
Abstract
Reports of chilblain-like lesions (CLL) coinciding with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection have been described in the literature, but this phenomenon has not been critically summarized. The aim of this paper is to summarize reports of CLL coinciding with SARS-CoV-2 infection to clarify the prevalence, clinical relevance, and prognostic value of these lesions. A literature search was conducted using the Embase, Pubmed, and Scopus databases from December 2019 to June 16, 2020 using the search terms (“COVID-19” OR “coronavirus” OR “2019-nCoV” OR “SARS-CoV-2”) AND (“chilblain-like” OR “COVID toes” OR “acral”). Papers that described skin changes in patients with suspected or confirmed COVID-19 were included. A total of 31 papers were summarized, representing 813 cases of CLL. Available data suggests an equal gender distribution, mean age of 21 years, and median age of 14 years. Mild extracutaneous symptoms were reported in 53% of cases and 47% were asymptomatic. CLL occurred an average of 16 days after extracutaneous symptoms. Patients with CLL were positive for SARS-CoV-2 in 15% of cases. Lesions were mainly described as asymptomatic and/or pruritic erythematous to violaceous acral macules and plaques. Partial or complete resolution occurred in 85% of cases in a mean of 13 days. The most common histologic findings were perivascular and perieccrine superficial and deep lymphocytic infiltrates. Although a causal relationship between CLL and SARS-CoV-2 has not been confirmed, the temporal association and 15% positive SARS-CoV-2 rate in affected individuals should not be ignored.
Introduction
Coronavirus Disease 2019 (COVID-19) is caused by a novel coronavirus called severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) which first appeared in late December 2019 in Wuhan, China. 1 The virus is mainly transmitted through respiratory droplets and contaminated objects. 2 -4 SARS-CoV-2 infection has been found to have a mean incubation period of 5 days, ranging between 2 and 14 days. 5,6 On March 11, 2020 the World Health Organization declared the global outbreak of SARS-CoV-2 a pandemic. 7 Clinical features of SARS-CoV-2 infection vary widely from asymptomatic patients, to those with acute respiratory distress syndrome, multi-organ dysfunction, and death. 5 Common extracutaneous symptoms (ECS) include fever, cough, headache, sore throat, fatigue, headache, myalgia, and shortness of breath. Additional reported ESC symptoms include conjunctivitis, gastrointestinal symptoms and loss of taste and smell. 5,8,9
Since April 2020 there has been a reported surge in the literature of chilblain-like lesions (CLL) coinciding with the SARS-CoV-2 pandemic. This chilblain-like acral pattern, mainly affecting the toes, has been referred to as “COVID toes.” 5 Two early reports from France and Spain suggested that these CLL account for 19% and 38% of skin findings associated with SARS-CoV-2 infection, respectively. 10,11 Other cutaneous findings of SARS-CoV-2 infection are outside the realm of this paper. To date, a comprehensive summary of the published literature of CLL associated with SARS-CoV-2 infection is lacking. The aim of this paper is to summarize reports of CLL coinciding with SARS-CoV-2 infection to clarify the prevalence, clinical relevance, and prognostic value of these lesions.
Methods
A literature search was conducted using the Embase, Pubmed, and Scopus databases from December 2019 to June 16, 2020 using the search terms “COVID-19” OR “coronavirus” OR “2019-nCoV” OR “SARS-CoV-2” AND “chilblain-like” OR “covid toes” OR “acral.” Title, abstract and full-text screening was conducted in duplicate by 2 reviewers (N.K. and I.M.) using Covidence online systematic review software (www.covidence.org). No language restriction was applied to our search and no studies were excluded by language. The references of included studies were reviewed to ensure relevant studies were not missed. Data not published in the literature, data published only in conferences, and papers not reporting skin changes coinciding with SARS-CoV-2 were excluded. The following information was extracted from studies included in this review: author, date, country, study design, number of cases, age (mean, median, range) in years, sex, ECS, SARS-CoV-2 test result, morphology and symptoms associated with CLL, body site, temporal association with ECS, severity of ECS, outcome of lesion and recurrence.
Results
Overall, 31 papers met the inclusion criteria and were summarized in this review (Supplemental Figure S1), representing 813 total cases of CLL associated with SARS-CoV-2 infection (Supplemental Table S1). Included studies were published between April to June 2020, with 52% of articles being published in May. Twelve papers were from Italy, 11 from Spain, 4 from France, 2 from the United States and one each from Belgium and Kuwait (Table 1). Variability of reported data made comparison and calculation of some data unfeasible.
Summary of Important Clinical Characteristics and Outcomes of Chilblain-Like Lesions Occurring During the SARS-CoV-2 Pandemic Up to June 2020.
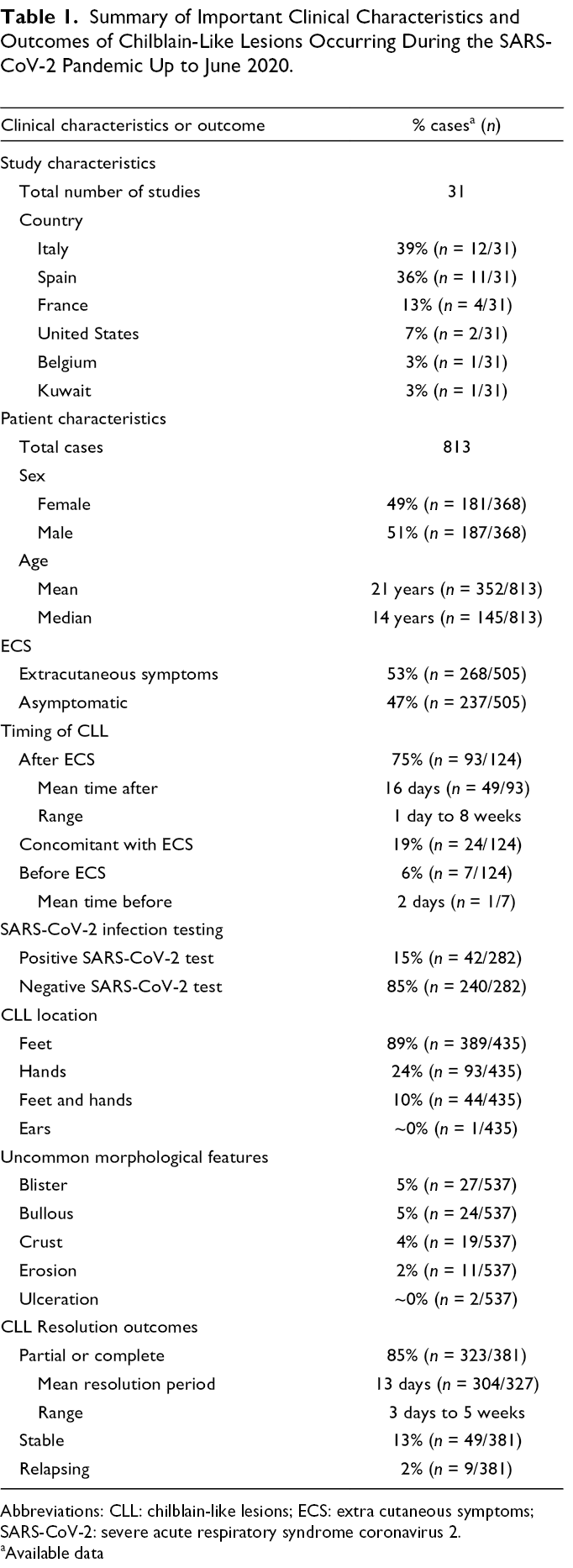
Abbreviations: CLL: chilblain-like lesions; ECS: extra cutaneous symptoms; SARS-CoV-2: severe acute respiratory syndrome coronavirus 2.
aAvailable data
Sex was available for 368 cases (45%): 181 (49%) were female and 187 (51%) were male. Age data were available for 497 cases (61%) with a range of 1-91 years. The mean age was 21 years and the median was 14 years, based on available data from 352 cases (43%) and 145 cases (18%) respectively (Table 1).
In 505 cases (62%) where ECS were assessed, 268 (53%) had ECS, and 237 (47%) were asymptomatic (Table 1). There were an additional 238 cases (29%) for which the authors had reported ECS but the exact case numbers were unspecified. For 70 cases (9%) no data on ECS was collected. When cases were associated with ECS, available data showed that CLL appeared after ECS in 93 cases (75%), at a mean of 16.4 days after the extracutaneous symptoms, ranging from 1 day to 8 weeks, which was calculated with data available from 49 cases (53%). Only 24 CLL cases (19%) occurred at the same time as ECS and in only 7 cases (6%) CLL appeared before ECS. Of 505 cases reporting ECS, 504 (>99%) cases were asymptomatic or mild (Table 1). The most commonly reported ECS included fever, cough and other general respiratory symptoms, gastrointestinal symptoms, pharyngitis and headache. Other reported symptoms included general weakness, anosmia, and ageusia.
Papers reported testing by reverse transcription polymerase chain reaction (RT-PCR) in 16 papers (52%), both RT-PCR and antibody testing serology in 9 papers (29%), and antibody testing alone in one paper (3%). SARS-CoV-2 infection data were unavailable in 5 papers (16%). A total of 282 patients (35%) were tested for SARS-CoV-2 infection in which 42 (15%) were confirmed positive and 240 (85%) confirmed negative (Table 1). Testing was not done in 211 cases (26%). Additionally, there were 201 cases (25%) in which testing was being done, but there was an unspecified number of positive tests. Data were not available for 119 cases (15%). Many papers reported suspected cases which had contact with a confirmed SARS-CoV-2 infected patients (5 studies), suspected cases (6 studies), or high risk areas (2 studies). 11 -20
CLL were most commonly described as erythematous to violaceous macules (11 studies), plaques (9 studies), or papules (8 studies) with edematous and/or purpuric areas (13 studies). 10,12 -37 Lesions occasionally developed bullae (6 studies), blisters (5 studies), erosions (4 studies), and crust (4 studies). 12,13,15,16,19,22 -26,27,30–33 -33,37,38 Available data showed that CLL were most commonly on the feet (toes, heels, and/or soles) in 89% (n = 389/435) of cases, hands (fingers) in 24% (n = 93/435), and feet and hands in 10% (n = 44/435) (Table 1). Lesions presented asymptomatically or with mild pain, burning and/or pruritis. Outcomes were reported for 381 cases (47%) with majority showing good prognoses: 323 (85%) had partial or complete resolution, 49 (13%) were stable, and 9 (2%) had a relapsing course. Mean resolution period was 13 days ranging from 3 days to 5 weeks and calculated from available data from 304 cases (37%) (Table 1).
Biopsies obtained in 11 studies reported histologic findings. 11,13 -19,23,26,28,33,37,38,38 Dermal perivascular, perieccrine and periadnexal superficial and deep lymphocytic infiltrate was the most commonly reported finding. 11,13 -19,23,26,28,33,38,38 In addition, vacuolar changes, papillary derma edema, singly necrotic keratinocytes, and lichenoid dermatitis were observed. 11,14,15,19,23,26,38 A few studies showed dermal vessel thrombi, microthrombi, and dermal fibrin. 11,13,23,26,28 Some studies described findings suggestive of vascular involvement, such as vessels with endothelial cell swelling, endothelial activation, and red blood cell extravasation. 13,23,26,28,33
Discussion
Since April 2020 there has been a reported surge of CLL coinciding with the COVID-19 pandemic and additional reports are continuously emerging. In this review, we comprehensively summarize the emerging evidence regarding CLL associated with COVID-19.
Chilblains, also known as pernio, is an inflammatory cutaneous manifestation from a maladaptive response to non-freezing cold weather. 39 Chilblains are most commonly idiopathic but may be associated with an autoimmune connective tissue disease, hematologic malignant disease and rarely viral infections.39 Chilblains are located mainly on the toes, fingers, ears, and face; are often present with pruritic, painful, swollen erythematous and violaceous macules, papules, plaques, and nodules; and persist for over 24 hours. 39,40 Blisters, erosions, and ulcerations may be present and usually spontaneous resolve in 1-3 weeks. 39 Histological features, often considered non-specific, include a superficial and deep perivascular and perieccrine, with or without periadnexal lymphocytic infiltrate as well as dermal edema. 39,41,42 Necrotic keratinocytes and vascular microthrombi can be found in the dermis. 42,43
The papers included in this review suggest that cases of CLL associated with COVID-19 share some clinical and histologic features with classic chilblains. However, the reported CLL coinciding with SARS-CoV-2 infection also differ from classic chilblain lesions for several reasons. Firstly, demographic data for CLL shows an equal gender distribution and a surge in pediatric cases compared with classic chilblains seen in a predominantly young to middle-aged female population and uncommonly in children. 39 Secondly, in CLL skin changes have been reported on the heels and soles which distinguish these lesions from classic chilblains. 12,16,22,27,37 Thirdly, several papers report no association with cold weather. 11,22,23,31,33,35 The acute rapid spike in incidence of these CLL without cold exposure differentiates from chilblains and suggests an alternative etiology. Regions such as Murcia and Aragon in Spain, where there were zero reported diagnoses of chilblains in 2019 have suddenly in recent months reported surges of over 40 chilblain-like cases. 24,35 Another example of the recent surge CLL is a paper that compared 3 cases of chilblains in all of 2019, to 30 cases over the last few months in the metropolitan area of Milan, a catchment area of 3 000 000 people. 14 In addition, the surge in CLL cases have a temporal relationship with the outbreak of COVID-19 as all of the reported surges appeared quickly after peak incidences in Spain, Italy and France. 12,15,22,23,35 While the temporal correlation does not prove causation, the surge in cases is highly suggestive.
The etiology of these CLL is currently unknown. Available data rules out a history of cold induced, autoimmune, coagulative, or malignant causes of chilblains. 10,11,13,15,20,44 Viral etiologies including Epstein–Barr virus, cytomegalovirus, Coxsackie virus, parvovirus B19, herpes simplex virus, measles morbillivirus, rubella virus, human immunodeficiency virus, hepatitis B, and hepatitis C have been ruled out in many cases. 13,20,28,33,34,37 Skin changes secondary to a drug reaction have also ruled out. 24,33
A strong correlation does not prove causation and debate continues regarding the relationship of CLL with SARS-CoV-2 infection. However, the temporal relationship and the absence of other triggers have led many authors to support a causative relationship between CLL and SARS-CoV-2. 10,13,15,22,26,31,35 Recurring theories on etiology include an immune dysregulation or a coagulation disorder induced by the SARS-CoV-2 infection. 11,13,23,28,31,45 Specifically, authors have suggested an exaggerated innate immune response and/or a delayed immune-mediated response. 15,24,30,31,46,47 However, immunologic studies have yet to be completed to assess this. 13,20 Secondly, there have been reports of acral ischemic lesions due to thrombosis usually in adults with severe SARS-CoV-2 disease. 48 These patients present with hypercoagulation and elevated D-dimer levels. 23,26 While this may be a discrete disorder more related to the virus in critically ill patients, some authors suggest that there is a continuous spectrum of disease from erythematous macules and CLL to gangrene or digital ischemia. 23,45 This theory is supported by findings of vascular microthrombi, elevated D-dimer levels, dermal vessel thrombi and clinical features suggesting vaso-occlusion. 11,13,23,28
On the other hand, in the absence of confirmed SARS-CoV-2 infection, these CLL may be unrelated to the SARS-CoV-2 virus. 21,22,24,34,37 Proposed etiologies in these cases include environmental factors during the pandemic such as prolonged barefoot exposure in cool indoor environments, restrictions leading to lack of sun exposure and vitamin D levels and physical inactivity resulting in vascular stasis and microthrombosis. 15,24,37,49 However, the likelihood of the numbers of patients presenting with these findings as a result of these reasons is low and it is more likely that these patients had false negative tests.
At this time, there are only 282 cases (35%) of reported CLL with available SARS-CoV-2 status. Therefore, SARS-CoV-2 status (past or present) is missing for the majority of reported cases and this is a major limitation in the published literature. Initially when CLL were reported, testing was limited due to either a lack of resources or due to strict testing criteria, in which mild symptoms or asymptomatic patients did not qualify for testing. 31,35,49,50 In addition, there has been speculation in many papers concerning the validity and reproducibility of these early diagnostic tests. 15,28,51 Four cases which tested negative to nasopharyngeal swab and aspirate for SARS-CoV-2 in April were retested with the new availability of validated serology tests with one patient testing positive. In another paper, of the 19 patients who initially tested negative with nasopharyngeal swabs, 6 patients subsequently tested positive with serological testing. 13 Our literature review reveals that in confirmed SARS-CoV-2 cases the CLL manifest late in the disease course, usually after ECS. The delayed manifestation of cutaneous symptoms brings into question the validity of tests done using upper respiratory swabs in which the virus usually becomes undetectable after 6-11 days. 13,52 These instances demonstrate the concern of false negatives possibly due to undetectable viral load which in turn may underestimate the number of CLL SARS-CoV-2 positive cases. As well, CLL patients are often asymptomatic (no ECS) and do not tend to have the cytokine storm associated with a more severe disease course and this may be related to a lower viral load. However, more data are required to draw firm conclusions on this regard.
Additionally, the specific geographical distribution of studies, with 90% (n = 28/31) of studies published from Western Europe, is important to discuss. We suggest several factors which may play a role in this clustered geographical distribution. First, although exposure to cold weather has been ruled out in many cases, we note that historically, idiopathic chilblains have been frequently reported in Western Europe with its damp climate enhancing the conductivity of cold. 53 Second, a genetic predisposition to chilblains has been suggested, supported by observations of familiar clustering and a robust phenotypic familial aggregation in chronic chilblains. 54 We suggest that reported familial clusters and geographic distribution may warrant a genetic predisposition for CLL to be considered. 16 Additionally, other factors such as ethnicity, diet and altitude have been shown to affect cold induced vasodilatation, a proposed mechanism of chilblains, and may also warrant consideration. 54,55 Further, body mass index, a potentially predisposing factor of chilblains, has yet to be considered. 56,57
There are several limitations for this review. First, some studies pooled CLL into a broader category of skin changes and no data were provided for individual lesions within the category, limiting our ability to report on the prevalence of positive cases and extracutaneous symptoms. Second, the limited geographical locations represented in this study may impact the generalizability of these findings. Third, study data is limited by availability of valid testing and strict SARS-CoV-2 related testing restrictions. Additionally, knowledge surrounding SARS-CoV-2 infection and dermatological symptoms is continuously being updated and as this study was based on current available information up to June 16, 2020, understanding of CLL may change as more literature becomes available. Further, data not published in the literature and data only published in conferences were excluded due to the availability of higher quality evidence. Finally, variability of reported data and lack of follow up in many cases limited the quality of results. In order to mitigate these limitations, the Covid-19 Dermatology Registry was established by the American Academy of Dermatology for ongoing, consistent collection and analysis of skin manifestations of COVID-19. 58 We encourage physicians and healthcare providers submit cases to the Covid-19 Dermatology Registry.
In conclusion, this review summarizes 31 papers presenting 813 total CLL cases coinciding with SARS-CoV-2 infection. These surges have a temporal relationship with SARS-CoV-2 infection and seem to affect mostly young individuals with an equal gender distribution. Available data shows half of CLL cases were associated with mild ECS, and the rest were asymptomatic. Only 15% of cases were confirmed positive, however this may be underreported due to a lack of testing availability and poor test validity. Most often these CLL arose late in the disease course which could affect testing accuracy. CLL were described mainly as asymptomatic or painful and/or pruritic erythematous to violaceous, edematous, purpuric acral macules, plaques, and papules, which spontaneously partially or completely resolved in an average of 13 days. Although a causal relationship between CLL and SARS-CoV-2 has not been confirmed, the temporal association, lack of typical chilblain triggers, and 15% positive SARS-CoV-2 test rate in the current literature is highly suggestive of linkage and should not be ignored. This relationship may be further investigated with widespread use of molecular and serological SARS-CoV-2 testing and ongoing systematic reporting of skin findings in SARS-CoV-2 positive individuals.
Supplemental Material
online Supplementary file 1 - Supplemental material for Chilblain-Like Lesions (CLL) Associated With COVID-19 (“COVID Toes”): A Systematic Review
Supplemental material, Online Supplementary file 1, for Chilblain-Like Lesions (CLL) Associated With COVID-19 (“COVID Toes”): A Systematic Review by Nadia Kashetsky, Ilya M. Mukovozov and James Bergman in Journal of Cutaneous Medicine and Surgery
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.