
Abstract
Background
In conjunction with more sensitive culture and molecular diagnostic testing modalities, simultaneous or sequential infection with more than 1 vector borne zoonotic pathogen is being increasingly documented in human patients. On a frequent basis, many people are exposed to apparently healthy, but infected, domestic and wild animals, the arthropod vectors with which these animals have co-evolved, and the bacterial, protozoal and other pathogens for which various animals are reservoirs. Unsuspected zoonotic transmission by scratch, bite, or vector exposures can result in chronic, indolent, or potentially life-threatening infections.
Methods
In December 2016, at 2 years of age, a male child residing in Ontario, Canada received facial scratches from a feral cat. In August 2018, seizures began 8 days after the child developed a focal, suspected insect bite rash. In June 2019, potential mold toxicity in the child’s bedroom was assessed by fungal culture and urinary mycotoxin assays. Beginning in January 2022, Bartonella spp. serology (indirect fluorescent antibody assays), polymerase chain reaction (PCR) amplification, DNA sequencing, and enrichment blood and brain cultures were used on a research basis to assess Bartonella spp. bloodstream and central nervous system (brain biopsy) infection. In 2024, using recently developed PCR and DNA sequencing targets, Babesia species infection was retrospectively assessed due to the rash observed in 2018.
Results
Although there was historical cat and suspected tick exposures, serological testing for Bartonella henselae and Borrelia burgdorferi were repeatedly negative. Sequential neurodiagnostic testing partially supported a diagnosis of Rasmussen’s encephalitis. Astrogliosis was the only brain biopsy histopathological abnormality. Bartonella henselae DNA was amplified and sequenced from enrichment cultures of brain tissue. Retrospectively, Babesia odocoilei and Babesia divergens-like MO-1 infections were confirmed by amplification and sequencing of DNA extracted from enrichment blood cultures processed in January 2022, from blood and brain tissue cultures in June 2022, and blood in January and June 2023.
Conclusions
Infection with B. henselae, B. odocoilei, and B. divergens-like MO-1, complicated by mycotoxin exposure, created a complex clinical scenario for this child, his parents, and his doctors.
Introduction
Zoonotic diseases, caused by pathogens that are transmitted from or occur in wild or domestic animals and infect humans, constitute at least 60% of all known infectious diseases, whereas 14% of human infectious diseases are vector borne, and vector borne zoonotic diseases (VBZDs) comprise 22% of all emerging human infectious diseases.1,2 These remarkable percentages are difficult to translate to clinical practice, wherein many instances highly specialized physicians attempt to address complex, chronic, and often non-specific symptoms in individual patients.3-6 The diagnosis of occult, zoonotic, and vector borne infections in patients with chronic illnesses presents numerous challenges, including obtaining a detailed animal and vector exposure history spanning years, assessing regional, national and international travel exposures, comprehending the large number of bacterial, fungal, protozoal and viral VBZD pathogens that can induce neurological symptoms, and the inherent limitations in sensitivity and specificity associated with infectious disease diagnostic testing modalities.7-9 Neurobartonelloses provide excellent contemporary examples of the medical complexity associated with geographically diverse vectors, numerous animal reservoir hosts, the increased and frequent interactions among humans, pets and wildlife, and the discovery of an increasingly large number of pathogenic Bartonella spp. in the past 2 decades. 10
Despite challenges, and in conjunction with the development and validation of more sensitive culture and molecular diagnostic testing modalities, simultaneous or sequential infections with multiple VBZDs are increasingly documented in human patients. In addition to microbiological considerations, co-infections create challenges in clinical interpretation, including assessment of atypical infectious disease patterns among coinfected patients, as well as assessing the potential medical importance of each individual infectious agent to the patient’s illness. Case-based examples of co-infection or sequential infections are numerous; however, due to limitations in diagnostic test sensitivity it is likely that these types of infections are far more prevalent than reported in current medical literature. A specific example of multiple zoonoses includes co-infection with Anaplasma platys, Bartonella henselae, Candidatus Mycoplasma hematoparvum, in a 27-year-old female veterinarian who was experiencing seizures and status epilepticus. 11 Among animals, dogs are most often infected with A. platys and Candidatus M. hematoparvum, whereas cats, dogs, and a variety of other terrestrial and marine mammalians can harbor B. henselae in their blood, tissues and pathological effusions. Due to extensive exposure to animals, their associated vectors, and biospecimens obtained from sick animals, veterinarians are at occupational risk of acquiring Bartonella spp. and other zoonotic and vector borne infections.12,13 Another recent example, illustrating the medical complexity of sequential infection, involved a complex case of B. henselae reactivation in a 26-year-old-female following SARS CoV2 infection. 14
The purpose of this case report is to document infection with 3 VBZD pathogens (Babesia odocoilei, Babesia divergens-like MO-1 and Bartonella henselae), most likely sequentially acquired, within the blood and brain of a child who developed a therapeutically refractory seizure disorder somewhat consistent with Rasmussen’s encephalitis.
Case report
On December 28, 2016, at 2 years of age, a male child residing in Ontario, Canada was scratched on the right side of the face by a semi-feral cat (Figure 1). Fever and regional lymphadenopathy, symptoms of Cat Scratch Disease (CSD), did not develop following the scratch. On August 10, 2018, his mother observed a focal rash on his right arm, thought to be an insect bite (Figure 2). Eight days later, the child had his first generalized tonic-clonic (GTC) seizure, followed by 2 GTC episodes of 30 seconds to 2 minutes in duration that resolved spontaneously. Figure 3 depicts a timeline of sequential, neurological, microbiological and treatment events for this patient. Emergency room (ER) admission resulted in no treatment or interventions. A month later, following ER admission for GTC seizures, levetiracetam (300 mg twice daily) was administered when there were no magnetic resonance imaging (MRI) brain abnormalities. In November 2018, following ER admission for GTC seizures, levetiracetam (750 mg twice daily) was increased to the maximum recommended dose. Cat scratches on the right side of the face of a 2-year-old boy. Picture from December 2016 provided by the parents. Suspected insect bite and rash. Arrow pointing to the suspected bite site. Picture from August 2018 provided by the parents. Timeline of sequential, neurological, microbiological and treatment events for this patient.


After the levetiracetam dose adjustment, the child remained seizure free for almost 2 years. When weaned off levetiracetam in August 2020, GTC seizures recurred and, for the first-time, he developed focal seizures. Between September 2020 and February 2021, there were 13 ER admissions for GTC seizures, focal seizures lasting 9 minutes or longer, cluster seizures, or status epilepticus. During this time, 4 different anticonvulsants were prescribed. As lacosamide (100 mg every 12 hours administration starting October 14, 2020) induced extreme lethargy and irritability and did not reduce seizure frequency, administration was stopped January 31, 2021. Topiramate (36 g every 12 hours) and brivaracetam (60 mg every 12 hours) administration began in January 2021. As seizures remained therapeutically refractory, eslicarbazepine (400 mg once daily at bedtime) was added in February 2021, after which seizure frequency and intensity decreased slightly. Beginning in May 2021, the maximum dose of eslicarbazepine (800 mg once daily at bedtime) was being administered. Seizure frequency further decreased, and hospital admissions for status epilepticus became less frequent, averaging once a month between June 2021 and December 2024. All 3 anticonvulsants have continued to date, during which time the child has progressively experienced increased anxiety and aggression to self and others.
Between September 2018 and May 2021, the patient had 5 routine EEGs, 1 prolonged EEG, and 3 MRI studies at the local children’s hospital. All awake and asleep electroencephalogram (EEG) results between the fall of 2020 and spring 2021 documented slow background waveforms and epileptiform discharges in the right hemisphere. Sequential MRIs were considered normal. In June 2021, a positron emission tomography (PET) scan at a children’s hospital in Montreal, Quebec documented hypometabolism involving the entire right hemisphere. Retrospective analysis of serial MRIs from 2018 to 2021 indicated subtle, progressive right hemisphere unilateral focal cortical atrophy, consistent with Rasmussen’s encephalitis (RE). 15 In August 2021, a Montreal team participated in a virtual seizure conference with the child’s local hospital in Ontario and The Hospital for Sick Children in Toronto. Parents were informed of how RE is diagnosed, the rarity of the disease, and the surgical treatment modality used, hemispherectomy. Unavoidable surgical morbidity of hemispherectomy, specifically hemiparesis and homonymous hemianopsia, was discussed, as well as the potential benefit of seizure freedom. Additionally, parents were provided an article discussing the ethical considerations involved when considering the benefits of potential seizure freedom of a hemispherectomy vs known permanent postoperative deficits of this surgery. 15 Following the principles of patient- and family-centered care (PFCC) and a shared decision-making (SDM) approach, the family was given time to consider different options for their child, which included an open brain biopsy for diagnostic purposes as well as additional neuroimaging.
The child was admitted to the Epilepsy Monitoring Unit (EMU) at Sick Kids for a prolonged EEG with video, MRI, and Magnetoencephalography (MEG) to further define the seizure focus (es). EEG with video captured both focal impaired motor onset seizures and focal retained awareness motor onset seizures. Like previous EEG results, both awake and asleep states were abnormal, with frequent interictal epileptiform discharges in the frontocentral and temporal right hemisphere. When comparing the MRI in October 2021 with an MRI in May 2021, it was determined that there was mild sulci asymmetry, with slightly more prominent sulci in the right parietal lobe superiorly and right central sulcus, with no evidence of focal cortical thinning. MSI (combined MRI and MEG) documented 50 epileptiform spikes over the right hemisphere, compared to only 3 over the left hemisphere. The combined documented abnormalities in the right hemisphere (same side as the cat scratch) resulted in differential diagnoses including Rasmussen’s encephalitis, and to a lesser extent, infection-induced encephalitis or autoimmune encephalitis.
Sequential ochratoxin A and citrinin values documented during the medical evaluations of the boy in this case report.
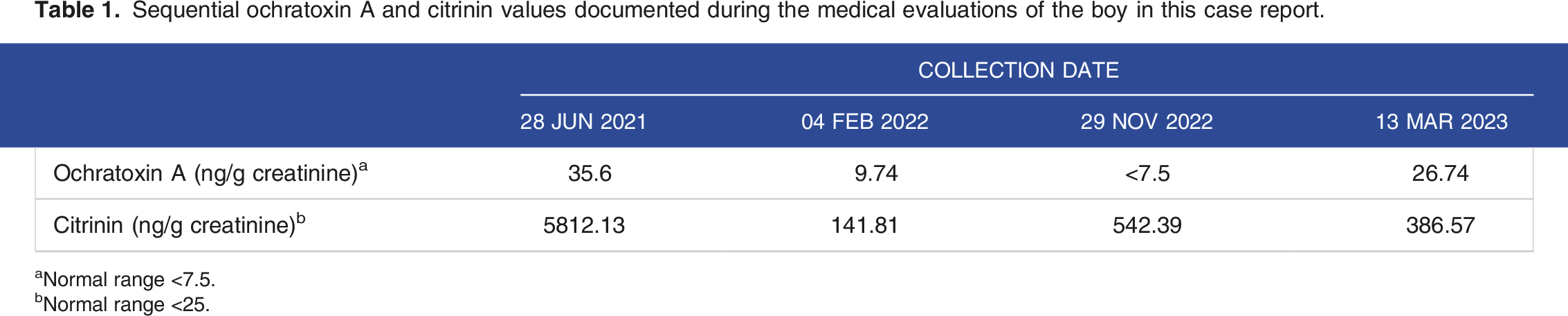
aNormal range <7.5.
bNormal range <25.
Summary of commercial infectious disease diagnostic testing performed in 2021, during the medical evaluations of the boy in this case report.

Bartonella serological and molecular test results for a child with progressive neurological abnormalities and seizures following a cat scratch.

aDenotes DNA extraction from enrichment blood BAPGM and Brugge blood cultures at incubation days 7, 14, and 21 or brain tissue cultures at 2, 5, 7, 9, 14, 16, 19, and 21 days.
NA = Not applicable.
<32, no seroreactivity to Bartonella spp. antigens at a 1:32 serum dilution.
Bh, Bartonella henselae; Bvb I, Bartonella vinsonii subsp. berkhoffii genotype I; Bvb II, Bartonella vinsonii subsp. berkhoffii genotype II; Bk, Bartonella koehlerae; Bq, Bartonella quintana.
qPCR, quantitative polymerase chain reaction.
ddPCR, digital polymerase chain reaction.
In June 2022, right cortical brain biopsies were obtained at Sick Kids Hospital, Toronto, Canada. Bacterial and fungal cultures were negative, as were PCR assays for MV, EBV, HHV6, Adenovirus Human herpesvirus 7, Mycoplasma and Chlamydophila pneumoniae. Sections of the right cerebral cortex, leptomeninges and white matter documented a preserved cortical laminar pattern, with no balloon cells or meganeurons. The grey-white junction was preserved but appeared focally pale. Glial fibrillary acid protein (GFAP) immunohistochemistry identified astrogliosis. Fresh brain biopsy tissue shipped overnight to the NCSU-IPRL was cultured in Brugge and BAPGM enrichment culture media. Bartonella henselae DNA (132/133bp, 99.2% homologous to B. henselae SA2 GenBank Accession # AF369529) was amplified and sequenced from 5-day BAPGM and 21-day Brugge brain tissue enrichment cultures. Using a B. henselae-specific probe, serial qPCR testing of DNA extracted from both enrichment cultures tested at 2, 5, 7, 9, 14, 16, 19, and 21 days was positive for both media at different time points.
Beginning January 2024, monthly intravenous immunoglobulin (IVIG, 1 g/kg) treatments have been administered through November 2024. Between June 2022 and June 2024, 2 post-surgery CT scans revealed no abnormalities, whereas routine and prolonged EEGs, an MRI, and PET scan all identified abnormalities consistent with previous analyses. Based upon the PET scan, the entire right hemisphere remained hypometabolic. By April 2024, seizures had decreased slightly in frequency and intensity, and the efficacy of his rescue medication (midazolam, 4 mg) increased, resulting in no ER admissions after January 24, 2024.
Babesia odocoilei and Babesia divergens-like MO-1 genus and species-specific DNA sequence results for a child with progressive neurological abnormalities and seizures following a cat scratch and presumed tick bite.

aIdentifies B. odocoilei or B. divergens sequences obtained using Babesia genus ITS primers.
bIdentifies B. odocoilei sequences obtained using B. odocoilei specific ITS primers.
cIdentifies B. divergens-like MO-1 sequences obtained using B. divergens specific ITS primers.
Discussion
Based upon an unusual sequence of events, a combination of cat scratch transmitted B. henselae infection at 2 years of age, presumably followed by tick transmission of B. odocoilei, and B. divergens-like MO-1 infection 18 months later, and mycotoxin exposure documented after seizure onset created a complex clinical scenario for this child, his parents, and his doctors. Initial Bartonella research testing in blood and enrichment blood cultures was negative; however, 6 months later brain biopsy tissue incubated in 2 enrichment culture growth media resulted in 16S-23S, ITS ddPCR positivity and DNA sequence confirmation of B. henselae SA2.17,18 It is possible that B. henselae gained access to the child’s brain following the right facial cat scratch in 2016, and infection persisted until microbiological confirmation in 2022. Because his sequential EEG and MEG results localized the seizure foci predominantly to the right hemisphere and serial MRI findings documented subtle right-sided pathological changes, bacterial access to the brain may have occurred due to retrograde axonal transport from a peripheral nerve, or alternatively, by traversing the blood-brain or blood-cerebrospinal fluid barriers.25,26 As the brain is historically considered an immune privileged site, 26 regardless of the route of infection to the brain, we hypothesize that the bacteria remained viable and were subsequently able to induce a persistent intracranial infection for at least 6 years in duration (2016-2022). Bartonella henselae bacteremia has been previously reported in patients with seizure disorders, including a 23-year-old woman who developed fatigue, headaches, memory loss, disorientation, insomnia, poor coordination, tremors, and infrequent petit mal seizures 1 year after a diagnosis of CSD. 27 During the subsequent 2 year-period, she experienced 2 grand mal seizures and was treated with gabapentin for epilepsy. Approximately 3 years after her CSD diagnosis and at multiple time points during her sequential medical evaluations, she remained B. henselae seroreactive and B. henselae (Houston I strain type) DNA was amplified from her blood, BAPGM enrichment blood cultures, an agar plate bacterial isolate, and a BAPGM enrichment cerebrospinal fluid culture. 27 In another case report, a young girl experienced a spectrum of neurological complaints including frequent headaches, visual and auditory hallucinations, anxiety, vision loss involving the lower left quadrant of both eyes, episodic bouts of generalized paralysis, facial palsy, chronic insomnia, seizures, dizziness, cognitive dysfunction, and memory loss. 28 Bartonella henselae DNA was PCR amplified and sequenced from the girl’s formalin-fixed paraffin embedded right parietal lobe tissue, surgically resected in 2000 at 11 years of age, and from a blood specimen collected in 2012, further supporting the potential for longstanding intravascular and CNS infection. These and other case reports emphasize the potential for chronic bloodborne, or central nervous system infection following a cat scratch, regardless of whether the classical symptoms of CSD (fever, lymphadenopathy) developed prior to seizure onset. Although CSD is most often a self-limiting infection, it is increasingly clear that a subset of patients develops neurobartonellosis, if they fail to immunologically eliminate B. henselae. Given the frequency of cat and other animal scratches that pose a potential risk for Bartonella spp. transmission, in conjunction with the long period between the scratch and the development of symptoms, it is critical to obtain a detailed history of animal and vector exposures for patients with unusual or unexplained neurological presentations. 12
Rasmussen’s encephalitis (RE) was the primary differential diagnosis in the boy in this case report. RE is a unilateral hemispheric encephalitis, most often accompanied by refractory focal epilepsy, hemiparesis, and progressive cognitive decline.29,30 RE is characterized by 3 stages: a prodromal stage, an acute stage and a residual stage. Although a cause for RE has not been definitively identified, immune-mediated activation by a viral or other foreign antigen has been proposed in the etiopathogenesis. 31 Based upon histopathology, brain tissues from RE patients contain multifocal areas of cortical inflammation, in particular perineuronal lymphocytic infiltration primarily involving CD8+ and CD4+ T cells and microglial activation.29-31 Surgical removal of the affected hemisphere is currently the recommended treatment. RE cases most often occur in children (90% of reported cases) with a median onset of disease in a previously healthy child occurring at 6 years of age. CSD, an infection caused by B. henselae, is also diagnosed most often in children who are scratched by a cat, and subsequently develop fever and lymphadenopathy. The spectrum of illness associated with atypical CSD or bartonellosis in children and adults is broad and includes seizures, encephalopathy, neuroretinitis, and peripheral neuropathy, as well as less common neurological presentations. 12 Because fever and lymphadenopathy did not accompany the cat scratch to this child’s face and due to the unilateral nature of his CNS pathology, RE became the primary differential diagnosis; however, histopathology and the slow neurological progression were not diagnostically consistent with RE. Whether and the extent to which infection with a Bartonella or Babesia spp. might contribute to the development of unilateral hemisphere pathology (RE) or a disease that mimics RE deserves future research consideration.
Tables 2 and 3 in this case emphasize the potential medical complexity when attempting to confirm a diagnosis of neurobartonellosis. Bartonella henselae IFA is not highly sensitive, which may be of particular importance in patients with long standing infections.13,14,23 In this case, 3 commercial laboratories and our research laboratory failed to detect antibodies to Bartonella henselae or seroreactivity to the other Bartonella spp. that were concurrently tested. The long incubation period prior to development of neurological symptoms, in conjunction with the lack of sensitivity of IFA testing, creates a diagnostic dilemma for patients, clinicians and diagnosticians. Although BAPGM enrichment blood culture has improved bacterial isolation or molecular detection of Bartonella spp. DNA, on a research basis we failed to amplify B. henselae DNA from blood (n = 3 samples), serum (n = 3 samples) and enrichment blood cultures tested at 7, 14, and 21 days (n = 9 samples), using both qPCR and ddPCR from the January 2022 triple draw blood specimens. Intermittent bacteremia, in conjunction with extremely low numbers of viable bacteria (below the limits of PCR amplification) in the blood at the time of culture, may have negated our ability to document B. henselae infection prior to obtaining the brain biopsy for PCR testing and enrichment culture in 2 media. In conjunction with suspected, persistent CNS infection, it is possible that B. henselae was also in the blood stream at an extremely low-level bacteremia in January 2022, based upon positive ddPCR blood and enrichment blood culture results from December 2022 and January 2023, respectively (Table 3).
Unexpectedly, based upon amplification of 18S rRNA gene and 2 Intergenic Transcribed Spacer regions (ITS1 and ITS2) DNA sequences, infection with 2 Babesia species, B. odocoilei or B. divergens-like MO-1 organisms, spanning an 18-month time interval, was confirmed from multiple time points and from blood and brain enrichment blood cultures from this boy. Human infection with B. divergens, B. divergens-like MO-1, B. microti and B. odocoilei have been reported previously in North America. 32 Unlike this patient, neurological complications reported in human patients most often occur in association with high parasitemia, co-morbidities and the hemolytic anemia that is expected with acute babesiosis. 33 Recently, in conjunction with research efforts to improve detection of Babesia spp. DNA in patient specimens, we reported B. odocoilei infection in 7 human patients from the USA and Mexico, all of whom listed a spectrum of non-specific, but predominantly neurological symptoms on a research study questionnaire. 23 Six of these individuals were co-infected with a Bartonella sp. 23 In that study, a cutaneous rash, very similar to the rash in this boy, was reported in a 2 and half-year-old girl from Oklahoma, who subsequently developed night sweats, knee pain, nightmares, and sleep apnea during the ensuing months. 23 The parents of both children suspected an insect bite, but did not observe an attached tick, and had never seen similar prior rashes, even with known mosquito bites. When and how the child in this report became infected with B. odocoilei and B. divergens-like MO-1 was impossible to confirm. Due to their young ages, it seems plausible that Babesia transmission occurred in Canada and Oklahoma during summer months, when the parents observed the rash on their child’s arm. It also seems plausible that infection with B. henselae, followed by infection with 1 or both Babesia spp. (coinfections) initiated the seizure activity 8 days after the rash was observed. Historically, in the United States of America and Canada, B. odocoilei infection has been documented most often in cervids (white tailed deer, elk, reindeer, moose, and caribou). 34 Ixodes scapularis is considered the primary vector for transmission of B. odocoilei. Babesia divergens-like MO-1 has been reported in immunocompromised patients from Arkansas, Kentucky, Michigan, Missouri, and Washington; however, to our knowledge co-infection with these 2 piroplasms has not been previously reported. 35 Babesia divergens-like MO-1 piroplasma has been identified in cottontail rabbits from Massachusetts, where Ixodes dentatus was the suspected tick vector. 36 Due to historical limitations associated with serological and molecular diagnostic testing modalities, it is possible that human co-infections with more than 1 Babesia spp. are more prevalent than previously reported.
Based upon mycotoxin test results, environmental mold neurotoxicity was potentially an ongoing contributing factor to the boy’s illness when his seizures became refractory in August 2022. The primary mycotoxin source was the mattress placed on the floor to protect the child against falls during seizures between 2019 and 2020. The unintended consequence of this decision created an additional level of complexity when attempting to assess the symptoms and other findings reported in this child. In addition to nephro- and immunotoxicity, acute and chronic exposure to ochratoxin A has potential toxic effects on the central nervous system, including the hippocampus.37,38 This mycotoxin was found in the child’s urine, however, its concentration in the brain was not assessed. As neurological and neurocognitive impairments have been reported in people exposed to mycotoxins, an additive or synergistic effect of mycotoxins with B. henselae, B. divergens-like MO-1, and B. odocoilei infections potentially complicated the child’s illness. 39 Based upon DNA sequencing results, we conclude that this child was co-infected with B. henselae, B. divergens-like MO-1, and B. odocoilei. Collectively, this case illustrates the diagnostic and medical complexities associated with occult vector borne infections and mycotoxin exposure for physicians, medical researchers, and patients.
Footnotes
Acknowledgements
We wish to acknowledge and thank the parents for their many contributions to this investigation, including providing medical records, blood, serum and brain biopsy specimens from their son, as well as pictures of the cat scratch lesions and suspected insect bite and rash. We also thank the many physicians who have and continue to provide care for this child. The authors thank Dr Charlotte Mao (pediatric infectious diseases) for helpful discussions of the manuscript content, and Chance Liedig, Charlotte Moore and Ana Cláudia Calchi for facilitating this investigation by assisting in sample acquisition and serological and molecular testing and GenBank accession submissions.
Author contributions
EBB coordinated communications with the family, the child’s physicians, and drafted the manuscript. RGM, CR and EK performed Bartonella and Babesia spp. microbiological and molecular testing, contributed to the interpretation of results, helped finalize the manuscript, and confirmed results reported in the manuscript. All authors reviewed the final manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: In conjunction with Dr. S. Sontakke and North Carolina State University, E. B. Breitschwerdt holds US Patent No. 7,115,385 Media and Methods for Cultivation of Microorganisms, which was issued on October 3rd, 2006. He is a co-founder, shareholder and Chief Scientific Officer for Galaxy Diagnostics, a company that provides advanced diagnostic testing for the detection of Bartonella spp. infections. Dr. Ricardo Maggi is a co-founder and the Chief Technical Officer for Galaxy Diagnostics Inc. All other authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported through donations to the Bartonella/Vector Borne Diseases Research Fund at the North Carolina State University College of Veterinary Medicine, through a grant from the Steven & Alexandra Cohen Foundation, and by the state of North Carolina. The funding agencies were not involved in the design or any aspect of the study.
Ethical statement
Informed consent
The child’s parents provided written permission for the inclusion of their son into this research study and the subsequent testing of his collected samples. Additionally, they provided written permission for the publication of the information reported in this case report, including any images referenced in the publication.