
Abstract
Introduction
Distal Medium Vessel Occlusions (DMVOs) represent a significant subset of Acute Ischemic Stroke (AIS), with unique treatment challenges due to vessel size and location. While Endovascular Therapy (EVT) shows promise, its efficacy compared to Best Medical Treatment (BMT) remains unclear.
Methods
PubMed, Cochrane Central, and ScienceDirect were searched from inception till May 2025. Categorical data were pooled as risk ratios (RRs) along with 95% Confidence intervals (CIs) using the Review Manager software. Quality was assessed using the Cochrane Risk of Bias tool and the Newcastle Ottawa Scale.
Results
Thirty-seven studies pooling a total of 9,505 patients were included in this meta-analysis. The excellent functional outcome (modified Rankin Scale (mRS) 0-1) was comparable between both the EVT and BMT arms (RR= 1.04; 95% CI: [0.96, 1.13]; p= 0.34; I2= 59%). Similarly, the functional independence (mRS 0-2) showed no significant difference between the two groups (RR= 1.00; 95% CI: [0.94, 1.06]; p= 0.99; I2= 64%). The 90-day mortality (RR= 1.21; 95% CI: [0.97, 1.52]; p= 0.09; I2= 46%) and neurological deterioration (RR= 1.39; 95% CI: [0.65, 2.95]; p= 0.40; I2= 82%) were also comparable between the two arms. EVT showed a statistically significant increase in early neurological improvement (RR= 1.38; 95% CI: [1.05, 1.82]; p= 0.02; I2= 53%) although it was associated with a high risk of symptomatic intracranial hemorrhage (sICH) (RR= 1.56; 95% CI: [1.15, 2.13]; p= 0.005; I2= 39%).
Conclusion
EVT was associated with a significant increase in the early neurological improvement, although the risk of sICH was high in it. Other safety and efficacy outcomes were comparable. Further high-powered randomized trials are needed to confirm these findings.
Keywords
Introduction
Acute Ischemic Stroke (AIS) ranks as a primary source of chronic disability among adults and is the second most common cause of death worldwide. 1 Endovascular therapy (EVT) has been recognized as the gold-standard treatment for patients with Large Vessel Occlusion (LVO), encompassing the Internal Carotid Artery (ICA), the first segment of the middle cerebral artery (MCA) (M1), and the Basilar artery. The robustness of this approach has been corroborated by multiple randomized controlled trials and meta-analyses over time.2-7 However, an alarming count of patients presents with occlusions in medium and distal cerebral vessels, such as the anterior cerebral artery (ACA), M2–M4 segments of the MCA, posterior cerebral artery (PCA), posterior inferior cerebellar artery (PICA), anterior inferior cerebellar artery (AICA), and superior cerebellar artery (SCA) (5). Distal Medium Vessel Occlusions (DMVOs) are a subset of AIS and account for a substantial percentage of ischemic strokes, ranging from 25% to 40%. 8 These occlusion sites pose distinctive challenges owing to the narrower diameter, heightened tortuosity, and peripheral placement of the vessels, obscuring thrombectomy procedures and elevating the chance of complications, such as vessel perforation and distal embolization. 9
Conventionally, Best Medical Treatment (BMT), comprising antiplatelets, anticoagulants, and supportive care, has served as the standard of care for DMVOs, although this approach has yielded less favorable outcomes. 10 While EVT is well-established for LVOs, its use in DMVOs remains unclear. Recent advancements in thrombectomy devices, like low-profile stent retrievers and distal aspiration catheters, have made EVT more viable for distal occlusions. Studies by Sun et al. and Anadani et al. have demonstrated that EVT for distal occlusions is relatively achievable, offering beneficial clinical outcomes.11,12 However, inconsistent patient selection, occlusion locations, and device choices have led to variable results, underscoring the need for further evidence to establish EVT’s role in DMVO treatment. A meta-analysis by Loh et al. (2023) discovered that EVT for DMVO can lead to favorable functional outcomes and minimal complication rates, supporting this approach as a feasible treatment option. 13 Conversely, Wang et al. (2025) found no clinical superiority of EVT over BMT in major outcomes. 14 This discrepancy highlights the potential risks of EVT and reinforces the continuing uncertainty regarding its role in treating DMVO.
Hence, our study aimed to provide an updated meta-analysis comparing EVT and BMT in DMVO-related AIS. This meta-analysis utilized recent clinical data, building upon the work of Wang et al., 14 which included recently published high-quality trials15,16 and rigorous methods to address gaps in the literature. This approach explored the evolving procedural strategy for DMVO.
Methods
This meta-analysis was conducted according to the guidelines laid down by the Preferred Reporting of Items in Systematic Review and Meta Analysis [PRISMA] guidelines 17 and followed the Cochrane Handbook for Systematic Reviews of Interventions. 18 This review’s protocol was registered on PROSPERO under the ID: CRD420251088113.
Search Strategy
A search was conducted across PubMed, Cochrane Central, and ScienceDirect from inception through May 2025. A robust search strategy was formulated with the use of relevant keywords, which comprised, but were not limited to, “Endovascular Thrombectomy”, “Distal, Medium Vessel Occlusions”, and “Ischemic Stroke”, in combination with Boolean operators such as “OR” and “AND”. The detailed search strategies used for each of the above databases are listed in Supplemental Table 1.
Study Selection and Eligibility Criteria
All the articles retrieved in our search were imported into EndNote version 20.5, and any duplicates found were removed. Two authors (B.S. and Z.U.A.) independently assessed the articles based on their titles and abstracts during the primary screening process. During secondary screening, the full texts of the articles identified in primary screening are assessed against a predetermined eligibility criterion. Any conflicts during the screening process were resolved by discussion through a third author (M.H.W.).
Inclusion criteria consisted of Randomized Controlled Trials (RCTs) and observational studies, which comprised adult patients > 18 years with AIS caused by DMVO (occlusion at ACA, MCA M2-M4 segment, PCA, PICA, AICA, and SCA); Intervention groups consisted of EVT therapy, which included mechanical thrombectomy (MT), intra-arterial thrombolysis, or bridging therapy. Control groups consisted of BMT patients receiving either conservative treatment or intravenous thrombolysis alone.
Data Extraction
Two independent authors (Z.U.A. and M.A.) performed data extraction from the eligible studies into an Excel sheet. Extracted baseline characteristics comprised: Author name, year of study, location, data collection period, study design, sample size, occlusion site, arms compared, mean age, sex, male%, NIHSS score on admission, and clinically relevant outcomes reported. Primary outcomes included excellent functional outcome and functional independence at 90 days. Secondary endpoints included symptomatic intracranial hemorrhage (sICH), 90-day mortality, early neurological improvement, and neurological deterioration.
Endpoints Definitions
The excellent functional outcome is defined as the modified Rankin Scale (mRS) score of 0-1, whereas the functional independence is determined by an mRS score of 0-2. sICH definitions used by the included studies are provided in the Supplemental Table 2.
Early neurological improvement is defined as a decrease of 4 or more points in the National Institutes of Health Stroke Scale (NIHSS) score, or a score of 0 on the earliest NIHSS after 24 hours but before discharge. Alternatively, neurological deterioration is defined as an increase in NIHSS score of ≥4 points 24 hours after admission.
Risk of Bias Assessment
The Cochrane Risk of Bias tool for randomized controlled trials (RoB 2.0) 19 was employed by two authors (E.Z. and H.K.) to evaluate the quality of the included RCTs, whereas the Newcastle-Ottawa Scale (NOS) 20 was used to evaluate the observational cohorts included. The studies were divided into the following quality categories based on the NOS: high (8-9 score), medium (5-7 score), and low (<5 score). RoB 2.0 is divided into five domains: (1) bias from the randomization process, (2) bias from deviations from planned interventions, (3) bias due to missing outcome data, (4) bias in outcome measurement, and (5) bias in selecting reported results. Meanwhile, the NOS evaluates studies based on three domains: selection, comparability, and outcome.
Statistical Analysis
Statistical Analysis was performed using Review Manager (RevMan) Version 5.4.1, and the data were presented as forest plots. Categorical data were pooled as risk ratios (RRs) with 95% confidence intervals (CIs) employing the Mantel-Haenszel random effects model. Subgrouping was performed based on occlusion sites, including the ACA, MCA M2-4, PCA, and the unspecified DMVO subgroup, in which the occlusion site in DMVO is not specified. Heterogeneity was evaluated using Higgins I2 statistics 21 and a p-value of <0.05 was deemed statistically significant. With outcomes showing heterogeneity >50%, we assessed the source of heterogeneity using leave-one-out sensitivity analysis. Publication bias was evaluated visually through funnel plots and statistically via Egger’s regression test. To determine the certainty of evidence, the GRADE assessment was done using the GRADEpro GDT. 22
Results
Study Selection
After an initial detailed search across PubMed, Cochrane Central, and ScienceDirect, a total of 4,321 articles were identified. After removing duplicates (n = 2,808), the remaining articles (n = 1,513) were passed through the primary title and abstract screening, thus yielding a total of 152 articles. These filtered articles were passed through the full-text secondary screening, yielding 37 articles15,16,23-57 which were included in the final quantitative synthesis. The study selection process is depicted in the PRISMA flowchart in Figure 1. PRISMA flowchart of the study selection process
Study and Patient Characteristics
The Baseline Characteristics of Included Studies

Note. All values are reported as Mean +− Standard deviation. * Median (Inter Quartile), **Median (Range).
A1, A2, A3 = A1, A2, A3 segment of the Anterior cerebral artery respectively; EVT: endovascular treatment; IV, intravenous; NIHSS: National Institutes of Health Stroke Scale; mRS: modified Rankin scale; M1 = M1 segment of the middle cerebral artery; M2 = M2 segment of the middle cerebral artery; M3=M3 segment of the middle cerebral artery; M4=M4 segment of the middle cerebral artery; sICH = symptomatic intracranial hemorrhage. P1=P1 segment of Posterior communicating artery, P2=P2 segment of Posterior communicating artery; P3=P3 segment of Posterior communicating artery; IVT: intravenous thrombolysis; MM: medical management; BMM: Best Medical Management; BMT: Best medical treatment; DMVO: distal and medium vessel occlusions; BT: bridging therapy; MT: Mechanical thrombectomy; ACA: Anterior cerebral artery; ENI: early neurologic improvement; eMT: early mechanical thrombectomy; rMT: rescue mechanical thrombectomy; RCT: Randomized controlled trial; END: Early neurological deterioration.
Outcomes
Summary of Meta-Analysis

Note. RR: Risk ratio; CI: Confidence interval.
Excellent Functional Outcome
Thirty-one studies comprising 8,832 patients (EVT: 3,872 vs BMT: 4,960) were included in the analysis of excellent functional outcome. Pooled analysis using a random-effects model showed no significant difference between EVT and BMT (RR = 1.04; 95% CI: [0.96,1.13]; p = 0.34). Heterogeneity was moderate (I2 = 59%) (Figure 2). Excellent functional outcome forest plot
Functional Independence
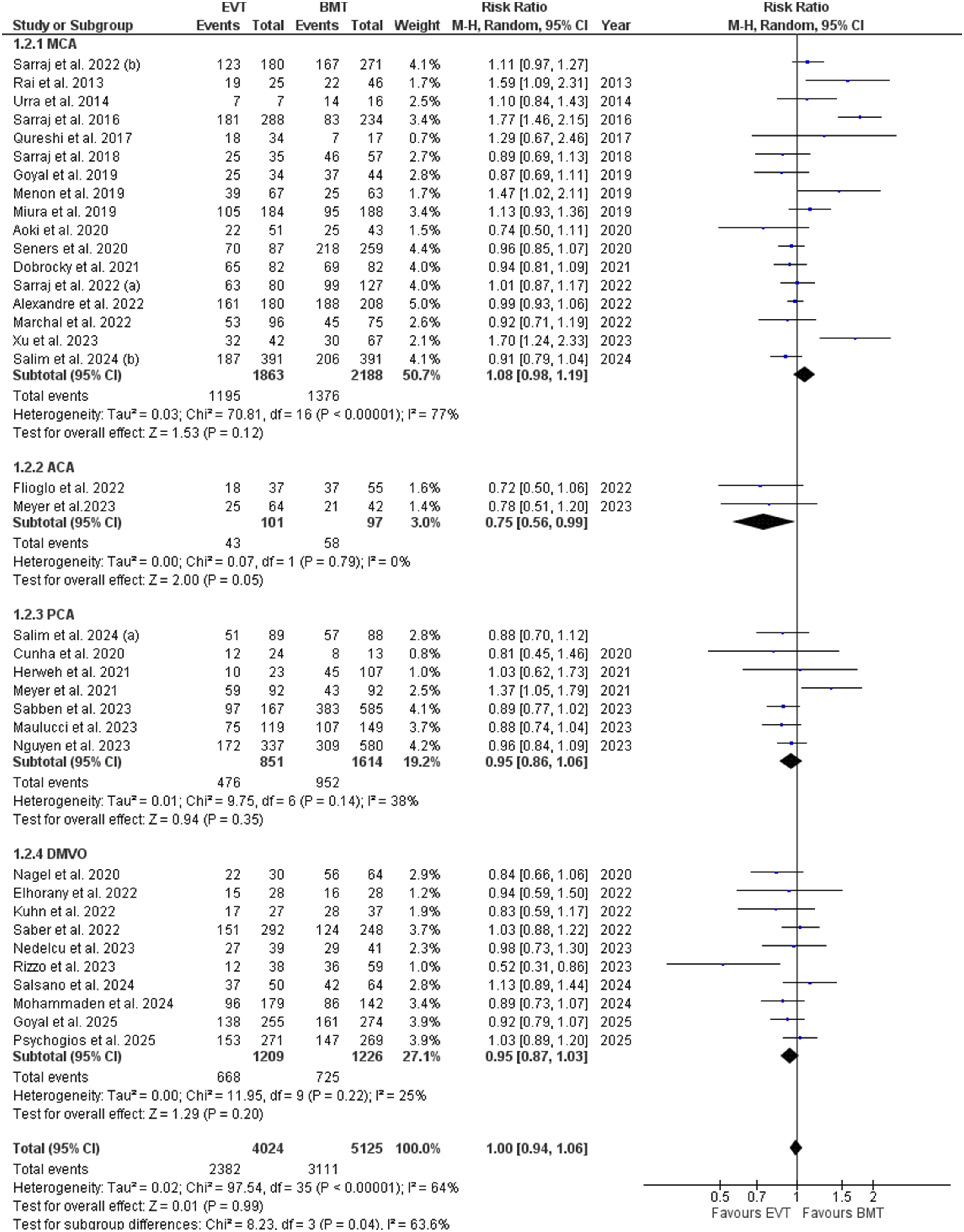
A total of 36 studies, including 9,149 patients (EVT: 4,024; BMT: 5,125), reported on functional independence. The pooled analysis demonstrated no statistically significant difference between EVT and BMT (RR = 1.00; 95% CI: [0.94-1.06]; p = 0.99). Moderate heterogeneity was observed (I2 = 64%) (Figure 3). Functional independence forest plot
Symptomatic Intracranial Hemorrhage
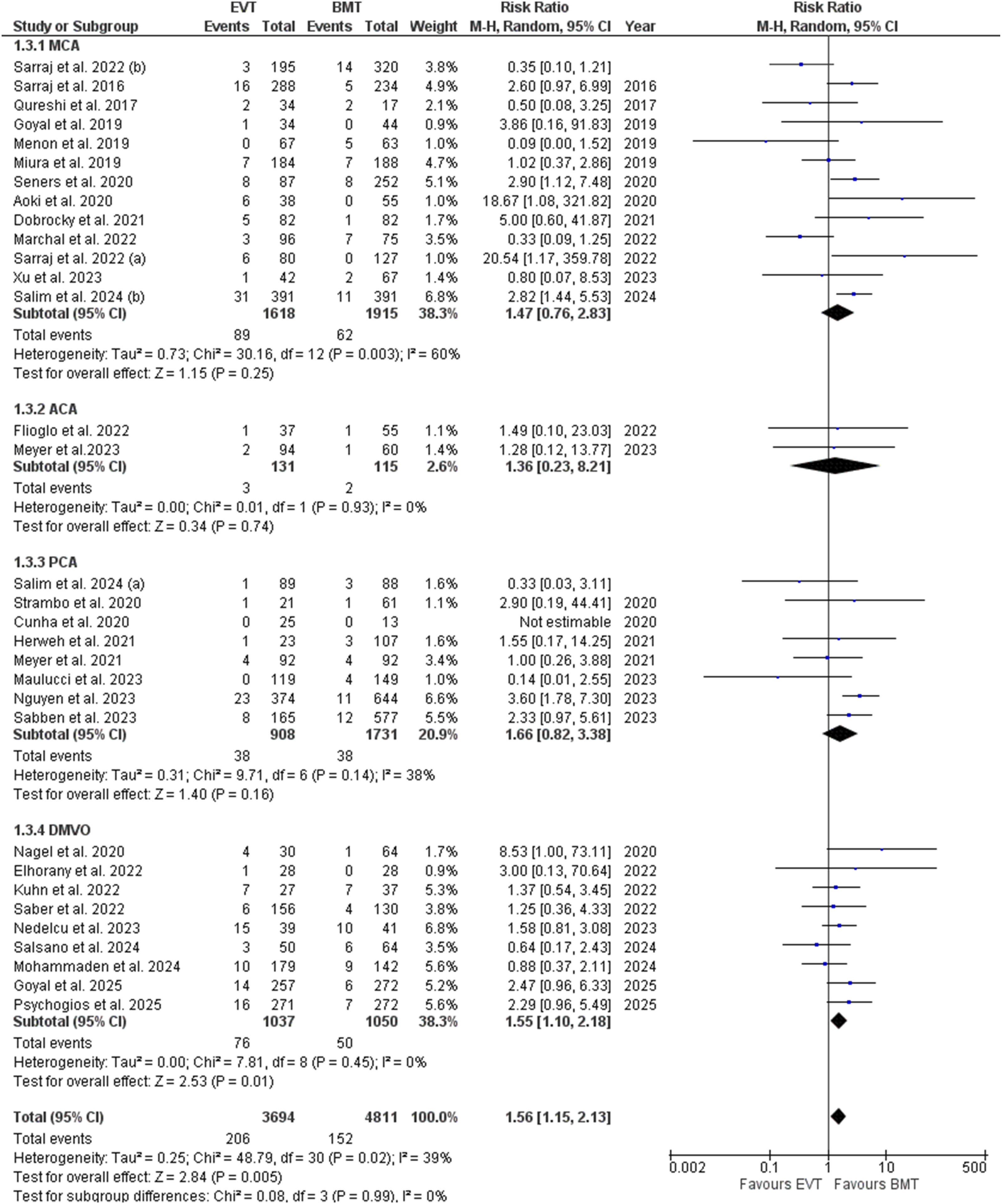
Thirty-one studies involving 8,505 patients (EVT: 3,694; BMT: 4,811) reported the incidence of sICH. EVT was associated with a significantly increased risk of sICH compared to BMT (RR = 1.56; 95% CI: [1.15, 2.13]; p = 0.005). Heterogeneity was moderate (I2 = 39%) (Figure 4). Symptomatic intracranial hemorrhage forest plot
90-Day Mortality
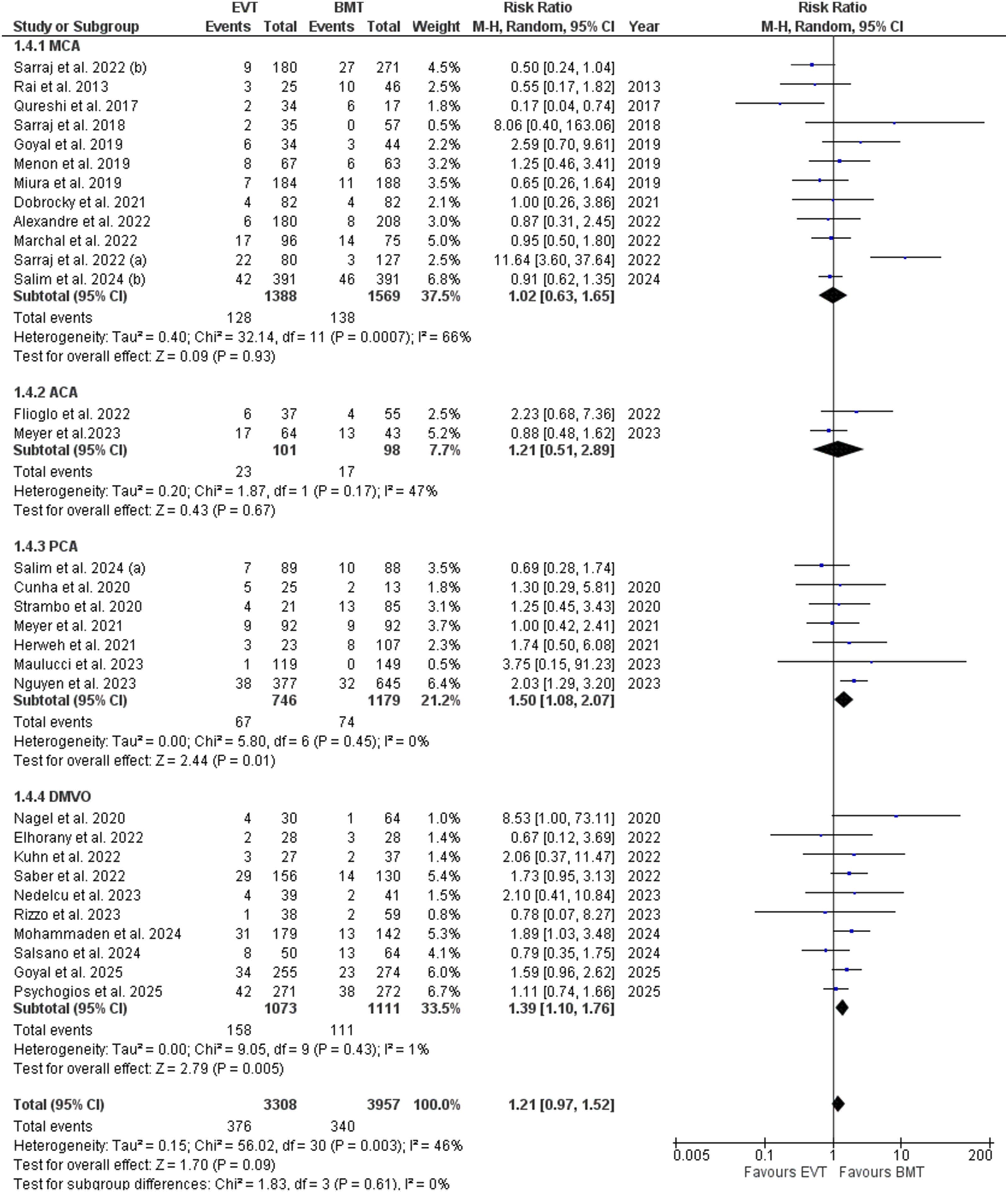
Mortality at 90 days was reported in 31 studies encompassing 7,265 patients (EVT: 3,308; BMT: 3,957). The pooled analysis revealed no significant difference in mortality between the two groups (RR = 1.21; 95% CI: [0.97, 1.52]; p = 0.09). Heterogeneity was moderate (I2 = 46 %) (Figure 5). 90 days mortality forest plot
Early Neurological Improvement
Seven studies involving 821 patients (EVT: 381; BMT: 440) assessed early neurological improvement. EVT was associated with a significantly higher likelihood of improvement compared to BMT (RR = 1.38; 95% CI: [1.05, 1.82]; p = 0.02). Heterogeneity was moderate (I2 = 53%) (Figure 6). Early neurological improvement forest plot
Neurological Deterioration
Six studies, including 2,035 patients (EVT: 778, BMT: 1,257), reported on neurological deterioration. The meta-analysis showed no significant difference between EVT and BMT (RR = 1.39; 95% CI: [0.65, 2.95]; p = 0.40). However, heterogeneity was substantial (I2 = 82%) (Supplemental Figure 1).
Subgroup Analysis Based on Occlusion Site
MCA
On the subgroup analysis based on the MCA M2-M4 occlusion sites, all the efficacy outcomes including the excellent functional outcome (p = 0.24), and functional independence (p = 0.12), and the safety outcomes including the sICH (p = 0.25), and 90 days mortality (p = 0.93), became statistically insignificant (Figures 7-10). Excellent functional outcome subgroup analysis based on the occlusion sites Functional independence subgroup analysis based on the occlusion sites Symptomatic intracranial hemorrhage subgroup analysis based on the occlusion sites 90 days mortality forest plot subgroup analysis based on the occlusion sites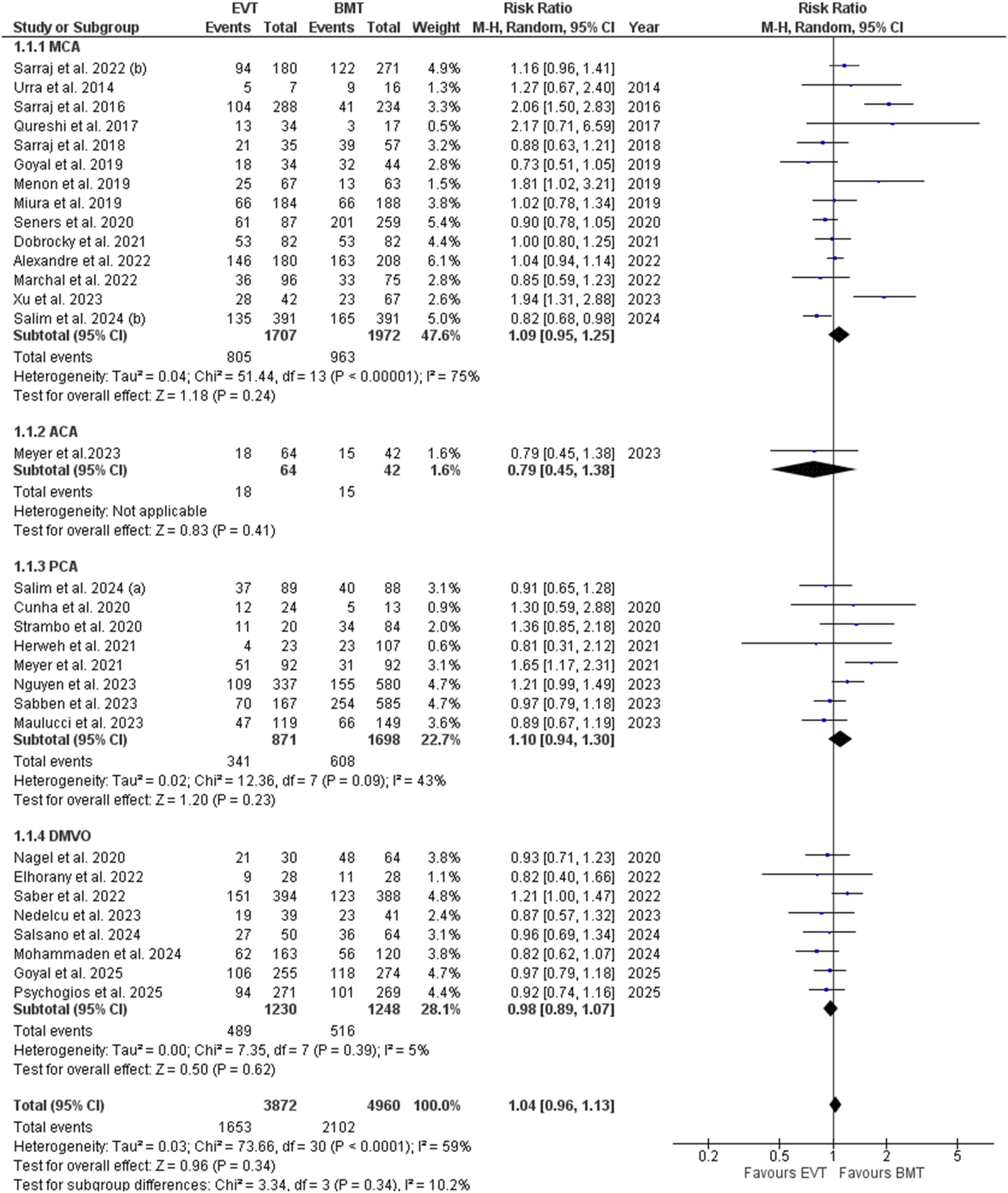
ACA
On subgrouping based on the ACA occlusion sites, the endpoints including excellent functional outcome (p = 0.41), sICH (p = 0.74), and 90 days mortality (p = 0.67) became insignificant except for the functional independence which showed a statistically significant decrease in the EVT (RR= 0.75; 95% CI: [0.56, 0.99]; p= 0.05; I2= 0%) (Figures 7-10).
PCA
Subgrouping based on the PCA occlusion sites showed insignificant results regarding the excellent functional outcome (p = 0.23), functional independence (p = 0.35), and sICH (p = 0.16) whereas the mortality was significantly increased (RR= 1.50; 95% CI: [1.08, 2.07]; p= 0.01; I2= 0%) (Figures 7-10).
DMVO
Subgroup analysis based on the unspecified occlusion site in DMVO; showed no significant difference in excellent functional outcome (p = 0.62) and the functional independence (p = 0.20) whereas both the sICH (RR= 1.55; 95% CI: [1.10, 2.18 ]; p= 0.01; I2= 0%) and the 90 days mortality (RR= 1.39; 95% CI: [1.10, 1.76]; p= 0.005; I2= 1%) were significantly increased in the EVT (Figures 7-10).
Risk of Bias Assessment
Risk of bias for randomized studies was evaluated using the RoB 2.0 tool. 19 Four studies15,16,34,40 were assessed. All the studies exhibited some concerns in Domain 5 (selection of the reported result), whereas both Menon et al. and Qureshi et al. also showed some concerns in Domain 2 (deviations from the intended interventions), as shown in RoB 2.0 traffic light plot Supplemental Figure 2.
For non-randomized studies, quality was assessed using NOS. 20 All studies scored between 7 and 9, indicating high methodological quality. Most studies reported robust performance across the selection, comparability, and outcome assessment domains, as shown in Supplemental Table 3.
Sensitivity Analysis and Publication Bias
For outcomes having heterogeneity > 50% we performed a leave-one-out sensitivity analysis to investigate the cause of this heterogeneity. On removing the study by Sarraj et al. 2016, 47 the heterogeneity falls to 46% and 45% for the excellent functional outcome and functional independence, respectively (Supplemental Figures 3-4). Likewise, on removing the studies by Menon et al. 34 and Marchal et al., 32 the heterogeneity decreased to 41% and 39% for the outcome of early neurological improvement, respectively (Supplemental Figures 5-6).
Publication bias was assessed visually using funnel plots and statistically via Egger’s regression test. On visual inspection of funnel plots, no asymmetry was found, suggesting insignificant publication bias which was further confirmed using Egger’s regression test (Supplemental Figures 7-12) and Table 2.
GRADE Assessment
GRADE Summary of Findings Table

Note. CI: confidence interval; RR: risk ratio; a. The 95% confidence interval is crossing 1; b. The heterogeneity (I2) is more than 60%; DMVO: Distal and medium vessel occlusion; EVT: Endovascular thrombectomy; BMT: Best medical treatment; sICH : Symptomatic intracranial hemorrhage
Discussion
In this systematic review and meta-analysis of 37 studies comparing EVT with BMT in patients with DMVO, we assessed both efficacy and safety outcomes. The pooled analysis revealed no significant differences between EVT and BMT in achieving excellent functional outcome, functional independence, 90-day mortality, or rates of neurological deterioration. EVT was associated with significantly greater early neurological improvement compared to BMT; however, it also demonstrated a higher risk of sICH.
This meta-analysis sets itself apart from prior studies by using a larger sample size of 9,505 patients, compared to Wang et al.’s 14 6,826 patients and Loh et al.’s 13 2,469 patients. It also includes recent high-impact trials like ESCAPE-MeVO 15 and DISTAL, 16 which were not part of earlier analyses. Our findings regarding comparable excellent functional outcomes, functional independence, 90-day mortality, and rates of neurological deterioration, along with increased early neurological improvement and a higher risk of sICH, were consistent with those of Wang et al. 14 However, Loh et al. 13 reported a significant increase in functional independence in the EVT group. Moreover, we employed the GRADE assessment to evaluate the certainty of the evidence, which further enhances the methodology compared to previous reviews.
Current guidelines strongly endorse EVT for AIS due to proximal large-vessel occlusion (LVO). The 2018 AHA/ASA guidelines recommend MT with a stent retriever for patients with intracranial ICA or proximal MCA occlusions within 6 hours of onset. 58 European stroke guidelines similarly endorse EVT for LVO (including M2 MCA occlusions), but note that M3/ACA/PCA occlusions were underrepresented in trials and have uncertain benefit. 59 By contrast, EVT was not initially applied to DMVOs for several reasons. Early trials and subsequent meta-analyses largely excluded patients with small distal vessel occlusions, and those enrolled with M2, or more distal occlusions, represented only a small subset. Consequently, there was no robust randomized evidence to guide the use of EVT in this population. Additionally, the technical complexity of navigating smaller, tortuous distal vessels raised concerns about procedural safety, including risks of vessel injury, dissection, or perforation. 60 Furthermore, DMVO strokes often present with lower NIHSS scores and milder deficits, leading to a preference for intravenous thrombolysis (IVT) or conservative management. 60 Despite accounting for approximately 25 to 40% of all ischemic strokes, optimal treatment strategies for DMVO remain undefined.8,61 Recent advancements in low-profile thrombectomy devices and perfusion-based imaging have enhanced the feasibility and safety of EVT in this setting, and an increasing number of observational studies and RCTs are now evaluating its role in DMVO.
Our pooled analysis demonstrated that EVT did not confer a significant advantage over BMT in achieving either excellent functional outcome or functional independence at 90 days. Our findings build upon and expand upon previous meta-analyses by Loh et al. 13 and Wang et al. 14 Loh et al. 13 reported that EVT was associated with improved functional independence compared to BMT, only after statistical correction. Similarly, Wang et al. 14 found no significant overall difference in functional outcomes. However, both studies were limited by smaller sample sizes and lacked the most recent data. By incorporating a larger number of studies and more recent evidence, our analysis offers an updated and more comprehensive evaluation of EVT in DMVO. The recent ESCAPE-MeVO randomized trial similarly found no benefit of EVT on excellent functional outcome. 15 The trial investigators noted several factors that may have contributed to the lack of benefit, including longer workflow times, incomplete reperfusion in a substantial proportion of patients, and a higher incidence of sICH and other adverse events in the EVT group. Moreover, approximately 15% of EVT-assigned patients showed spontaneous recanalization prior to thrombectomy, often following IVT, further diluting any potential EVT effect. Consistent with these findings, data from large observational registries have similarly shown no significant differences in functional outcomes between EVT and BMT.23,57 The consistency of these results suggests that EVT does not clearly improve functional outcomes in the overall population of patients with DMVO. Moderate heterogeneity was observed in these outcomes, possibly reflecting differences in baseline stroke severity (e.g., NIHSS score), affected vessel segments (e.g., dominant vs. non-dominant M2, PCA, ACA), and use of IVT. It is plausible that EVT offers benefit in specific subgroups (e.g., dominant M2 occlusions), which may be offset by neutral or even harmful effects in others. Wang et al. further explored this and reported that, for M2 segment MCA occlusions, EVT was associated with significantly higher odds of achieving excellent functional outcomes compared to BMT. 14 They also observed reduced functional independence in individuals with ACA occlusion, which aligns with the findings of our subgroup analysis. A pooled meta-analysis of EVT-treated ACA strokes found that approximately only 41% achieved 3-month functional independence, and roughly 20% died by 3 months. 62 These rates are substantially lower than those reported for proximal MCA strokes or other LVOs.
We observed no significant difference in rates of neurological deterioration between EVT and BMT. Early deterioration was generally uncommon in both groups across studies. This implies that EVT did not meaningfully prevent early worsening any more than medical therapy. Prior literature on DMVO has not emphasized neurological decline, but available data are consistent with our findings. A post-hoc analysis of the HERMES study found that the incidence of unexplained early neurological deterioration (UnEND) was similar between the EVT and medical management arms, and patient-related factors did not increase the risk of UnEND with EVT compared to medical management. 63 This is broadly consistent with non-DMVO stroke data, where early NIHSS fluctuations often depend on infarct growth and edema, factors not entirely prevented by EVT. 64 We also observed significant heterogeneity in the pooled analysis of neurological deterioration, suggesting variability in outcome definitions, assessment time points, or patient selection across studies, which may limit the generalizability of this finding. However, while EVT did not appear to reduce early neurological deterioration, our analysis revealed a significant advantage in terms of early neurological improvement. This effect was consistently observed across studies and was statistically significant in our pooled estimates. Among the included studies, Marchal et al. (2022), which contributed the highest weight to our analysis, reported a greater improvement in NIHSS scores at discharge among EVT-treated patients compared to those who received medical management alone. 32 This finding is biologically plausible, as successful recanalization in smaller, distal vessels can promptly restore perfusion to penumbral tissue, leading to rapid clinical improvement. Similar associations between early reperfusion and neurological recovery have been well established in the context of proximal LVOs. 65 Nonetheless, the observed early improvement did not translate into superior long-term functional outcomes. This discrepancy may be attributable to the relatively small infarct volumes typically associated with DMVO, where early symptom resolution may have limited impact on eventual disability or independence. Alternatively, the higher rate of sICH and other complications with EVT might negate the early gains by 90 days.
Our analysis found a significantly higher rate of sICH in the EVT group, consistent with the previous meta-analysis. 14 This elevated risk may reflect the inherent procedural challenges of thrombectomy in smaller, more fragile distal vessels, which are prone to injury during catheter navigation or device deployment. Moreover, patients with DMVO often have lower baseline NIHSS scores and smaller infarct cores, potentially reducing the margin of benefit from EVT and increasing the relative impact of procedure-related complications.66,67 Loh et al. also observed a numerical increase in sICH with EVT, though it did not reach statistical significance in their smaller sample. 13 Notably, a meta-analysis by Chen et al. focusing on EVT in large LVO among patients with mild stroke also found a higher incidence of sICH in the EVT group compared to those treated with medical management, suggesting that lower stroke severity may be associated with a less favorable risk-benefit profile for EVT. 68 Taken together, the available evidence indicates that EVT for DMVO does increase the risk of symptomatic bleeding, and this risk should be carefully weighed against the uncertain clinical benefit.
Our subgroup analysis of the MCA, including M2, M3, and M4 occlusion sites, found no significant differences in efficacy or safety between EVT and BMT. It’s important to note that these results apply to a broad grouping of MCA occlusions rather than isolated M2 occlusions, where EVT might show benefits due to larger vessel size and favorable anatomy. However, the absence of significant benefits across the overall MCA subgroups highlights the need for more detailed analysis of specific vessel segments to identify which MCA occlusion patients truly benefit from EVT. Additionally, the increased mortality seen in the EVT group within the PCA subgroup suggests that EVT may not be suitable for this patient population. A multicenter cohort of 752 patients with isolated PCA occlusion found that EVT doubled the risk of sICH and early neurological deterioration. 42 They concluded that EVT should not be routinely recommended for PCA strokes outside trials. Similarly, a pooled meta-analysis of 7 studies reported no difference in functional outcomes for isolated PCA occlusions but a significantly higher mortality in the EVT arm. 69 The evidence consistently shows that EVT for isolated PCA occlusions appears less beneficial and potentially harmful. Additional high-quality randomized trials focused on specific occlusion sites are needed to verify these results and identify which patients with specific occlusion locations are likely to benefit from EVT treatment.
Lastly, we found no significant difference in 90-day all-cause mortality between patients with DMVO stroke treated with EVT versus BMT, a result consistent with earlier analyses.13,14 The available data do not indicate a clear mortality benefit of EVT over BMT in this patient population, emphasizing the need for larger prospective randomized trials to assess the impact of EVT on survival definitively. In contrast, EVT has been shown to reduce mortality in patients with LVO stroke. A systematic review of 18 trials reported significantly lower 90-day mortality with EVT compared to BMT. 70 However, a more recent meta-analysis of 22 studies found a higher risk of 90-day mortality with EVT, suggesting that outcomes may vary based on patient selection, timing, and complication rates. 71 Given that DMVO strokes generally carry a lower baseline risk of death than LVO strokes, any intervention must be exceptionally safe to confer a mortality benefit. Our findings suggest that neither EVT nor BMT alone improves survival in DMVO, possibly due to a balance between potential life-saving reperfusion benefits and the procedural or hemorrhagic risks associated with thrombectomy. Notably, even in LVO stroke, the mortality benefits from EVT have been modest, making the neutral result in DMVO a consistent and expected extension of current evidence.
The observed findings indicate that although EVT may lead to early neurological improvement, these do not necessarily translate into long-term functional benefits. Clinicians should carefully weigh the potential for early recovery against the higher risk of sICH associated with EVT. Given the high heterogeneity and low certainty of current evidence, further high-quality randomized trials are essential to confirm the long-term advantages and risks of EVT for patients with AIS caused by DMVO before it can be broadly recommended for this group.
Limitations
This meta-analysis has certain limitations. First, the analysis was conducted at the study level rather than using individual patient data, limiting the ability to adjust for patient-level confounders. Secondly, many included studies were observational registries or non-randomized cohorts, which are prone to selection bias and residual confounding. For instance, patients selected for EVT often had more severe strokes or showed early deterioration under medical care. In contrast, those who did well with IVT alone were not taken for intervention. Such confounding can affect the apparent treatment effect sizes. Additionally, there was variability in treatment protocols, including intervention time windows, use of bridging IVT, imaging selection criteria (such as non-contrast CT and CTA versus perfusion imaging), thrombectomy techniques (device type, number of passes, adjunctive intra-arterial therapy), vessel occlusion sites like ACA, MCA, and PCA in DMVO stroke, study designs including observational studies and RCTs, and initial stroke severity indicated by NIHSS scores, which may contribute to heterogeneity. Additionally, differences in how sICH is defined can lead to heterogeneity; hence, future research should aim to standardize these definitions to minimize variability. A key limitation of this study is the high heterogeneity and low certainty in some outcomes, which highlights uncertainty in the pooled estimates and limits their generalizability. These limitations emphasize the need for large-scale, prospective RCTs to more definitively establish the safety and efficacy of EVT in patients with DMVO.
Conclusion
This systematic review and meta-analysis found no significant differences between EVT and BMT in terms of excellent functional outcome, functional independence, 90-day mortality, or neurological deterioration in patients with DMVO. However, EVT was associated with greater early neurological improvement, suggesting potential early clinical benefits that did not translate into superior long-term outcomes. Notably, EVT was also linked to a higher risk of sICH. Subgroup analysis revealed no significant advantage of EVT in MCA occlusion, suggesting that EVT’s benefit in this subgroup remains uncertain. In contrast, it was associated with a higher risk of mortality in the PCA subgroup. However, due to high heterogeneity and low certainty evidence, current findings cannot definitively establish equivalence between EVT and BMT. Instead, they indicate ongoing uncertainty about the relative effects of these treatments. More randomized trials are needed to confirm these results and offer clearer insights.
Supplemental Material
Supplemental Material - Comparing the Efficacy and Safety of Endovascular Therapy versus Best Medical Treatment in Acute Ischemic Stroke Patients With Distal Medium Vessel Occlusion: A Systematic Review and Meta-Analysis
Supplemental Material for Comparing the Efficacy and Safety of Endovascular Therapy versus Best Medical Treatment in Acute Ischemic Stroke Patients With Distal Medium Vessel Occlusion: A Systematic Review and Meta-Analysis by Muhammad Hassan Waseem, Zain ul Abideen, Eeshal Zulfiqar, Barka Sajid, Aisha Kakakhail, Haider Kashif, Muhammad Ansab, Muhammad Wajih Ansari, Rowaid Ahmad, Zara Fahim, Pawan Kumar Thada, and Brandon Lucke-Wold in Journal of Central Nervous System Disease.
Footnotes
Author Contributions
Study concept and design: MHW and ZUA; acquisition of data: ZUA, BS, HK and MA; analysis and interpretation of data: ZUA, EZ, and AK; drafting of the manuscript: RA, ZF, MWA, and PKT; critical revision of the manuscript: MHW and BLW.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data will be made available upon reasonable request to the authors.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.