
Abstract
Background
Posterior circulation ischemic stroke (PCS) accounts for up to 25% of all ischemic strokes but remains frequently under-recognized due to atypical symptoms and poor representation in conventional stroke scales. Early diagnosis is critical yet challenging. This study aimed to derive a pragmatic clinical scoring tool, the PCS-SCORE, to identify patients at high risk of PCS based solely on bedside features.
Methods
We retrospectively analyzed 5163 patients from a prospective stroke registry, including 1571 with -confirmed PCS. Key predictors were identified through multivariable logistic regression and lasso modeling. Variables were weighted according to regression coefficients and clinical relevance. The final PCS-SCORE (0-9 points) included: diabetes (1 point), hypertension (1), male sex (1), double/blurred vision (2), vertigo with vomiting (2), and incoordination (2).
Results
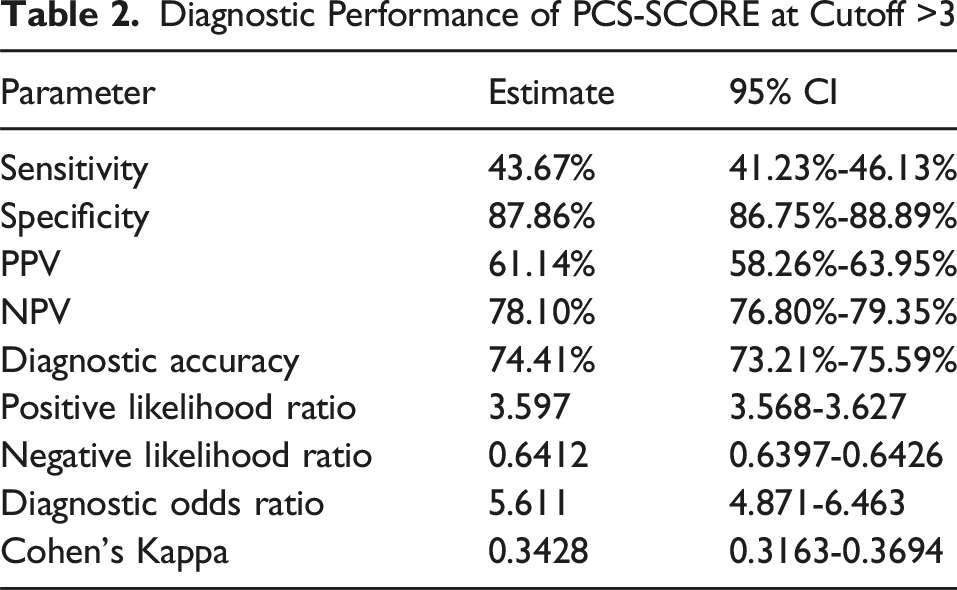
At a score threshold >3, the PCS-SCORE achieved an area under the curve (AUC) of 0.76, with 87.9% specificity and 43.4% sensitivity. Raising the threshold to >4 increased specificity to 94.4% (sensitivity 27.9%). Higher scores corresponded with progressively increased likelihood of PCS, enabling confident identification of high-risk patients.
Conclusion
The PCS-SCORE is a simple, highly specific bedside tool for early detection of posterior circulation strokes. Its rule-in strength makes it especially useful in prehospital settings, resource-limited environments, and crowded emergency departments. Prospective validation is ongoing.
Plain Language Summary
Posterior circulation ischemic stroke (PCS) represents up to a quarter of all ischemic strokes but is often missed because symptoms can be atypical and current stroke scales under-represent these cases. Prompt recognition is crucial for timely treatment, yet diagnosis remains challenging, particularly in prehospital or resource-limited settings. This study set out to develop a practical, easy-to-use clinical scoring tool—the PCS-SCORE—designed to identify patients at high risk of PCS based entirely on bedside findings. Researchers retrospectively reviewed data from a prospective stroke registry containing 5,163 patients, of whom 1,571 had confirmed PCS. Predictive factors were identified using multivariable logistic regression and lasso modeling. Each factor was assigned a point value based on statistical weight and clinical significance. The final PCS-SCORE ranges from 0 to 9 points and includes six predictors: diabetes mellitus (1 point), hypertension (1 point), male sex (1 point), double or blurred vision (2 points), vertigo with vomiting (2 points), and incoordination (2 points). Performance analysis showed that at a threshold score greater than 3, the PCS-SCORE achieved an area under the curve (AUC) of 0.76, with 87.9% specificity and 43.4% sensitivity. Increasing the threshold to greater than 4 improved specificity to 94.4%, though sensitivity decreased to 27.9%. Importantly, higher PCS-SCORE values correlated with a markedly increased probability of PCS, supporting its utility as a “rule-in” diagnostic aid. It’s high specificity makes it particularly useful for quickly identifying likely PCS cases, helping clinicians prioritize further imaging and urgent intervention. This is especially valuable in crowded emergency departments, rural or low-resource hospitals, and prehospital environments where rapid triage decisions are critical. In conclusion, the PCS-SCORE is a simple, bedside clinical tool with strong potential to improve early detect.
Introduction
Posterior circulation ischemic stroke (PCS) comprises up to a quarter of all ischemic strokes. 1 They are often elusive to diagnose due to nonspecific symptoms and the poor performance of commonly used clinical screening tools, such as F.A.S.T, 2 the Recognition of Stroke in the Emergency Room (ROSIER) Scale. 3 and the National Institutes of Health Stroke Scale (NIHSS), 4 which are predominantly designed to detect anterior circulation events. 5
Additionally, standard computed tomography (CT), the most widely available neuroimaging modality in emergency departments (EDs), often fails to detect PCS, leading to missed diagnoses and lost therapeutic opportunities. 6 This diagnostic ambiguity contributes to physician anxiety, particularly in patients presenting with dizziness, and has driven an over-reliance on advanced imaging techniques such as CT perfusion and MRI. 7 While more sensitive, these tools increase emergency room wait times, lead to potentially avoidable admissions, inflate bed occupancy, and consume valuable healthcare resources.8-10
Several attempts have been made to improve bedside diagnosis of PCS by adapting existing tools,such as BE-FAST (Balance, Eyes, Face, Arm, Speech, Time) 11 and POST-NIHSS, 5 or by introducing PCS-specific scales like the Adam’s Scale of Posterior Stroke (ASPOS), 12 the Israeli Vertebrobasilar Stroke Scale (IVBSS), 13 the TriAGe + Score, 14 and the PCI score. 15 While these instruments show promise, most were developed from relatively small cohorts, exhibit varying levels of complexity, and remain underutilized in real-world clinical practice.
Given the high morbidity associated with missed or delayed PCS diagnosis — particularly in strokes affecting the brainstem or cerebellum — there is a pressing need for a simple, bedside tool that enables clinicians to estimate the likelihood of PCS based on clinical presentation. Such a tool must be pragmatic, intuitive, and scalable across settings, from rural EDs to high-volume urban stroke centers.
In this study, we leveraged a large, prospectively maintained stroke database enriched with MRI-confirmed diagnoses to derive a weighted clinical score based entirely on historical and physical exam findings. Our goal was to create a rule-in tool, the PCS-SCORE, that facilitates early detection of posterior strokes and prioritizes high-risk patients for urgent neuroimaging and intervention.
Methods
This was a retrospective derivation study using prospectively collected registry data, intended for score development and internal validation from the Qatar Stroke Database spanning 2014-2023. The registry includes all patients presenting with suspected acute stroke to Hamad General Hospital, the principal stroke center in Qatar.
Inclusion and exclusion criteria:
We included PCS patient fulfilling these criteria as published previously 1 :
Acute neurological deficit attributable to posterior circulation ischemia, including basilar artery occlusion, confirmed by computed tomographic angiography (CTA), magnetic resonance angiography (MRA), or conventional cerebral angiography.
Acute neurological deficit with brainstem involvement, manifesting as alternating hemiplegia or tetraplegia, brainstem signs, visual loss, locked-in state, coma, or death.
Coma or loss of consciousness associated with acute posterior circulation infarction demonstrated on CT or MRI.
Accordingly, PCS was defined radiologically as ischemic infarction involving the brainstem, cerebellum, occipital lobes, and/or thalami.
The PCS cohort was compared with other patients in the registry, most of whom were initially suspected of having posterior circulation stroke at first presentation but were subsequently diagnosed with stroke mimics (eg, peripheral vestibular disorders), other medical conditions, or anterior circulation ischemic stroke following definitive evaluation.
Patients were excluded only if key clinical variables required for score derivation were missing or if intracerebral hemorrhage was present.
Demographic data (age, sex), vascular risk factors (pre-existing, physician-diagnosed hypertension, diabetes mellitus), and presenting symptoms (vertigo, vomiting, diplopia, blurred vision, dysarthria, incoordination, limb weakness) were extracted. Each case underwent independent adjudication by stroke neurologists and neuroradiologists.
Univariate and multivariate logistic regression models identified variables significantly associated with PCS. The final scoring model used coefficients from the multivariable model weighted and rounded to integers. Variables were assigned 1 or 2 points based on clinical relevance and statistical strength. The maximum score was 9.
Statistical methods included logistic regression (stepwise backward) and lasso regression (λ minimized via cross-validation). Model discrimination was evaluated using AUC. Diagnostic indices, sensitivity, specificity, PPV, and NPV were calculated at several score thresholds.
Results
Scoring System

Diagnostic Performance of PCS-SCORE at Cutoff >3
Diagnostic Performance of PCS-SCORE at Cutoff >4


Predicted probability of PCS with varying weighted score values
Receiver operating characteristic (ROC) analysis demonstrated an area under the curve (AUC) of 0.76, indicating good overall discrimination between PCS and non-PCS cases. As illustrated in Figure 2, higher score thresholds improve specificity at the cost of sensitivity, reinforcing the PCS-SCORE’s utility as a high-specificity, rule-in tool for identifying patients who warrant urgent imaging and intervention. Receiver Operating Characteristic (ROC) curve for the PCS-SCORE predicting posterior circulation ischemic stroke (PCS): The area under the curve (AUC) was 0.76, indicating good discrimination between PCS and non-PCS cases. The blue curve represents the performance of the PCS-SCORE model, while the diagonal reference line indicates chance-level discrimination
Discussion
Dizziness accounts for nearly 4 million ED visits annually in the U.S., yet posterior circulation stroke is often overlooked in this population due to its non-specific presentation and lack of focal signs. 16 The PCS-SCORE addresses this gap by offering a pragmatic rule-in tool tailored to bedside evaluation, helping to prioritize imaging in high-risk presentations.
This study introduces the PCS-SCORE; a pragmatic, bedside clinical tool designed to improve early identification of posterior circulation stroke (PCS) using binary clinical features alone. Unlike traditional scales such as FAST, ROSIER, or the NIH Stroke Scale (NIHSS), which predominantly emphasize anterior circulation symptoms like aphasia and hemiparesis, the PCS-SCORE was intentionally developed to capture the more subtle and non-localizing signs typical of PCS, including vertigo, diplopia, and incoordination. 17 These atypical symptoms, often mimicked by benign conditions such as vestibular neuritis or migraine, contribute to frequent misclassification and delayed diagnosis. 16
Although extended tools like BEFAST and POST-NIHSS have attempted to address these limitations, they either add complexity or still rely on structured neurological assessments not easily applied in fast-paced emergency settings. Similarly, posterior-specific scales such as the Adam’s Scale of Posterior Stroke (ASPOS), Israeli Vertebrobasilar Stroke Scale (IVBSS), PCI Score, and TriAGe+, while conceptually valuable, are either derived from small cohorts, require neuroanatomical interpretation, or are heavily dependent on advanced imaging, limiting their generalizability.
Comparison Between Different Posterior Circulation Stroke Scales

Male sex remained an independent predictor in both multivariable logistic and lasso regression models after adjustment for age and vascular comorbidities, reflecting a probably observed epidemiological association rather than a proposed biological mechanism. Nevertheless, several sex specific studies have shown a male predilection to posterior circulation stroke.18,19
And while vertigo with vomiting are non-specific and may point to either central or peripheral etiology when considered in isolation. Its inclusion in the PCS-SCORE reflects its incremental value only when combined with other posterior circulation features and vascular risk factors, lending it more weight and mitigating its diagnostic overlap with peripheral vestibular disorders.
This specificity is not merely a statistical artifact as it has tangible clinical utility. In emergency departments (EDs) operating under strain, low-specificity tools can flood diagnostic pathways with false positives, driving unnecessary imaging, prolonged wait times, bed overuse, and increased system inefficiency.7,10 Crucially, they also contribute to provider mental fatigue (a state of cognitive overload stemming from sustained diagnostic uncertainty, repetitive decision-making, and pressure to avoid missed diagnoses). 20 This is particularly problematic in PCS, where vague symptoms like dizziness, nausea, or unsteadiness often lack clear localizing signs. Clinicians, faced with ambiguous presentations, may default to defensive practice patterns: over-reliance on MRI, unnecessary admissions, or low-threshold referrals, all of which inflate workload without improving yield.
The PCS-SCORE is not intended to determine whether neuroimaging should be performed nor to delay reperfusion therapy. All patients with suspected stroke should continue to follow established acute stroke pathways. Rather, the score functions as a triage-support, rule-in tool, assisting clinicians in prioritizing high-probability PCS cases for urgent imaging in settings with diagnostic congestion or limited resources.
This approach enhances diagnostic precision by providing clinicians with a potential cognitive scaffold to mitigate alarm fatigue and the resultant downstream over-investigation.21,22 While high sensitivity is desirable for broad screening tools, the PCS-SCORE was not intentionally designed as a high-specificity instrument a priori. Rather, high specificity emerged empirically during model derivation and performance analysis. This observed rule-in strength suggests that the PCS-SCORE may complement existing high-sensitivity screening tools, such as FAST or BE-FAST, by helping prioritize patients with a higher probability of posterior circulation stroke in selected clinical settings thus, filling a critical gap in posterior circulation stroke triage where specificity, simplicity, and real-world usability converge.
Limitation
Limitations include retrospective derivation, absence of external prospective validation at this stage, and reliance on subjective symptom reporting (eg, vertigo, incoordination). As a registry-based derivation study, a formal a priori sample size calculation was not performed; however, the large cohort size (>5000 patients) exceeds that of most previously published posterior circulation scoring systems.
Conclusion
The PCS-SCORE is a simple, clinically intuitive tool that can support early diagnosis of posterior circulation strokes. It confidently identifies high-risk patients and streamlines imaging and treatment pathways, Prospective validation in real-life scenarios is needed.
Footnotes
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki. Ethical approval was obtained from the Institutional Review Board at the Medical Research Center, Hamad Medical Corporation (Research Protocol No. 03-SI-17-075).
Consent to Participate
The requirement for informed consent was waived due to the retrospective nature of the study and use of anonymized data.
Author Contributions
Dr Yahia Imam (YI) contributed to conceptualization, data curation, writing of the original draft, and writing–review and editing. Dr Rajvir Singh (RS) contributed to conceptualization, data curation, formal analysis, methodology, validation, visualization, and writing–review and editing. Dr Prem Chandra (PC) contributed to data curation, formal analysis, methodology, visualization, and writing–review and editing. Dr Ishrat Hakeem (IH) contributed to data curation and project administration. Dr Saadat Kamran (SK), Dr Ahmad Muhammad (AM), Dr Salman Al Jurdi (SAJ), Dr Suhail Hussain (SH), Dr Khawaja Hassan Haroon (KH), Dr Jon Davis Perkins (JP), Dr Ahmed Elsotouhy (AE), Dr Mohamed Sayed Abdelmoneim (MAb), Dr Zain A. Bhutta (ZB), Dr Mostafa Mahmoud (MM), Dr Ehab Mahmoud (EM), Dr Osman Koc (OK), and Prof. Dirk Deleu (DD) contributed to writing–review and editing. All authors read and approved of the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by an internal grant from the Medical Reserach Center(MRC) at Hamad medical corporation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are not publicly available due to institutional data protection policies but are available from the corresponding author on reasonable request and with appropriate ethical approvals.
Declaration of Generative AI and AI-assisted Technologies in the Writing Process
During the preparation of this work the author(s) used ChatGPT to improve language and grammar. After using this tool, the authors have reviewed and edited the content as needed and take full responsibility for the content of the publication.