
Abstract

Keywords
To the Editor,
Panitumumab and cetuximab, monoclonal antibodies that target epidermal growth factor receptor (EGFR), a tyrosine kinase receptor, are now standard of care for many cancers including colorectal, head and neck, and non-small cell lung cancers. 1
Acneiform eruptions are their most common skin toxicity, with a 50% to 100% incidence rate. 2 They arise within 1 to 3 weeks of EGFR inhibitor (EGFR-i) initiation, typically on the scalp, face, back, and chest, with a peak in intensity at 3 to 5 weeks. 2 Ultimately, the eruption may lead to clinical decisions to hold or discontinue lifesaving cancer treatment. 2
We present a retrospective analysis of patients with metastatic head and neck and colorectal cancer treated with first-line monoclonal antibody EGFR-i (panitumumab and cetuximab) at our institution between January 2017 and December 2021 (Table 1).
Descriptive Management of Acneiform Eruptions by Oncologists vs. Dermatologists.
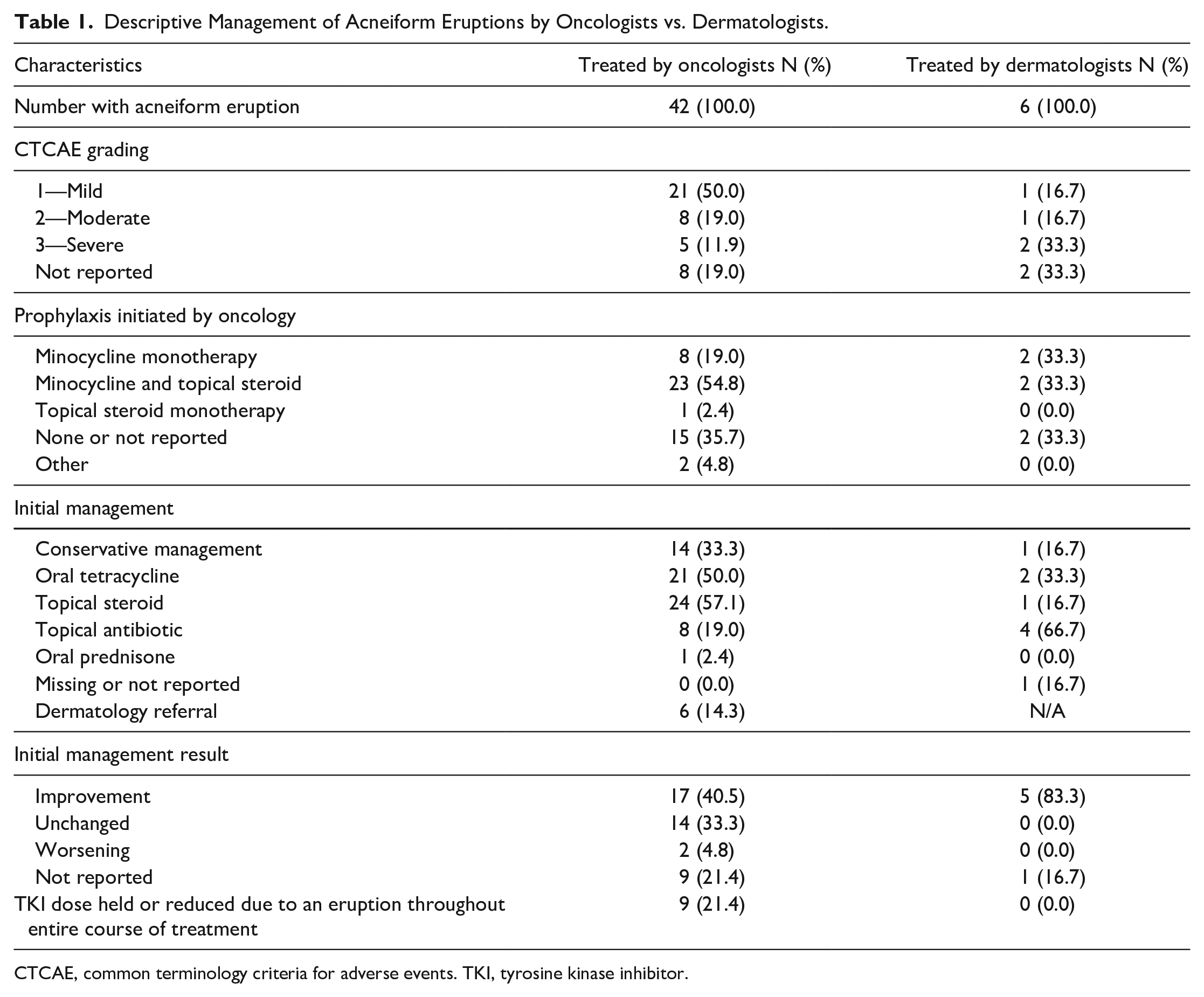
CTCAE, common terminology criteria for adverse events. TKI, tyrosine kinase inhibitor.
Of the 66 patients who started treatment, 42 (63.6%) developed an acneiform eruption: 21 (50.0%) were mild [common terminology criteria for adverse events (CTCAE) Grade 1], 8 (19.0%) were moderate (CTCAE Grade 2), and 5 (11.9%) were severe (CTCAE Grade 3 or above).
Of the patients who eventually developed an eruption, 54.8% did so despite prophylactical treatment by their oncologist with minocycline and a topical steroid, and 19.0% received minocycline monotherapy. Many current guidelines, such as the Multinational Association for Supportive Care in Cancer Skin Toxicity Study Group, recommend prophylactic treatment with minocycline (or doxycycline if kidney function is decreased), hydrocortisone 1% cream, moisturizer, and sunscreen. 3
In our study, treatments most often prescribed by oncologists for the initial management after the appearance of an eruption were various topical steroids (57.1%), followed by oral tetracyclines (50.0%), conservative management with observation and/or moisturizer (26.2%), and topical antibiotics (19.0%). This is in line with current guidelines that recommend treatment with oral antibiotics, a low-dose of isotretinoin, topical steroids, and topical antibiotics. 3 In contrast, when the patient was referred to a dermatologist, they favoured topical antibiotics (66.7%) and oral tetracyclines, specifically doxycycline (33.3%). Critically, 83.3% of patients treated by a dermatologist demonstrated improvement in their acneiform eruption, compared to 40.5% of all patients treated by oncologists. The tendency of dermatologists to include topical antibiotics in treatment, which is lower on the treatment ladder of more common non-drug-related acneiform eruptions, may reflect their expertise in treating acneiform eruptions in non-oncology settings. 4 Some dermatologists feel that that topical retinoids should not be utilized in the treatment of immunotherapy-induced acneiform eruptions, but most are comfortable using them. 5
Importantly, with dermatological consultation, no patient had their cancer treatment held or reduced, compared to 21.4% of cases treated by oncologists. Given that the emergence of an acneiform eruption is correlated with an increased survival time, treating teams should involve dermatologists in care to minimize pain, pruritus, and most importantly, interrupting needed cancer treatments. 1
Limitations of this study include the small number of patients (n = 66), and a single treating centre.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.