term for “a plug of lint or rag for stopping a wound,” the second definition after its obsolete usage as “a plug for a barrel.” 10 The first use of the word “dossil” was in an English translation of a text on surgery by Hanss Jacob Wecker, Compendius chyrurgeri (1585), in the section of the book devoted to tumors. 11
Demonstrating that at times it takes centuries for surgeons to learn, he described incising a large aneurysm the length of his patient’s thigh. Only a half inch beneath the skin the surgeon entered the calcified rind of the aneurysm filled with “a gallon and a half” of clotted blood and grumous material. 11 No notation was made of the outcome of the misadventure. (Nor would he be the last to mistake a femoral aneurysm for a groin abscess.)
To forestall further enlargement of the aneurysm, he recommended a pressure dressing over the swelling: “with some dozell or fitte bowlster, layde on the place, keepe the member rowled.” 11 He did not mention that the dossil is best applied before making an incision into the mass.
To control bleeding today’s trauma victims receive prehospital administration of antifibrinolytics: hemostatic dressings impregnated with kaolin and chitosan slow hemorrhage from open injuries. Yet half-millennium-old interventions are the foundations of Stop the Bleed™ courses today.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.