
Abstract
The epidemiology of neuroimmunological disorders in Africa remains poorly understood. Regional variation in diagnostics and provider knowledge has led to challenges in real-world application of diagnostic criteria. We conducted a cross-sectional survey of clinicians practicing in Africa to characterize the current state of clinical diagnostic resources and developed a clinician-driven prioritized action plan. 130 respondents from 24 out of 54 countries in Africa participated (44% national response rate). Most respondents specialized in neurology (n = 86, 66%) and practiced in an urban setting (n = 84, 65%). While all participating countries had access to a neurologist and ophthalmologist, only half had access to an in-country neuroimmunologist. Three-quarters of respondents had access to an MRI within a 25-kilometer radius with most reporting a maximum magnet strength of 1.5 Tesla (n = 46, 61%). The median cost for an MRI brain was 150 USD, and MRI spine was 160 USD. The most urgent action item selected to improve the timely diagnosis of neuroimmunological conditions was subsidizing the cost of MRI followed by increasing availability of MRI. There were notable gaps in availability of specialists and access to MRI to diagnose neuroimmunological conditions in Africa. Urgent action and regional collaborations focused on addressing MRI cost and availability are needed.
Plain Language Summary
We conducted a survey amongst clinicians practicing in Africa to understand the current state of neuroimmunology diagnostics, which includes availability of specialist doctors, MRI and special antibody blood tests. A total of 130 participants from 24 African countries participated in this electronic survey between March through April 2025. We found notable limitations, especially amongst respondents from low World Bank income countries, in availability of sub-specialists to diagnose neuroimmunological conditions, high-quality MRI, and antibody tests. Lowering cost of MRI was most frequently chosen as the most urgent action needed to improve timely diagnosis of neuroimmunological conditions in Africa.
Introduction
Despite the rise of non-communicable diseases in Africa, the epidemiology of neuroimmunological disorders, including demyelinating diseases (eg, multiple sclerosis [MS], neuromyelitis optica spectrum disorder [NMOSD], myelin oligodendrocyte antibody-related disease [MOGAD]) and non-demyelinating immune-mediated disorders (eg, autoimmune encephalitis [AE], neurosarcoidosis, neuro-rheumatologic disorders, central nervous system [CNS] vasculitis, etc.) remains poorly understood. A contemporary systematic review of MS in sub-Saharan Africa (SSA) found mainly case series, case reports and a few registry studies; the only epidemiological studies of MS were conducted in South Africa.1,2 In North Africa, where additional epidemiological studies have been conducted, MS prevalence was estimated between 3 to 14.9 per 100 000. 3 A systematic review of NMOSD in Africa found only retrospective data from ten countries, despite a global meta-analysis suggesting a higher incidence and prevalence of NMOSD amongst people of African descent compared with White ethnic groups.4-7 No epidemiological studies of MOGAD have been reported from Africa. With regards to non-demyelinating immune-mediated disorders, the published literature is limited to case reports and a few case series.8-12
While international diagnostic criteria have been established for MS, NMOSD and MOGAD, regional variability in requisite diagnostics has led to challenges in real-world application of these criteria.13-15 The third Atlas of MS outlined several global barriers to the diagnosis of MS, ranging from lack of awareness amongst the general public and healthcare providers to lack of diagnostic test availability. 16 A recent worldwide survey also found a gap in availability and affordability of diagnostic tests for NMOSD, especially in low- and middle-income countries. 17 While the aforementioned surveys include data from some African countries, an in-depth understanding of the status of diagnostics in Africa is necessary to identify barriers that may be unique to this setting.
This observational study conducted amongst clinicians practicing in Africa sought to characterize the current state of clinical resources for the diagnosis of neuroimmunological disorders, with a focus on demyelinating diseases, and subsequently develop a clinician-driven prioritized action plan to improve diagnosis of neuroimmunological disorders on the continent.
Methods
This cross-sectional study was conducted amongst clinician members of the African Committee for Treatment and Research In Multiple Sclerosis (AFRICTRIMS) and other African healthcare providers (mostly neurologists or those with an interest in neurology). Any self-identified healthcare provider who currently practices at least part-time in a country in Africa met the inclusion criteria. Those who previously practiced or did not practice in Africa were excluded. An anonymous electronic questionnaire was developed by MS specialists and African neurologists based on literature review18,19 and expert consensus, and assessed for content validity and clarity through expert review. To mitigate non-response bias and survey fatigue, only select questions were included in the main survey with the remainder in supplemental. The electronic survey was distributed via social media (WhatsApp) and email to clinician members of AFRICTRIMS between March to April 2025. Respondents answered questions about their role in the healthcare system, primary practice setting, patient population, and availability of health professionals and diagnostics. A summary of the questionnaire, including a main survey and optional supplemental survey, is included in Figure 1. (Full questionnaire is included in Supplemental Materials). Summary of Variables Collected by Standardized Questionnaires in Main and Supplemental Survey. For Additional Details, Please See Supplemental Section including Full Questionnaires
This study was exempt by the University of North Carolina at Chapel Hill Institutional Review Board. All study data were collected and managed using REDCap electronic data capture tools hosted at the University of North Carolina at Chapel Hill. REDCap (Research Electronic Data Capture) is a secure, web-based software platform designed to support data capture for research studies.20,21 Countries were stratified by 2024 World Bank income status into Upper-Middle Income [UMIC], Lower-Middle Income [LMIC] and Low-Income [LIC] categories. 22 Data reported in local currencies were converted to USD using the exchange rates on xe.com on April 16, 2025.
Statistical Analysis
Data are reported using descriptive statistics, including mean and standard deviation for normally distributed continuous variables, median and interquartile ranges for non-parametric continuous variables, and proportions for categorical variables. Where respondents from the same country entered discordant results about diagnostic test availability, a test was considered available in a given country if at least one respondent indicated in-country availability of that test. For other variables with responses from multiple respondents within a given country, responses were aggregated by country and reported as means or medians as appropriate. Listwise deletion was used to address missing data. For the clinician-derived action plan, participants used direct ranking to indicate urgency (1 = most, 8 = least) of an action item, and a mean score was calculated for each item.
Results
Respondent Characteristics
A total of 130 respondents from 24 out of 54 African countries participated (Figure 2). The highest proportion of respondents were from LMICs (n = 81, 62%) followed by LICs (n = 26, 20%), then UMICs (n = 23, 18%). Two-thirds of respondents were neurologists or neurology post-graduate trainees (Table 1). Most practiced in an urban area (n = 84, 65%) and described their primary clinical setting as a government or public clinic or hospital (n = 100, 78%). Map of Responding Countries by 2024 World Bank Income Group and Number of Respondents per country. Source: https://www.mapchart.net/africa.html Respondent Characteristics (n = 130) *Other respondent roles included ophthalmologist, obstetrician, nurse, nurse practitioner, pharmacist, physiotherapist, midwife.

Patient Population
Three-quarters of respondents noted that most patients with neuroimmunological conditions in their primary practice setting were of average or below average socioeconomic class for their country of practice (n = 92, 75%). In the past one year, more respondents had definitively diagnosed MS (n = 92, 71%) than NMOSD (n = 79, 61). Most had confirmed between one and five new cases of each diagnosis (MS: n = 73, 57%; NMOSD: n = 63, 50%). Most respondents who had definitively diagnosed more than five cases of both MS and NMOSD were from UMICs (n = 6, 26%) whereas none of the respondents from LICs had definitively diagnosed more than five cases of both MS and NMOSD. Most respondents had not confirmed a MOGAD diagnosis in the past year (n = 87, 69%). The proportion of respondents who diagnosed at least one confirmed case of MOGAD was higher among those who cared for pediatric patients (n = 12/28, 43%) compared to those who only cared for adult patients (n = 25/102, 24%). Most respondents indicated that the number of patients for whom they were unable to provide a definitive diagnosis due to diagnostic barriers in the past one year was higher than the number of definitive diagnoses they made; this was true for MS, NMOSD and MOGAD (Figure 3). Respondents reported most patients with neuroimmunological disorders were referred to them from general practitioners (32%) followed by ophthalmologists (27%) (Figure 4). Demyelinating Disorders Diagnosed by Respondents in the Past One year. Source of Referrals for Patients With Suspected Neuroimmunological Disorders in the Past One Year

Access to Health Professionals
Availability of Specialized Health Professionals by Respondents per Country

Bolded values represent data per income group and overall. Percent values equal to 100 are omitted for countries with only one respondent for brevity. km = kilometer.
Access to MRI Diagnostics
Attributes of MRI Access by Respondents per Country

Bolded values represent data per income group and overall. Percent values equal to 100 are omitted for countries with only one respondent. MRI = Magnetic Resonance Imaging; T = Tesla; km = kilometer.
Antibody Diagnostics by Country
Availability and Type of Serum Antibody Testing for NMOSD and MOGAD by Country
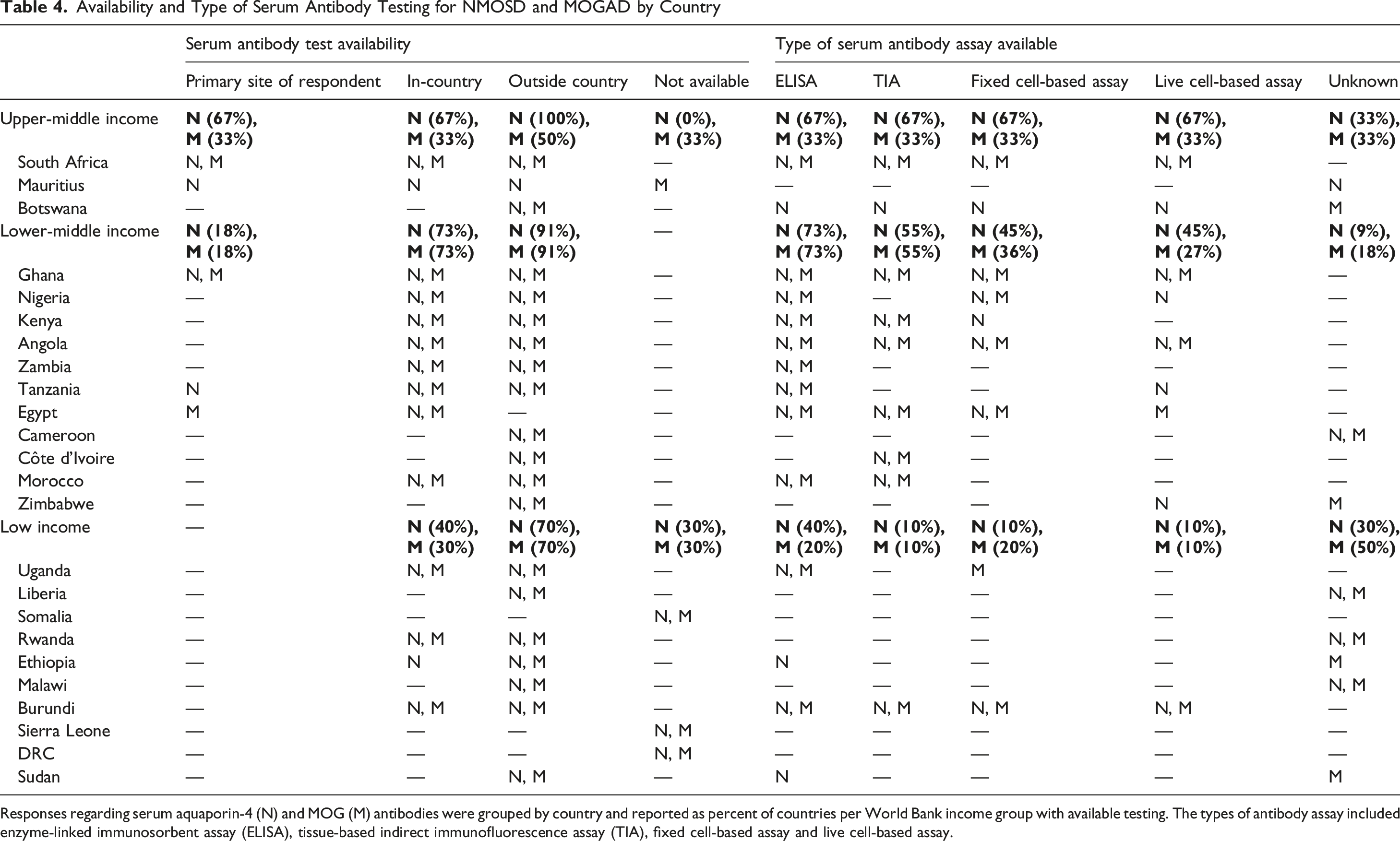
Responses regarding serum aquaporin-4 (N) and MOG (M) antibodies were grouped by country and reported as percent of countries per World Bank income group with available testing. The types of antibody assay included enzyme-linked immunosorbent assay (ELISA), tissue-based indirect immunofluorescence assay (TIA), fixed cell-based assay and live cell-based assay.
Diagnostic Costs and Insurance Coverage
Median Cost of MRI Brain and Spine by Country and World Bank Income Level

Bolded values represent data per income group and overall.
Insurance Coverage of MRI and Serum Antibody Tests by Respondents per Country

Bolded values represent data per income group and overall. As each respondent could select multiple options, percent values reported by type and level of coverage, not by country. Government = public, national or government-sponsored health insurance. No coverage = neither government nor private.
Prioritized Action Plan
The action item selected as most urgent to improve the timely diagnosis of neuroimmunological conditions in the respondent’s primary practice setting was subsidizing the cost of MRI (mean score = 2.8, SD 2.2) followed by increasing availability of MRI (mean score = 3.4, SD 2.2). Figure 5 outlines the ranking of the remaining action items. Ranked urgency of Action Items to Improve Timely Diagnosis of Neuroimmunological Disorders by Percent of Respondents (n = 90)
Supplemental Survey
Fewer participants (n = 25/130, 19%) completed the optional supplemental survey (Figure 1). These respondents were primarily neurologists (n = 23, 92%) representing half of countries that were included in the full survey (n = 12/24, 50%) and practicing in an urban area (n = 20, 80%) and government/public practice setting (n = 16, 64%). Most respondents (n = 16, 64%) indicated that more than half of patients with MS, NMOSD and/or MOGAD came for at least one follow-up appointment in the past one year. Respondents also reported that they had diagnosed the following neuroimmunological conditions within the past year: CNS systemic lupus erythematosus (n = 11, 44%), CNS vasculitis (n = 9, 36%), neurosarcoidosis (n = 7, 28%), stiff person syndrome (n = 7, 28%), anti-NMDA receptor encephalitis (n = 6, 24%), neuro-Sjogren’s (n = 6, 24%), and neuro-Behcet’s (n = 4, 16%). Respondents from five out of the 12 countries represented reported having an active patient registry for neuroimmunological disorders (Ghana, South Africa, Nigeria, Kenya, Burundi).
Most respondents indicated that the wait time to see a neurologist was less than three months (n = 22, 88%), and this did not differ between those practicing in a public vs private setting. Most respondents had access to a local, in-person radiologist (n = 21, 84%) with a median of 5.5 (IQR 3, 13). Few could access a neuro-radiologist either in-person (n = 12, 48%) or virtually (n = 3, 12%); nine respondents indicated no access to a neuroradiologist (n = 9, 36%). The most frequently available local allied health professional for neuroimmunological patients were physical therapists (n = 25, 100%), followed by dieticians (n = 20, 80%), speech therapists (n = 19, 76%), and psychologists (n = 19, 76%); only six respondents indicated having access to an MS nurse (n = 6, 24%). Most respondents (n = 16, 64%) reported that either none or less than half of their patients with neuroimmunological disorders typically obtain annual surveillance MRIs, primarily due to cost of MRI (n = 19, 76%) and lack of patient follow up in clinic (n = 10, 40%). Respondents from seven out of the 12 countries reported in-country availability of both CSF NMO and MOG IgG testing (n = 7, 58%), while those from four countries reported these CSF samples needed to be sent outside the country (n = 4, 33%). Very few respondents indicated that more than half of their patients with neuroimmunological disorders used government insurance to assist with MRI costs (n = 3, 12%). More respondents indicated that more than half of their patients used private insurance to assist with MRI costs (n = 7, 29%) as compared with government insurance (n = 3, 12%).
Discussion
We present data from clinicians providing care for patients with neuroimmunological disorders across the African continent to better understand the current access, availability and cost of diagnostics. Various global studies have focused on a specific disease entity or diagnostic test and noted disparities in availability and affordability of diagnostic tests for as well as in provider knowledge of MS and NMOSD.17,23 Regional survey studies from Latin America and Southeast Asia conducted amongst healthcare providers to understand availability and barriers of diagnostics similarly found gaps in availability of neurologists, neuroimmunology sub-specialists, availability of high-quality MRI and antibody tests for NMOSD and MOGAD.19,24 However, per our review of the literature, this is the first study to comprehensively report the current landscape of diagnostics for MS, NMOSD, and MOGAD in Africa. Our findings outline the challenges of diagnosis across different health systems within the continent and highlights clinicians’ perspectives on improving timely diagnosis.
Population of Patients with MS, NMOSD, and MOGAD
In the literature, the MS to NMOSD prevalence ratio varies between 30:1 in largely White cohorts to 2.6:1 in East Asian populations.5,23,25 In this study, slightly more respondents indicated they had definitively diagnosed more new cases of MS as compared to NMOSD in the past one year. Although this study was notably not designed to ascertain prevalence, the findings suggest an important incongruence. Global reports of low MS prevalence in sub-Saharan Africa as well as studies that support higher NMOSD prevalence amongst those of African ancestry have led to the prevailing belief among clinicians that NMOSD is more prevalent than MS in Africa.5,23 This difference between the prevalence ratio assumptions held by clinicians and this study’s findings may be due to several reasons, including that MS is truly more prevalent than NMOSD but underdiagnosed in Africa, or that NMOSD is underdiagnosed, misdiagnosed or faces a survivorship bias due to higher early mortality rates compared to MS in Africa. MOGAD was diagnosed more frequently by respondents who cared for pediatric patients compared to only adult patients, a finding which is supported by the literature that MOGAD is more common in children compared to other CNS demyelinating disorders.26,27 Furthermore, the number of suspected but unconfirmed diagnoses of demyelinating disorders due to patient-related, financial or systemic barriers to diagnostics was higher than definitive diagnoses across each disease entity in the past one year. While these findings are estimates by clinicians, do not reflect true population-based metrics and must be interpreted with caution, this underscores the concern for ascertainment bias in our current epidemiological understanding of neuroimmunological disorders across Africa due to resource limitations leading to underdiagnosis. Our study’s finding that respondents from UMICs diagnosed more cases of MS and NMOSD is supported by a global ecological survey that found MS prevalence correlated with a country’s healthcare expenditure per capita and density of neurologists and MRI units. 28 Referrals for suspected neuroimmunological patients were primarily from general practitioners, ophthalmologists, and clinical officers (who function similarly to physician assistants in many healthcare systems across Africa), a finding that is similar to a retrospective study conducted in Ireland. 29 Notably, general practitioners were the target audience for a recent virtual MS training course in Africa, and additional engagement of ophthalmologists and clinical officers in future sessions is needed. 30
Availability of Health Professionals
Availability of a neurologist or ophthalmologist locally was lowest in LICs. Data on workforce density from global studies support this finding, and, furthermore, indicate that sub-Saharan Africa has the lowest density of neurologists and ophthalmologists of any world region.31,32 While the absolute number of neurologists and ophthalmologists within African countries has increased over time, the distribution is mainly concentrated in urban areas, 33 which is underscored by most of this study’s respondents primarily practicing in an urban area. Taken together, these findings suggest that more rural areas within LICs have the least access to health professionals who can diagnose neuroimmunological disorders, and this may strongly influence estimates of prevalence. Interestingly, the reported wait time to see a neurologist was lowest in LICs, which may be explained by under-utilization of neurology services in LICs vs longer health system referral mechanisms in the other income groups. However, this needs to be further studied with a larger sample size.
While no previous studies have examined the availability of sub-specialized health professionals, specifically neuroimmunologists, neuro-radiologists and neuro-ophthalmologists, by country in Africa, the third Atlas of MS reported about 5% of all neurologists globally have subspecialty expertise in neuroimmunology. 34 When contextualized with the World Health Organization’s report of 0.03 neurologists per 100 000 in Africa, 31 this supports our study’s finding that sub-specialists are even more scarce. While a sub-specialist is not necessary to diagnose neuroimmunological disorders, referral to one may be useful for cases in which there is diagnostic uncertainty, especially for conditions that may not be commonly diagnosed by the practicing general neurologist. Furthermore, tele-neurology may be leveraged to bridge this gap in access to sub-specialist evaluation and follow up for patients with suspected or confirmed neuroimmunological conditions.35-37 Notably, there was variation in reported availability of an in-country neuroimmunologist from respondents in six countries, suggesting that provider awareness of sub-specialist availability is warranted and may be highlighted through regional groups such as the AFRICTRIMS network. However, as we could not confirm formal, standardized sub-specialist training for neuroimmunologists and neuro-ophthalmologist, these data may be over-estimates.
Availability and Cost of MRI
Availability of local referral for MRI and access to either a 1.5 or 3 Tesla MRI unit was lowest in LICs in our study. This corresponds with global studies of MRI unit density, which found that the lowest density of MRI units is in LICs and in the African region. 38 Studies assessing MRI access within and across health systems in Africa noted that MRI units were concentrated within urban areas, more dominant in the private sector, typically of 1.5 Tesla strength, and clinically under-utilized; additionally, a non-negligible portion of them were not operational, a finding that was also noted amongst LICs in our study.39-41 Given the significant role of MRI in diagnosis of neuroimmunological disorders and the superiority of 3 Tesla MRI in visualizing smaller lesions, especially in the spinal cord, limited access to high-quality MRI constitutes a notable barrier to diagnosis in the region.13-15,42 Additionally, MS carries the highest risk of developing asymptomatic lesions compared with NMOSD and MOGAD and silent MS lesions predict higher risk of clinical relapse; as such, surveillance MRI is routinely recommended for MS, but it is not as important for NMOSD or MOGAD.43-45 After diagnosis, optimal disease monitoring differs between the three disorders and this carries important implications for strategies that must be employed depending on the specific disorder. Regarding delay to MRI, surprisingly, respondents from LICs reported the shortest time from MRI ordered to clinician review; this may be due to a selection bias in participants of higher socioeconomic strata who are able to afford MRI in LICs, under-utilization of available MRI units in LICs, shorter wait times for follow-up appointments, or variations in MRI scheduling within health systems in non-LICs. Insurance coverage for MRI, which was lowest amongst LICs, represents an important cost-related barrier to care and carries implications for both diagnostics and disease management. A large survey conducted amongst patients with MS in Latin America found that those with private insurance had greater access to imaging and appropriate delivery of disease-modifying treatments. 18 A dedicated, regional study amongst patients with MS, NMOSD and MOGAD across Africa may better underscore the role of insurance coverage in time to diagnosis and delivery of treatment, and these data could bolster the levels of advocacy and stakeholder interest on a national and regional scale.
Median cost of MRI in this study was similar to but slightly lower than the average of 200 USD reported by a recent needs assessment survey of radiologists in Africa. 41 Costs of MRI reported by those practicing in a private setting were higher than those in a government setting, likely reflecting a combination of differences in socioeconomic status of patients, level of subsidization, and costs of MRI operation and maintenance by practice setting. Interestingly, median costs did not clearly correlate with World Bank income status as the cost of MRI brain was slightly higher in LICs than LMICs. As this study was not specifically designed to detect true differences in MRI costs and there were broad ranges reported even within countries, dedicated comparative cost analyses of MRI across income strata within Africa are needed to further explore the validity, reproducibility and causal factors of this finding.
Availability and Cost of Antibody Testing for NMOSD and MOGAD
Respondents from only three of 24 countries reported having no access to serum aquaporin-4 and anti-MOG antibody tests. A 2019 study that used convenience sampling to outline the limited global availability of antibody testing found that about half of responding African countries did not have access to either antibody test. 17 The difference may be attributed to recent improvements in ability to perform antibody tests either in-country, the inclusion of shipping samples outside the country, or the use of multiple respondents per country in our study to capture more variation within countries as compared to convenience sampling. Variation in reported availability by respondents from within the same country also represents an important gap in provider knowledge of availability of testing within countries and, as such, these data may be used to improve awareness for providers. A broader knowledge gap is also likely, as most respondents did not find antibody testing to be urgent in improving diagnostics (Figure 5), even though there is clearly insufficient availability of antibody testing in many countries. This discrepancy represents an important target for educational efforts as a perceived lack of urgency may pose a barrier to future efforts to increase availability of testing.
Cost of antibody testing for serum aquaporin-4 was lower than the median reported cost in a prior global survey of NMOSD, likely because the antibody testing cost within Africa is truly lower than the global median due to laboratory or personnel costs and possible subsidization. 17 ELISA was the most frequently available assay to test for both NMOSD and MOGAD but is known to have a low sensitivity. In particular, ELISA is especially not recommended for anti-MOG antibody testing, which may explain why most respondents had not definitively diagnosed MOGAD in the past year.46,47 Only a few countries reported access to the gold-standard cell-based assay. 48 This limited access to serum antibody testing in several countries also draws attention to an important need for low-cost diagnostics, such as point-of-care dried blood sport testing, which may improve clinicians’ ability to accurately and quickly diagnose neuroimmunological disorders in resource-limited settings. Dried blood spot testing has recently been shown to be feasible for aquaporin-4 antibody detection, so programs are urgently needed to expand access to this test in lower resourced settings globally, especially in Africa.49,50 Given the lack of access to MOG antibody testing, particularly non-ELISA assays, development of similar systems for MOG antibodies are also urgently needed. Lastly, because quality management systems for medical laboratories across Africa are growing, this may be an important existing infrastructure within many African countries to expand high-quality, standardized antibody testing for neuroimmunological conditions. 51
Respondents from several countries that had access to the antibody tests reported that they were not aware of the assay type; this represents an important knowledge gap amongst providers taking care of this patient population since assay type may influence interpretation of tests results, clinical decision-making and estimates of disease prevalence. While a virtual MS training course was recently implemented in Africa, additional courses aimed at improving provider knowledge for diagnosing NMOSD and MOGAD are warranted. 30
Non-demyelinating Immune-Mediated Disorders
While data on non-demyelinating immune-mediated disorders, such as autoimmune encephalitis (AE) and neurosarcoidosis, was limited mainly to the supplemental survey completed by a smaller cohort of respondents, the findings suggest that these conditions are being diagnosed by clinicians in Africa and warrant being systematically studied through regional collaborations. Data on availability of antibody testing, especially for AE and other antibody-mediated conditions, was not specifically gathered in this study. However, a recent review of AE in Latin America noted concerns for underdiagnosis due to scarcity and cost of antibody testing, as well as the reliance on shipping samples to North America and Europe. 52
Prioritized Action Plan to Improve Timely Diagnosis
In synthesizing the current state of diagnostics to generate a clinician-driven prioritized action plan to improve rapid diagnosis, MRI cost and availability were the most frequently selected as most urgent by respondents. A global survey of barriers to MS diagnosis found that lack of awareness of MS symptoms amongst the public and health care professionals was the most commonly identified barrier to early diagnosis of MS, while lack of specialized medical equipment such as MRI was less frequently selected. 16 Since our study was conducted only amongst clinicians practicing in Africa, the prioritization of MRI cost and availability likely represents a more pressing barrier to this group and highlights the importance of regional data in identifying specific barriers to improve timely diagnoses.
Limitations
Our study has several limitations. While only 44% of African countries were represented, to our knowledge, this study is the most comprehensive report of neuroimmunology diagnostics in Africa to date. Selection bias may have influenced results as respondents were mainly clinicians with a special interest in neuroimmunology, had access to an electronic method of completing the survey, and had at least a basic level of English proficiency (mainly Anglophone countries were represented). While some countries had multiple respondents resulting in over-representation of their country’s data, others only had one respondent. Consequently, this may under-estimate variations and complexity reported in countries with low response rates. Compared to the overall distribution of World Bank income categories in Africa, LICs were underrepresented in this study, further suggesting that results are likely to be under-estimates. Additionally, the response rates for certain variables (such as cost of antibody tests) and the supplemental survey were significantly lower than for other survey variables and could be attributed to respondents either not knowing the requested information or to survey fatigue. As a result, variables with lower response rates over-represented data from urban, university-affiliated respondents and, as such, may be under-estimates of true costs. Data for most variables collected are also subject to recall bias. However, the selection of clinicians as the target population for this study allowed for a broad, efficient assessment of diagnostics that would not have been possible through other sampling methods. Lastly, due to the descriptive nature of this study, any causal associations cannot be directly made; however, these data may be hypothesis generating for future studies.
Conclusions
The survey of the current state of neuroimmunology diagnostics in Africa highlights gaps in access to specialists and diagnostic tests that will benefit from multisectoral advocacy to improve access to diagnostics in parallel with educational interventions to increase knowledge of neuroimmunological disorders amongst neurology providers. Several countries without access to specific antibody tests are geographically proximal to countries with access, and this finding should be harnessed to develop regional collaborations to increase access to diagnostics and more timely diagnoses. Finally, the emphasis and urgency of improving availability and cost of MRI to diagnose neuroimmunological conditions in a timely manner represents the need for a coordinated task force to prioritize and implement solutions within this region.
Footnotes
Acknowledgements
The authors would like to thank the members of the African Committee for Treatment and Research In Multiple Sclerosis (AFRICTRIMS) for their participation.
Ethical Considerations
This study was exempt by the University of North Carolina at Chapel Hill Institutional Review Board.
Consent to Participate
Due to the anonymous nature of the online questionnaire, the requirement for informed consent was waived by the University of North Carolina at Chapel Hill Institutional Review Board. Nonetheless, a research information sheet outlining the study aims, benefits, risks, data security measures, and statement of voluntary participation was provided to each subject at the beginning of the online survey.
Author contributions
M. Sahu: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Software, Writing - original draft, Writing - review & editing.
M. Chomba: Methodology, Writing - review & editing.
F. Duodu: Methodology, Writing - review & editing.
M. Diaz: Methodology, Project administration, Writing - review & editing.
D. Sokhi: Methodology, Writing - review & editing.
D. Saylor: Conceptualization, Formal analysis, Methodology, Supervision, Writing - original draft, Writing - review & editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received funding from the NIH Fogarty International Center (K01TW011771, D43TW009340) and American Academy of Neurology/American Brain Foundation Neurodisparities Clinical Research Training Scholarship.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Anonymized data not published within this article will be made available by request from any qualified investigator that follows regulations regarding data sharing.