
Abstract
Background and Objectives
This study aims to assess whether adult patients with encephalitis from different racial and ethnic backgrounds exhibit significant differences in clinical presentation, diagnostic findings, and outcomes.
Design and Methods
A retrospective cohort study was conducted by utilizing the electronic health records of encephalitis patients in the greater Houston and Baltimore areas. Patients were categorized by race/ethnicity into White or ethnic minority (including Black, Hispanic, and Asian patients). Data was analyzed for the presence of significant differences in clinical characteristics between the two groups.
Results
Among 599 patients, 312 (52.1%) were White and 287 (47.9%) were of an ethnic minority. White patients were more often over sixty years-old upon presentation (43.1% vs 23.9%, P < 0.001) and more likely to present with memory deficits (36% vs 26.3%, P = 0.012). Ethnic minority patients more frequently presented with co-existing HIV (20.3% vs 3.4%, P < 0.001), severe organ dysfunction (44% vs 34.4%, P = 0.028), cerebrospinal fluid (CSF) pleocytosis (white blood cell count ≥5 cells/µL) (83.1% vs 69.3%, P < 0.001), and abnormal electroencephalogram (EEG) findings (84.3% vs 71.9%, P = 0.035). Ethnic minority patients also had worse outcomes on the Glasgow Outcome Scale (GOS) as defined by GOS <4 (59.3% vs 47.2%, P = 0.005). Binary logistic regression identified abnormal magnetic resonance imaging (MRI) and Glasgow Coma Scale (GCS) <13 as independent predictors of an adverse clinical outcome (GOS <4) with an adjusted odds ratio [95% confidence interval] (P value) of 1.609 [1.042-2.486] (P = 0.032) and 2.689 [1.675-4.317] (P < .001), respectively.
Conclusion
Ethnic minority patients with encephalitis present at a younger age and are more likely to have co-existing HIV, severe initial organ dysfunction, CSF pleocytosis, abnormal EEG findings, and worse clinical outcomes. Abnormal MRI and GCS <13 are independent predictors of an unfavorable clinical outcome and may aid in risk stratification.
Plain Language Summary
Race and ethnicity have been shown to affect patient symptoms and outcomes in various diseases, including autoimmune neurological diseases. There has not yet been a comprehensive study on how race and ethnicity affects all causes of encephalitis in adults, including both infectious and autoimmune sources. Our research team used patient records from the past and from two major cities to collect data on patient demographics, symptoms, diagnostic and imaging findings, treatment received while hospitalized, and outcomes/recovery. Patients were categorized by race/ethnicity into two groups for this initial study; White or ethnic minority (including Black, Hispanic, and Asian patients). We analyzed the data to see if there were major differences in any factors between the two groups. The total number of patients was 599, with 52.1% being White and 47.9% of an ethnic minority. We found that White patients tended to present at a much older age and with memory gaps. Ethnic minority patients were sicker when they presented to the hospital in terms of other diseases they co-presented with, as well as initial imaging and lab findings. Our ethnic minority patients had worse outcomes in terms of neurological recovery and functional status by their discharge. A separate analysis showed that abnormal magnetic resonance imaging (MRI) results and a certain level of consciousness upon admission were indicative of worse outcomes by discharge. Our study revealed that ethnic minority patients with encephalitis are more likely to present younger and with more severe illness upon hospitalization, which may be a potential reason for worse functional outcomes. More work needs to be done to differentiate symptoms and outcomes between the two groups based on the cause of encephalitis (infectious vs. autoimmune). This study has also identified abnormal MRI and level of consciousness upon admission as potential predictors of worse outcomes, which should be further studied.
Keywords
Introduction
Encephalitis is an inflammation of the brain caused by an infectious or autoimmune etiology that can induce neurological and psychiatric symptoms, and if not treated immediately, can lead to serious complications such as brain injury or even death. It is estimated to occur in around 5-10 per 100,000 U.S. persons each year 1 with an average inpatient mortality rate of 5.6%,2,3 demonstrating a considerable burden of disease in the U.S.
The influence of racial disparities in autoimmune disease outcomes, such as multiple sclerosis (MS), has been established in the current literature.4-6 Though MS has a higher incidence in White people, recent research has demonstrated that ethnic minority populations, most notably African American and Hispanics, are more likely to develop worse outcomes and be negatively impacted by social determinants of health, further exacerbating differences in outcomes. 6 Research in the past decade on autoimmune encephalitis (AE) has demonstrated that non-White race is positively associated with anti-dopamine receptor 2 encephalitis incidence in pediatric patients. 7 Data has also suggested that non-White race is a risk factor for anti-N-methyl-D-aspartate receptor (NMDAR) encephalitis,8,9 with African Americans being disproportionately affected in prevalence and incidence. 10 A retrospective study in 2013 on encephalitis found that Asian/Pacific Islander patients were less likely to recover when compared to patients of other races, though the study was limited to pediatric populations. 11 No previous studies have examined the association between racial and ethnic disparities, and clinical characteristics and outcomes in all causes of adult encephalitis.
The goal of this retrospective study was to assess racial and ethnic disparities across all causes of adult encephalitis with regards to clinical characteristics, diagnostic and imaging findings, and clinical outcomes. Investigating these relationships may reveal whether certain populations experience poorer clinical prognoses and offer insight into improving outcomes for encephalitis patients. To address these objectives, we conducted a multicenter retrospective cohort study to evaluate racial disparities in adult encephalitis and identify clinical factors associated with adverse patient outcomes. Given the limited literature on racial and ethnic disparities in encephalitis, this study initially examined all-cause encephalitis and broadly categorized patients by race/ethnicity into White or ethnic minority to identify overarching patterns.
Materials and Methods
Standard Protocol Approvals, Registrations, and Patient Consents
This study was approved by the Institutional Review Boards at the University of Texas and Johns Hopkins Hospital. This was designed as a retrospective study in which adult encephalitis patients were identified from electronic health record databases from medical centers in the Greater Houston and Greater Baltimore regions between January 2005 to December 2022.
Inclusion Criteria
Patients were identified using the International Classification of Disease (ICD-9) diagnosis codes. Inclusion criteria was determined with the 2013 International Encephalitis Consortium (IEC) criteria. 12 For initial analysis, patients were dichotomized by race/ethnicity into White or ethnic minority (including Black, Hispanic, and Asian patients) to identify broad disparities, with plans for more granular stratification in future work.
Data Collection
Data was collected from patient charts, with most variables obtained from the initial patient encounter at the emergency department, including demographics, comorbidities, presenting signs and symptoms, laboratory values, and initial imaging results. The Charlson Comorbidity Index (CCI) was scored using previous medical history, with a score greater than 2 indicating the presence of comorbidity. 13 Immune status was also determined based on several factors (presence of human immunodeficiency virus (HIV), recent chemotherapy within 1 month, solid organ or bone marrow transplantation, having received ≥20 mg of prednisone or equivalent for >1 month, or congenital immunodeficiency). Several scores were calculated to assess consciousness and severity of brain injury and illness upon presentation. Glasgow Coma Scale (GCS) and Full Outcome of Responsiveness (FOUR) Score were utilized for levels of consciousness.14,15 The Sequential Organ Failure Assessment (SOFA) was utilized to determine organ function/failure at presentation and predict intensive care unit (ICU) mortality. 16 Etiology was defined as infectious, seropositive autoimmune, or unknown.
Clinical outcomes were primarily defined by the Glasgow Outcome Scale (GOS), which measures patient recovery following traumatic brain injury. 17 A score of 5 indicates good recovery with minor neurological and psychological deficits, with the rest of the scale ranging from moderate disability with functional independence (4) to death (1). Our study classified GOS <4 as an adverse clinical outcome.18,19 Other outcome measures used were length of stay (in days), ICU admission, and mortality.
Statistical Analysis
Data analysis was conducted using IBM Statistical Package for the Social Sciences version 29.0.0. Bivariate analyses of dichotomous clinical variables were performed using the Pearson Chi-Square test or Fisher’s Exact test, as appropriate. For continuous variables, the median and interquartile range (IQR) were reported, and the Mann-Whitney U test was used to compare medians. Variables with a P-value less than 0.05 and a 95 percent confidence interval were considered statistically significant. The subgroup analysis utilized the same statistical approach as the primary analysis.
A separate bivariate analysis was performed to determine variables associated with adverse clinical outcomes, as defined by GOS <4. Variables significantly associated with an adverse clinical outcome were entered into a binary logistic regression analysis, validated by bootstrapping and the Hosmer-Lemeshow test, with 95% confidence intervals.
A socioeconomic factors analysis was performed. Insurance status was recorded from patient charts and defined as public, private, dual (public and private), or none. Median household income for each patient was determined based on zip code at time of admission using the Kinder Institute for Urban Research Houston Community Data Connections Database and U.S. Census Data.
Most variables in the combined database were present in all patients. Patients who did not have data for a certain variable were excluded from the analysis of the variable.
Results
Patient Demographics and Etiology
Demographics, Etiology, and Clinical Features Between White and Ethnic Minority Populations in Adult Encephalitis

Abbreviations: HIV, Human Immunodeficiency Virus; GCS, Glasgow Coma Scale; SOFA, Sequential Organ Failure Assessment; FOUR Score, Full Outcome of Responsiveness Score.
*Significant value as defined by P < 0.05.
aP-value for difference between White and ethnic minority patients.
bImmunocompromised is defined as having Human immunodeficiency virus (HIV), recent chemotherapy (<1 month ago), solid organ or bone marrow transplantation, receiving ≥ 20 mg of prednisone or the equivalent for >1 month, or congenital immunodeficiency.
cDefined as a mean arterial pressure <70 mmHg.
Both populations had similar proportions of patients with an infectious, seropositive autoimmune, and unknown etiology (Table 1).
Onset and Clinical Presentation
The proportion of patients presenting acutely (within <5 days) did not differ significantly between the two groups (49.8% vs 54.1%, P = 0.312). More White patients presented with memory deficits (36% vs 26.3%, P = 0.012). Presence of fever, focal neurological deficits, seizures, headache, neck stiffness, nausea, photophobia, and movement disorder were comparable between the two groups. Both populations had a median GCS score of 14 upon presentation and a similar proportion of patients presenting with a FOUR Score <14 (27.4% vs 21.2%, P = 0.097). More ethnic minority patients presented with a SOFA score >3, indicating severe organ dysfunction and/or failure upon presentation (44% vs 34.4%, P = 0.028) (Table 1).
Serum and Imaging Findings
Diagnostic Findings, Treatment, and Outcomes Between White and Ethnic Minority Populations in Adult Encephalitis

Abbreviations: CSF, Cerebrospinal Fluid; CT, Computed Tomography; MRI, Magnetic Resonance Imaging; EEG, Electroencephalogram; PLEX, Plasmapheresis; IVIG, Intravenous Immunoglobulin; ICU, Intensive Care Unit; GOS; Glasgow Outcome Scale.
*Significant value as defined by P < 0.05.
aP-value for difference between White and ethnic minority patients.
bWhite blood cell count ≥5 cells/µL.
cMeets both criteria of protein count <50 and white blood cell count <50.
Treatment
A higher proportion of ethnic minority patients were treated with vancomycin compared to the White population (61.5% vs 47.2%, P < 0.001). No meaningful differences were found regarding the use of antivirals, steroids, and immunotherapy (Table 2).
Clinical Outcomes
A higher proportion of ethnic minority patients had adverse clinical outcomes (59.3% GOS <4 vs 47.2%, P = 0.005). In addition, ethnic minority patients had a greater median [IQR] length of hospitalization (12 [7-30] vs 11 [6-18], P = 0.009) (Table 2).
Logistic Regression and Bivariate Factors Associated With an Adverse Clinical Outcome, Defined as Glasgow Outcome Scale <4

Abbreviations: HIV, Human Immunodeficiency Virus; SOFA, Sequential Organ Failure Assessment; GCS, Glasgow Coma Scale; CSF, Cerebrospinal Fluid; CT, Computed Tomography; MRI, Magnetic Resonance Imaging; EEG, Electroencephalogram; PLEX, Plasmapheresis; IVIG, Intravenous Immunoglobulin; ICU, Intensive Care Unit.
aConfidence Interval.
bp-value for difference between White and ethnic minority patients.
cClinical features that were significant in the bivariate analysis, as defined by P < 0.05, were entered into a logistic regression. This included Age >60 years, Ethnic Minority Race, Charlson Comorbidity Index >2, Headache, GCS <13, and Abnormal MRI. Hosmer-Lemeshow test was not significant (P = 0.787). All variables were validated internally with bootstrap (P < 0.05).
dImmunocompromised is defined as having Human immunodeficiency virus (HIV), recent chemotherapy (<1 month ago), solid organ or bone marrow transplantation, receiving ≥ 20 mg of prednisone or the equivalent for >1 month, or congenital immunodeficiency.
eDefined as a mean arterial pressure <70 mmHg.
fWhite blood cell count ≥5 cells/µL.
Socioeconomic Status
Socioeconomic Factors Analysis by Health Insurance Status in Adult Encephalitis

Abbreviations: HIV, Human Immunodeficiency Virus; CCI, Charlson Comorbidity Index; ICU, Intensive Care Unit; GOS, Glasgow Outcome Scale.
*Significant value as defined by P < 0.05.
aDual coverage indicates having both private and public insurance plans.
bp-value for difference between different insurance plans.

Health insurance in adult encephalitis by race
Patients with dual coverage were more likely to be > 60 years old (dual 76.3% vs none 12.7% vs public 44.4% vs private 25.9%, P < 0.001) and have a CCI >2 (dual 83.1% vs none 33.3% vs public 59% vs private 33.6%, P < 0.001) compared to the other three insurance groups. Ethnic minority patients were more likely to be uninsured or on public insurance (none 70.5% vs public 64.6% vs private 40% vs dual 18.2%, P < 0.001). A greater percentage of patients with no insurance or with public insurance were immunocompromised (none 25.4% vs public 30.9% vs private 17.4% vs dual 16.9%, P = 0.005) and HIV-positive compared to those with private or dual coverage (none 23% vs public 21.5% vs private 3.7% vs dual 1.7%, P < 0.001). Lack of insurance and public insurance were associated with infectious etiology (none 50.8% vs public 52.1% vs private 38.6% vs dual 35.6%, P = 0.012), while dual coverage was associated with autoimmune etiology (dual 27.1% vs none 9.5% vs public 11.7% vs private 38.6%, P = 0.002). Lower median household income was associated with being an ethnic minority (59,224 vs 90,772, P < 0.001), immunocompromised (68,962 vs 80,335, P = 0.001), HIV-positive (50,284 vs 80,692, P < 0.001), and an infectious etiology (71,609 vs 80,122, P < 0.001) (Supplemental Table 1). ICU admission, mortality, and GOS <4 had no significant differences between insurance groups or income levels.
Etiology Subgroup Analysis
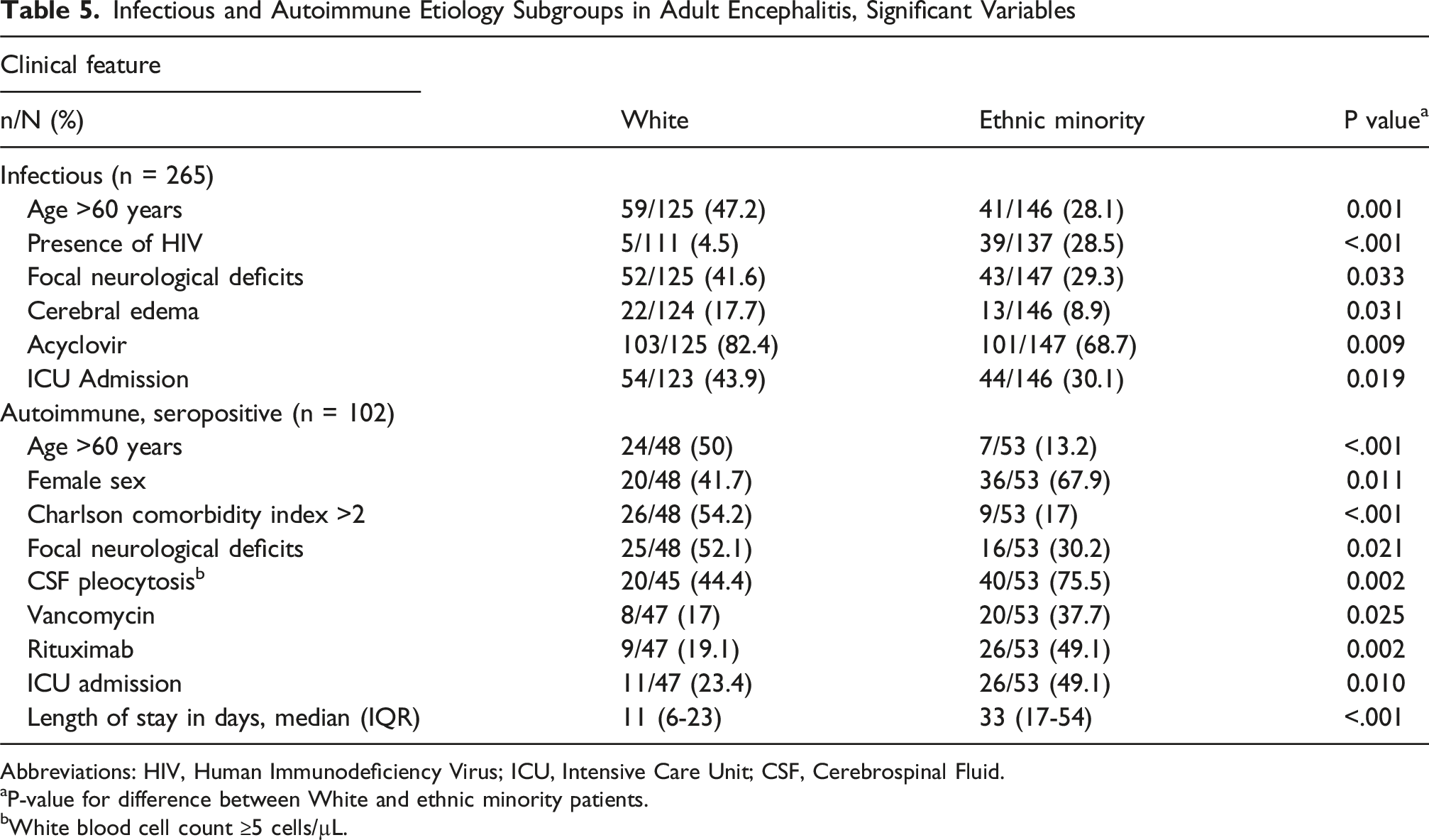
Infectious and Autoimmune Etiology Subgroups in Adult Encephalitis, Significant Variables
Abbreviations: HIV, Human Immunodeficiency Virus; ICU, Intensive Care Unit; CSF, Cerebrospinal Fluid.
aP-value for difference between White and ethnic minority patients.
bWhite blood cell count ≥5 cells/µL.
Infectious Subgroup
In this subgroup, more White patients presented >60 years old (47.2% vs 28.1%, P = 0.001) with focal neurological deficits (41.6% vs 29.3%, P = 0.033) and cerebral edema (17.7% vs 8.9%, P = 0.031). They were also more likely to receive acyclovir (82.4% vs 68.7%, P = 0.009) and require ICU admission (43.9% vs 30.1%, P = 0.019). More ethnic minority patients presented with HIV (28.5% vs 4.5%, P < .001).
Autoimmune Subgroup
In this subgroup, more White patients presented above >60 years old (50% vs 13.2%, P < .001) with a CCI >2 (54.2% vs 17%, P < .001) and focal neurological deficits (52.1% vs 30.2%, P = 0.021). Ethnic minority patients were more likely to be female (67.9% vs 41.7%, P = 0.011), present with CSF pleocytosis (75.5% vs 44.4%, P = 0.002), receive vancomycin (37.7% vs 17%, P = 0.025) and rituximab (49.1% vs 19.1%, P = 0.002), require ICU admission (49.1% vs 23.4%, P = 0.010), and have a longer hospitalization (33 [17-54] vs 11,6-23 P < .001).
Sex-based Subgroup Analysis
We conducted an additional subgroup analysis to assess for sex-based differences between White and ethnic minority patients regarding clinical presentation and outcomes (Supplemental Table 2). Due to the number of variables in this subgroup analysis, we only included significant variables.
Male Subgroup
In this subgroup, more White patients presented >60 years old (44.3% vs 27.7%, P = 0.003) with neck stiffness (25.4% vs 11%, P = 0.018), memory deficit (36.7% vs 24.5%, P = 0.023), and movement disorder (17.4% vs 8.1%, P = 0.018). Male White patients were more likely to receive IVIG (20.9% vs 10.8%, P = 0.018) and have a GOS <4 (59.3% vs 42.9%, P = 0.007). Male ethnic minority patients were more likely to have co-existing HIV (26.9% vs 4%, P < .001), be immunocompromised (30.9% vs 19.5%, P = 0.023), and present with CSF pleocytosis (87.8% vs 67.5%, P < .001) and a higher neutrophil count (median [IQR] 10 [0-43.25] vs 1 [0-33.5]). These patients were also more likely to have abnormal CT (41.5% vs 22.6%, P = 0.013) and EEG (85.9% vs 70.9%, P = 0.012) findings, receive vancomycin (63% vs 47.5%, P = 0.007), be admitted to the ICU (44.6% vs 33.3%, P = 0.046), and have a lengthier hospitalization (median [IQR] 14 [7-29.5] vs 10,5-18 P = 0.004).
Female Subgroup
In this subgroup, more White patients presented >60 years old (41.8% vs 20.3%, P < .001) with a CCI >2 (51.6% vs 37.8%, P = 0.016) and unknown etiology (47.1% vs 33.8%, P = 0.019). Female White patients were more likely to have a GOS <4 (61.7% vs 49.3%, P = 0.042). Female ethnic minority patients were more likely to have co-existing HIV (14.1% vs 2.8%, P < .001), have a seropositive autoimmune etiology (23.6% vs 13.7%, P = 0.027), and receive vancomycin (60.1% vs 46.9%, P = 0.023) and rituximab (12.8% vs 6.1%, P = 0.049).
Comorbidity Subgroup Analysis
HIV status was significant in our initial analysis between the two groups, as was the presence of comorbidities in our etiology subgroup analysis. An additional subgroup analysis to assess the role of comorbidities in clinical outcomes and socioeconomic status demonstrated the following results.
Presence of Comorbidity (CCI >2) Subgroup
In this subgroup, more White patients had a GOS <4 (66.4% vs 50.9%, P = 0.013) and higher median household income (median [IQR] 90,468 [66,025-120,947] vs 55,842 [45,714-73,148], P < .001). ICU admission, length of hospitalization, mortality, and presence of insurance did not differ between the two populations (Supplemental Table 3).
Absence of Comorbidity (CCI ≤2) Subgroup
In this subgroup, more White patients had a GOS <4 (54.7% vs 42.4%, P = 0.036) and had insurance (92.1% vs 80%, P = 0.004), along with a higher median household income (median [IQR] 93,115 [69,559-124,933] vs 68,141 [49,237-92,624], P < .001). Ethnic minority patients had a lengthier hospitalization on average (median [IQR] 115-30 vs 9.5 [4-18.75], P = 0.002). ICU admission and mortality did not differ between the two populations.
Discussion
Our retrospective cohort study of adults with encephalitis revealed several findings: 1. White patients are more likely to present at an older age and with memory deficits, 2. Ethnic minority patients are more likely to present with coexisting HIV, abnormal EEG findings, CSF pleocytosis, receive vancomycin, and have worse outcomes, 3. Abnormal MRI and GCS <13 are independent predictors of an adverse clinical outcome, and 4. Lower socioeconomic status is associated with a higher prevalence of comorbidities and being of ethnic minority race; however, it does not significantly affect in-hospital outcomes.
Despite a robust sample size, our study revealed a significant difference in age distribution between White and ethnic minority patients with encephalitis. Notably, a significantly higher proportion of White patients presented above 60 years old, with a median of 56 years old compared to 44 in ethnic minority patients. Older age upon presentation may explain the greater proportion of White patients who presented with memory deficits. To our knowledge, there has not yet been any data revealing the substantial age gap at presentation between different racial groups in encephalitis, a disease that presents with both infectious and autoimmune etiologies. It is known that anti-NMDAR autoimmune encephalitis more commonly presents initially in younger adults, 9 and that multiple sclerosis presents earlier with higher disease severity in Black populations. 4 A study done in the UK in 2022 revealed that neurological autoimmune diseases like myasthenia gravis and multiple sclerosis were diagnosed earlier in mixed-race, South Asian, and African-Caribbean populations than in White populations. 21 The authors hypothesized that increased inflammation at a younger age, psychosocial stress, socioeconomic status, and mode of onset of disease could all be potential factors contributing to an earlier onset of autoimmune disease in non-White patients, as seen in our ethnic minority patients. With regards to infectious encephalitis, a substantially higher percentage of ethnic minority patients in our study had coexisting HIV, possibly predisposing them to infection at an earlier age and playing a part in the substantial age difference at presentation.
Ethnic minority patients were more likely to present with severe organ dysfunction and/or failure, CSF pleocytosis, and abnormal EEG findings. The higher initial disease severity observed in ethnic minority patients is likely due to a complex, multifactorial etiology. Contributing factors may include underlying immunodeficiency, limited access to primary or preventative care, sociocultural barriers to timely treatment, and potential genetic predispositions to a pro-inflammatory state at a younger age.21,22 CSF pleocytosis has also been found to be associated with greater neurologic severity in encephalitis patients at admission.
23
In our study, patients of an ethnic minority were more likely to receive vancomycin and have an adverse clinical outcome as defined as GOS <4, with a longer hospitalization on average. Of note, mortality rates were comparable between the two populations, suggesting that a higher proportion of ethnic minority patients were discharged with severe disability (GOS score = 3) or in a neurovegetative state (GOS score = 2) compared to White patients (Figure 2). In conjunction with the finding that ethnic minority patients presented with greater disease severity initially, it is possible to conclude that these patients were more likely to have adverse clinical outcomes due to their initial presentation, rather than any major factors during their hospitalization. Glasgow outcome scale in adult encephalitis by race
Our logistic regression analysis identified abnormal MRI as an independent predictor of an adverse clinical outcome as defined by GOS <4. In autoimmune encephalitis, MRI has been shown to have little association with outcomes as defined by Modified Rankin Scale (mRS), seizure rate, or relapse/mortality rates. 24 However, data has shown specific MRI abnormalities to be independent predictors of adverse outcomes (mRS) in certain patient populations; eg, abnormalities in >3 lobes and left thalamic lesions in herpes simplex encephalitis 25 and focal cortical hyperintensity in pediatric encephalitis patients. 26 Our results suggest that further work is needed to define the prognostic value of MRI in outcomes of patients with encephalitis, with particular attention to specific MRI abnormalities and the interplay with etiology. Age over 60 years was significantly associated with GOS <4 in our initial bivariate analysis, but was found to not be an independent predictor of GOS <4 after adjustment. There are current mixed reports on whether older age is an independent predictor of adverse clinical outcomes in encephalitis,24,27 and our regression suggests that age does not play a substantial role in clinical outcomes in encephalitis when adjusting for other factors. GCS <13 has been previously found to be another independent predictor of an adverse clinical outcome, 27 demonstrated by our binary logistic regression as well.
Recent research has suggested non-White ethnicity as a risk factor for NMDAR encephalitis,8,9 which disproportionately affects African American, Hispanic, and Asian/Pacific Islander persons in incidence and prevalence,10,28 though there has not yet been a study looking at race in all subtypes of autoimmune encephalitis. Our study did not find a higher incidence of seropositive autoimmune encephalitis among ethnic minority patients compared to White patients (18.5% vs 15.7%, P = 0.369). This may be due in part to the exclusion of at least 25 ethnic minority patients with probable and possible seronegative autoimmune encephalitis (ie, limbic encephalitis, brainstem encephalitis, Hashimoto’s encephalopathy) from the seropositive autoimmune etiology group and inclusion into the unknown etiology group. One additional factor to consider is that data was extracted from two large metropolitan areas in the U.S. with differing racial makeup, possibly contributing to further variation from previous studies.
Socioeconomic Analysis
Public insurance, lack of health insurance, and lower median household income were associated with ethnic minority race, underlying health conditions (immune status, coexisting HIV), and infectious encephalitis. Of note, patients with autoimmune encephalitis were more likely to have private or dual insurance, and higher median household income while those with infectious encephalitis were more likely to have public or no insurance, and lower median household income. The association we found between autoimmune etiology and patients on dual insurance may be partially due to the extensive and costly workup that precedes a diagnosis of autoimmune encephalitis. A study in 2019 found that hospital charges and length of stays for patients diagnosed with autoimmune encephalitis were three to four times higher than for those with herpes simplex encephalitis, a common type of infectious encephalitis. 29 In our study, the disparities found at initial presentation did not appear to translate into differences when comparing outcomes (ICU admission, GOS, mortality rates). The lack of substantial difference in outcome between insurance groups and income levels suggests socioeconomic status plays a role in overall health characteristics upon presentation, but that patients of different races and economic backgrounds may receive similar care during hospitalization. However, this socioeconomic analysis is limited to insurance and household income, and further analysis should include education levels, social support, food insecurity, and environmental factors.
Subgroup Analyses
Within the etiology subgroup analysis, age >60 years was still significant within both infectious and autoimmune subgroups, demonstrating that etiology may not play a substantial role in the age of onset of encephalitis. Within the infectious subgroup, more ethnic minority patients presented with HIV, suggesting the role of immunodeficiency in predisposing patients to infectious CNS disease. More ethnic minority patients in the autoimmune subgroup were female, consistent with previous data demonstrating the prevalence of autoimmune encephalitis in females.9,26 Recent research has found that the CCI score was significantly higher in encephalitis patients without a viral etiology. 30 Coupled with our finding that a CCI >2 was only significant between our two population groups within the autoimmune subgroup, this may imply an interplay between comorbidities and race in autoimmune, but not infectious disease.
The differences found between the two population groups across infectious and autoimmune encephalitis could be due to a variety of factors, 20 including variation in initial presentation, illness severity, and disease progression between races depending on encephalitis etiology, which may lead to differences in treatment. Though there were no significant differences in the proportion of both population groups presenting with each etiology cluster (infectious, seropositive autoimmune, unknown; see Table 1), our subgroup analysis highlights the importance of considering etiology in the context of race in a patient’s disease progression.
Our sex-based subgroup analysis revealed that across both males and females, a higher proportion of White patients were >60 years old and had a GOS <4, while more ethnic minority patients had coexisting HIV and received vancomycin–findings consistent with our initial cohort analysis. Notably, male ethnic minority patients presented with more severe illness at admission, as indicated by higher rates of CSF pleocytosis and ICU admission. A recent 2023 study described sex-based differences in neurocognitive outcomes following brain inflammation and infection, noting that male patients were more susceptible to infection and associated adverse outcomes such as ICU admission. 31 Existing literature suggests that sex hormones modulate immune response and susceptibility through the effects of estrogens, progesterone, and androgens on pro- and anti-inflammatory cytokine pathways. 32 In addition, the relationship between blood-brain barrier (BBB) permeability and sex hormones has been established, with female sex generally associated with increased BBB integrity.33-35 These biological mechanisms may partially explain why male sex appeared to exacerbate the disease severity associated with ethnic minority race in our cohort.
The intersection between race and sex has been previously examined in other neuroinflammatory diseases such as multiple sclerosis, where Black women were found to have the worst clinical outcomes. 36 In contrast, our study found greater initial disease severity among ethnic minority men. These differing sex patterns may be due to the underlying etiological distinctions of each disease, with multiple sclerosis being an autoimmune condition and encephalitis encompassing both infectious and autoimmune etiologies. The protective role of estrogen in memory function has also been reported. 37 Our male patients did indeed have differences in presence of memory deficits, suggesting an interplay between age, race, sex, and memory. Additionally, female ethnic minority patients more frequently presented with autoimmune encephalitis, further highlighting the intersectional relationship between female sex, ethnic minority race, and autoimmune disease.9,26
In our comorbidity subgroup analysis, White patients were more likely to have a GOS <4 regardless of comorbidity status. While pre-existing health conditions likely influence clinical outcomes (the proportion of patients with GOS <4 was higher in both White and ethnic minority patients with comorbidities), they do not appear to completely account for differences in neurological recovery. Notably, among patients without comorbidities, there were differences in hospitalization length and insurance status between the two racial populations. This finding underscores the potential role of race in clinical outcomes even after matching patients with and without complex medical presentations. Taken together, our subgroup data strongly support that the role of racial disparities in clinical presentation and outcomes in encephalitis is complex and multifactorial.
Strengths and Limitations
Our study contributes to a limited body of knowledge on racial and ethnic disparities in encephalitis, specifically focusing on adult patients with both infectious and autoimmune etiologies included in a larger sample size. We included robust data from two large metropolitan areas in the United States.
Although a brief subgroup analysis was conducted comparing infectious and autoimmune encephalitis between our two groups, the primary focus of this study was all-cause encephalitis. A more comprehensive stratified analysis by etiology is needed in future research to better elucidate etiology-specific disparities. Additionally, patients were initially dichotomized into White and ethnic minority patients to assess broad differences; subsequent analyses will examine outcomes by individual racial and ethnic populations, including Black, Hispanic, and Asian patients. We acknowledge that grouping Black, Hispanic, and Asian patients into the ‘Ethnic minority’ population group does not account for the genetic, environmental, and socioeconomic differences between the groups.
This study was restricted to the data included in the electronic medical record due to its retrospective design. As a result, some information was missing or unknown, which resulted in a less robust sample for certain variables. The retrospective design also limited the ability to assess whether access to healthcare services was standardized across all patients, as differences in the quality and/or availability of diagnostic modalities and treatments were not readily obtainable in patients’ charts. Only patients with seropositive CSF results were classified as having an autoimmune etiology, leaving a sizable portion of patients with probable or possible seronegative autoimmune encephalitis in the unknown etiology group. The large proportion of patients with unknown etiologies upon admission suggest that encephalitis, particularly autoimmune, may be underdiagnosed or diagnosed belatedly. Though the study included data from two substantial metropolitan areas in the United States, the results may not be generalizable to less populated areas or other countries at this time. The socioeconomic analysis was limited by the fact that median household income was determined based on patient zip code, and thus was an estimate of the patient’s income per zip code area.
Conclusion
Ethnic minority patients with encephalitis tend to present at a younger age and are more likely to have co-existing HIV, severe initial organ dysfunction, CSF pleocytosis, abnormal EEG findings, and worse clinical outcomes. These findings highlight the potential role of racial disparities in contributing to disease severity and abnormal diagnostic findings at presentation, possibly leading to unfavorable clinical outcomes. Binary logistic regression identified abnormal MRI and GCS <13 upon presentation as independent predictors of a poor clinical outcome–prognostic markers that, with further validation, may help guide risk stratification and prognosis during hospitalization. Clinical outcomes did not differ between patients with varying household income levels and insurance types, suggesting excellence in equitable care across adult encephalitis patients in these two metropolitan areas.
Supplemental Material
Supplemental Material - Racial and Ethnic Disparities in Clinical Characteristics and Outcomes in Adults With Encephalitis: A Retrospective Study
Supplemental Material for Racial and Ethnic Disparities in Clinical Characteristics and Outcomes in Adults With Encephalitis: A Retrospective Study by Sienna Wu, Rodrigo Hasbun, Ralph Habis, Jordan Benderoth, Ivany Patel, Ashutosh Gupta, Megan Goyal, Arun Venkatesan, John C. Probasco, Paris Bean, Ashley Heck, Laya Rao, Rajesh Gupta in Journal of Central Nervous System Disease.
Footnotes
Acknowledgements
The authors would like to acknowledge all current and prior members of the encephalitis research collaboration between Johns Hopkins and UTHealth Houston who have made this work possible.
Ethical Considerations
This retrospective study was approved by the Institutional Review Boards at the University of Texas and Johns Hopkins Hospital. The Institutional Review Boards at both institutions have confirmed that informed consent is not required due to the retrospective nature of the study. IRB at University of Texas: Aseptic Meningoencephalitis in Adults, HSC-MS-08-0417. IRB at Johns Hopkins Hospital: Establishment of an Encephalitis and Seizure Disorder Registry and Clinical Database, IRB00083718.
Author Contributions
All authors contributed to the study conception and design. Material preparation and data collection were performed by Sienna Wu, Ralph Habis, Jordan Benderoth, Ivany Patel, Paris Bean, and Ashley Heck. Data analysis was performed by Sienna Wu and Rodrigo Hasbun. The first draft of the manuscript was written by Sienna Wu and all authors provided feedback on the manuscript. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: R. Hasbun receives personal compensation and research support from BioFire Diagnostics; R. Habis serves as study coordinator for a treatment trial for autoimmune encephalitis sponsored by Genentech; J.C. Probasco receives personal compensation for serving as Editor-in-Chief of NEJM Journal Watch Neurology and serves as site investigator for a treatment trial for autoimmune encephalitis sponsored by Genentech. All other authors have no relevant financial or non-financial interests to disclose.
Data Availability Statement
Anonymized data utilized for this study will be made available upon reasonable request to the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.