
Abstract
Antiseizure medications (ASMs) are the mainstay of symptomatic epilepsy treatment. The primary goal of pharmacotherapy with ASMs in epilepsy is to achieve complete seizure remission while minimizing therapy-related adverse events. Over the years, more ASMs have been introduced, with approximately 30 now in everyday use. With such a wide variety, much guidance is needed in choosing ASMs for initial therapy, subsequent replacement monotherapy, or adjunctive therapy. The specific ASMs are typically tailored by the patient’s related factors, including epilepsy syndrome, age, sex, comorbidities, and ASM characteristics, including the spectrum of efficacy, pharmacokinetic properties, safety, and tolerability. Weighing these key clinical variables requires experience and expertise that may be limited. Furthermore, with this approach, patients may endure multiple trials of ineffective treatments before the most appropriate ASM is found. A more reliable way to predict response to different ASMs is needed so that the most effective and tolerated ASM can be selected. Soon, alternative approaches, such as deep machine learning (ML), could aid the individualized selection of the first and subsequent ASMs. The recognition of epilepsy as a network disorder and the integration of personalized epilepsy networks in future ML platforms can also facilitate the prediction of ASM response. Augmenting the conventional approach with artificial intelligence (AI) opens the door to personalized pharmacotherapy in epilepsy. However, more work is needed before these models are ready for primetime clinical practice.
Keywords
Introduction
Epilepsy is one of the most common and disabling chronic neurological disorders, affecting over 50 million people worldwide. 1 The primary goal of pharmacotherapy with antiseizure medications (ASM) in epilepsy is to achieve complete seizure remission while minimizing therapy-related adverse drug reactions (ADRs). Seizure freedom can be achieved in up to 70% of patients with appropriately chosen and trialed ASMs. 2 However, seizure freedom is not achieved in the first ASM monotherapy trial in more than half of the patients who require ASM polytherapy. 3 Prevention and treatment of underlying comorbidities and reduction of morbidity and mortality associated with seizures, including sudden unexpected death in epilepsy (SUDEP), is also objective. Although these goals may not be practical for everyone, we do not want to settle for the status quo or good enough until all appropriate options are explored.
Currently, there are over 30 ASMs available in the United States for treating epilepsy. With such a wide variety, much guidance is needed in choosing ASMs for initial therapy, subsequent replacement monotherapy, or adjunctive therapy. Also, recommending the most appropriate ASM for an individual can be challenging, and weighing key clinical variables requires experience and expertise that may be limited. This review discusses the evolution of ASM therapy in clinical epilepsy. First, we discuss the crucial patient and medication-related factors influencing the selection of ASMs. Then, we highlight the future of ASM therapy, including the potential impact of Artificial Intelligence (AI) in aiding the selection of the most effective and tolerated ASM for the individual patient.
The current state
Most first-generation ASMs were introduced in the first half of the twentieth century through the early 1950s.
4
These drugs were primarily derived from barbiturates, including phenobarbital, phenytoin, primidone, and ethosuximide. The second generation ASMs introduced in the 1960s-1970s include carbamazepine, valproate, and the benzodiazepines, such as clobazam, clonazepam, and diazepam.
5
The 1980s heralded a third generation of ASMs with novel mechanisms of action that were target-based.
6
The Anticonvulsant Screening Program mainly spurred the development of the third-generation ASMs and has resulted in the introduction of over 20 ASMs.
5
Since 2018 alone, four novel ASMs, cannabidiol, everolimus, cenobamate, and fenfluramine, have been introduced. Cenobamate was Food and Drug Administration (FDA) approved in 2019 for the treatment of focal seizures, whereas fenfluramine was approved for Dravet-Syndrome (2020) and Lenox Gastaut syndrome (2022). The timeline for the introduction of ASMs is summarized in Figure 1. Introduction of currently available antiseizure medications to the market. The year of drug introduction refers to either Europe or the United States of America.
Currently, there is no set algorithm for selecting one ASM from the other—however, medication and patient characteristics are considered when selecting ASMs. Also, when adding or changing ASMs in a patient’s existing regimen, it is essential to discuss the risks and benefits of new medications before their initiation, including a frank discussion regarding boxed warnings and the most severe adverse effects, particularly those that can be life-threatening. Besides, patients should be given written instructions regarding adverse effects of concern for which they should seek emergency medical attention and those for which they should notify the prescriber.
Medication-related factors
Mechanism of action
Before prescribing an ASM, it is essential to understand the agent's putative mechanisms of action (MOA).7-9 Based on their molecular targets, ASMs can be categorized into drugs that act quite selectively via a single target (e.g., several of the sodium channel modulators) or act more broadly via multiple targets (e.g., valproate, topiramate, zonisamide, felbamate, cenobamate, cannabidiol).6,9,10 The MOA of most ASMs can be categorized into four broad classes: (1) modulation of voltage-gated sodium channels (e.g. phenytoin, carbamazepine, lamotrigine, lacosamide), voltage-gated calcium channels (e.g. ethosuximide), and voltage-gated potassium channels [e.g. retigabine (ezogabine)]; (2) enhancement of γ-Aminobutyric acid (GABA)-mediated inhibition through effects on GABA-A receptors (e.g. benzodiazepines, barbituates, striropentol), the GABA transporter-1 (e.g. tiagabine), or GABA transaminase (e.g vigabatrin); (3) inhibition of synaptic excitation mediated by ionotropic glutamate receptors, including N-methyl-D-aspartate (NMDA) [e.g, ketamine] and α-amino-3-hydroxy-5-methyl-4-isoxazole-propionate (AMPA) receptors (e.g. perampanel); and (4) direct modulation of synaptic release through effects on components of the release machinery, including synaptic vesicle glyocoprotein 2A (SV2A) [e.g. levetiracetam, brivaracetam] and the α2δ subunit of voltage-gated calcium channels (e.g. gabapentin, pregabalin).9,10 More recently, novel ASMs that act by unique MOA have been developed, including everolimus (inhibition of mTOR signaling in tuberus sclerosis),
11
fenfluramine (serotonergic 5-HT2 receptor agonist),
12
and cannadbidiol [Transient receptor potential vanilloid-1 (TRPV1), the orphan G protein-coupled receptor-55 (GPR55) and the equilibrative nucleoside transporter 1 (ENT-1).
13
The putative MOA of the commonly used ASMs is summarized in Figure 2. Putative mechanism of action of commonly prescribed antiseizure medications. AMPA: α-amino-3- hydroxy-5-methyl-4-isoxazolepropionic acid; GABA: γ-aminobutyric acid; NMDA N-methyl-D-aspartate; SV2A: synaptic vesicle protein 2A. Asterisks indicate that these compounds act by multiple mechanisms.8-10,14,16
Blockade of voltage-gated sodium channels is the most common mechanism of action among currently available ASMs. 8 ASMs that interact with voltage-gated sodium channels show a characteristic “use-dependent” blocking action so that they inhibit high-frequency trains of action potentials (as characteristically occurs with seizures) much more potently than they attenuate individual action potentials or firing at low frequencies.8,9 Phenytoin, carbamazepine, oxcarbazepine, and lamotrigine are considered “classical” sodium-channel-blocking ASMs since they inhibit high-frequency repetitive spike firing on the time scale of hundreds of milliseconds (“fast inactivation”).8,9 Lacosamide is also believed to induce its therapeutic effects by interacting with sodium channels. 9 However, unlike other sodium-channel-blocking ASMs, it inhibits spike firing in long trains of spikes on the time scale of 1-2 seconds. 14 It has been proposed that the very slow action of lacosamide is caused by an enhancement of a distinct and poorly understood form of inactivation, referred to as “slow inactivation”. 14
ASMs that act on GABA-A receptors as positive allosteric modulators include benzodiazepines, phenobarbital, and stiripentol. 9 Benzodiazepines such as diazepam, lorazepam, clobazam, and clonazepam are specific for synaptic GABA-A receptors containing the γ2 subunit and act to allosterically modulate these receptors to increase the channel-opening frequency, resulting in enhanced synaptic inhibition. 8 This confers a broad-spectrum antiseizure action. In contrast, barbiturates and stiripentol do not appear to increase the frequency of GABA-induced chloride channel opening but instead increase the channel open time.13,15 Because they are not specific for α3-containing GABA-A receptors, they are inactive in absence epilepsy and may even aggravate absence seizures. 16
When considering an add-on therapy for individuals who did not respond optimally to a single monotherapy, it is generally advisable to choose ASMs with different mechanisms of action. Such rational polypharmacy can increase efficacy and tolerability, even though no high-level evidence supports or refutes this approach. 3 Two medications showing a potentially favorable pharmacodynamic interaction are valproic acid and lamotrigine, the combination of which can be effective in controlling seizures unresponsive to either drug alone. 17 Some data suggest a favorable pharmacodynamic interaction between levetiracetam and lacosamide. 18
Spectrum of efficacy
The choice of antiseizure medication by the epilepsy type.
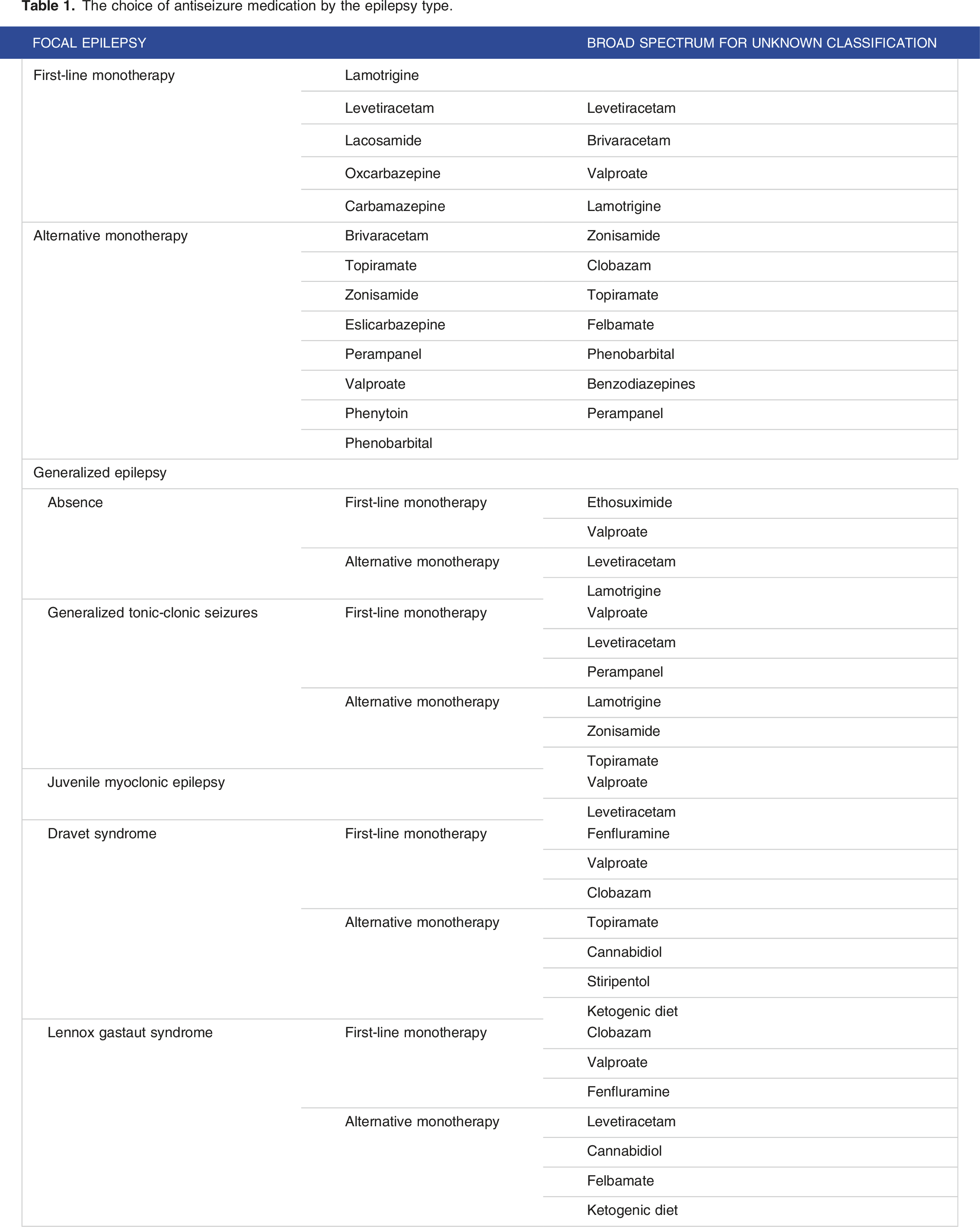
Clinicians should also be aware that improper selection of ASMs could result in ineffective treatment, pseudo worsening, or paradoxical worsening of seizures. In one study of 350 adults with uncontrolled seizures, 29% were found to have been prescribed an inappropriate ASM. 21 ASM-related seizure aggravation has been defined by the possibility of increased seizure frequency, seizure severity, or appearance of new seizure types and is reversed on discontinuation of the drug. 22 It has been shown that ASMs primarily exerting their antiseizure activity via sodium channel blockade could exacerbate seizures in Dravet syndrome. Also, carbamazepine, phenytoin, and tiagabine have been shown to aggravate idiopathic generalized epilepsy, particularly typical absences and myoclonic jerks. 23
Pharmacokinetics and drug-drug interactions
An ideal ASM should demonstrate complete absorption, linear kinetics, a long elimination half-life, and allow once or twice-daily dosing. Other favorable properties include low protein binding, lack of active metabolites, and kidney clearance. Although the optimal ASM regimen would consist of a single ASM, combinations of ASMs are used frequently in patients not responding to monotherapy. 24 When ASM polytherapy is used, clinically relevant interactions between ASMs are possible. Besides, ASMs may be combined with other drugs used to treat intercurrent or associated conditions. Drug-drug interactions could lead to either inadequate seizure control or drug toxicity. Consideration of ASM pharmacokinetic properties is crucial for avoiding drug-drug interactions.
Carbamazepine, oxcarbazepine, eslicarbazepine, phenobarbital, phenytoin, and primidone are inducers of hepatic cytochrome P450 enzymes (CYP), including CYP1A2, CYP2C9, CYP2C19, and CYP3A4, as well as glucuronyl transferases and epoxide hydrolase. 25 They may decrease the effects of other drugs administered concomitantly. Lamotrigine, perampanel, tiagabine, topiramate, and zonisamide also undergo hepatic drug metabolism and have potential drug interactions. 7 However, the newer generation ASMs, levetiracetam, gabapentin, pregabalin, and vigabatrin, are eliminated unchanged by the kidney and have no drug–drug interactions. ASM levels can be helpful to guide dose adjustments when an interacting medication is added.
Tolerability and safety
Medication intolerance is a frequent cause of ASM discontinuation, highlighting the importance of considering an ASM's adverse effect profile. 19 Third-generation ASMs have shown advantages in tolerability and safety, particularly in treating older patients and women of childbearing potential. 5 Carbamazepine, oxcarbazepine, lamotrigine, and phenytoin are highly associated with allergic drug reactions, including skin rash. Given the potential for cross-reactivity among aromatic ASMs, these should be avoided in any patient with a previous drug-induced skin eruption on any of these medications. 6 Genetic polymorphisms in drug-metabolizing enzymes such as CYP enzymes, drug transporters, and the HLA system have also been shown to influence ADR occurrence. 26 When available, this information should guide the selection and dosing of ASMs.
Medication formulation
In acute hospitalizations, frequent convulsive seizures, and other scenarios warranting rapid titration of ASMs, it is essential to consider ASMs that can be titrated rapidly, such as levetiracetam and phenytoin, over ASMs requiring several weeks of titration, including cenobamate or lamotrigine. Some patients may prefer an ASM with once-daily dosing for convenience, decreased side effects, increased tolerability, and improved adherence. Examples of ASMs with extended-release formulations or a long half-life that allow once-daily dosing include levetiracetam, eslicarbazepine, zonisamide, perampanel, and cenobamate. The formulation may also be essential in some patient populations, with liquid formulations preferred in children and those with dysphagia or tube feeding. ASMs available in liquid formulations include valproic acid, lamotrigine, oxcarbazepine, felbamate, levetiracetam, and phenytoin.
Cost
Cost is an important, albeit often overlooked, factor that should be considered in selecting ASMs. For some patients, brand-name medications can be prohibitively expensive. Generally, third-generation ASMs only available by brand manufacturers are more expensive than older-generation ASMs. Although accounting for a minority of prescriptions, in 2018, brand-name medications accounted for nearly 80% of costs associated with ASMs. 27 Before the expiration of lacosamide’s patent in 2022, the brand-only Vimpat was estimated to represent nearly 40% of the costs associated with ASMs. 28 As the availability of generic medications increases, a commensurate attenuation in brand-only ASMs could reduce costs to patients and the broader healthcare system. 27 However, there is evidence that switching brands to generic manufacturers could increase the risk of breakthrough seizures in previously seizure-free adult patients. In a matched control study of over 3500 patients with epilepsy, switching from brand-name to generic ASMs and switching between different generic manufacturers were both associated with a greater risk of breakthrough seizures in previously seizure-free patients. 29
Patient characteristics
Age
When it comes to epilepsy, older adults are a particularly special population. They are more likely to have multiple medical comorbidities, which may give rise to adverse effects related to polypharmacy, pharmacokinetic interactions, and their underlying comorbidities. 30 There are some considerations to guide ASM selection in this patient population. Enzyme-inducing ASMs and valproate are generally avoided, given the propensity for potential pharmacokinetic interactions with other medications. 6 Oxcarbazepine and eslicarbazepine are also generally avoided, given the increased risk of hyponatremia, which other medications, including antihypertensives, may potentiate. 6 Furthermore, decreased renal clearance and hepatic metabolism in this patient population result in greater sensitivity to adverse events. Therefore, using the lowest effective dose in this patient population is prudent.
Lamotrigine is regarded as being well tolerated among older adults with epilepsy when compared to other conventional sodium channel blockers with a lower risk of adverse effects. 20 Levetiracetam has also been well tolerated in this patient population, demonstrating superior tolerability, particularly when compared to valproic acid and carbamazepine. 31 However, the side effects reported by patients receiving levetiracetam, including somnolence and dizziness, can contribute to increased fall risk, particularly in the setting of other risk factors such as polypharmacy. 32 Although not extensively studied, lacosamide and zonisamide have also been reported to be relatively well tolerated in this patient population. 33
Sex
Another essential consideration is sex, specifically for women with epilepsy. When considering the initiation of ASMs in women with epilepsy of childbearing potential (WCP), several factors should be considered apart from the general principles of tolerability and adverse effect profile. Oral contraception methods should also be discussed with WCP, particularly those on enzyme-inducing ASMs, as these may result in contraceptive failure, posing an increased risk of unintended pregnancy. 34 On the other hand, estrogen-containing hormonal contraceptives have been associated with decreased serum concentrations of lamotrigine, posing an increased risk for breakthrough seizures. 25 Besides, folate supplementation should be recommended for all WCP, given the risk of neural tube defects and neurocognitive outcomes associated with folate deficiency. 35
Pregnancy
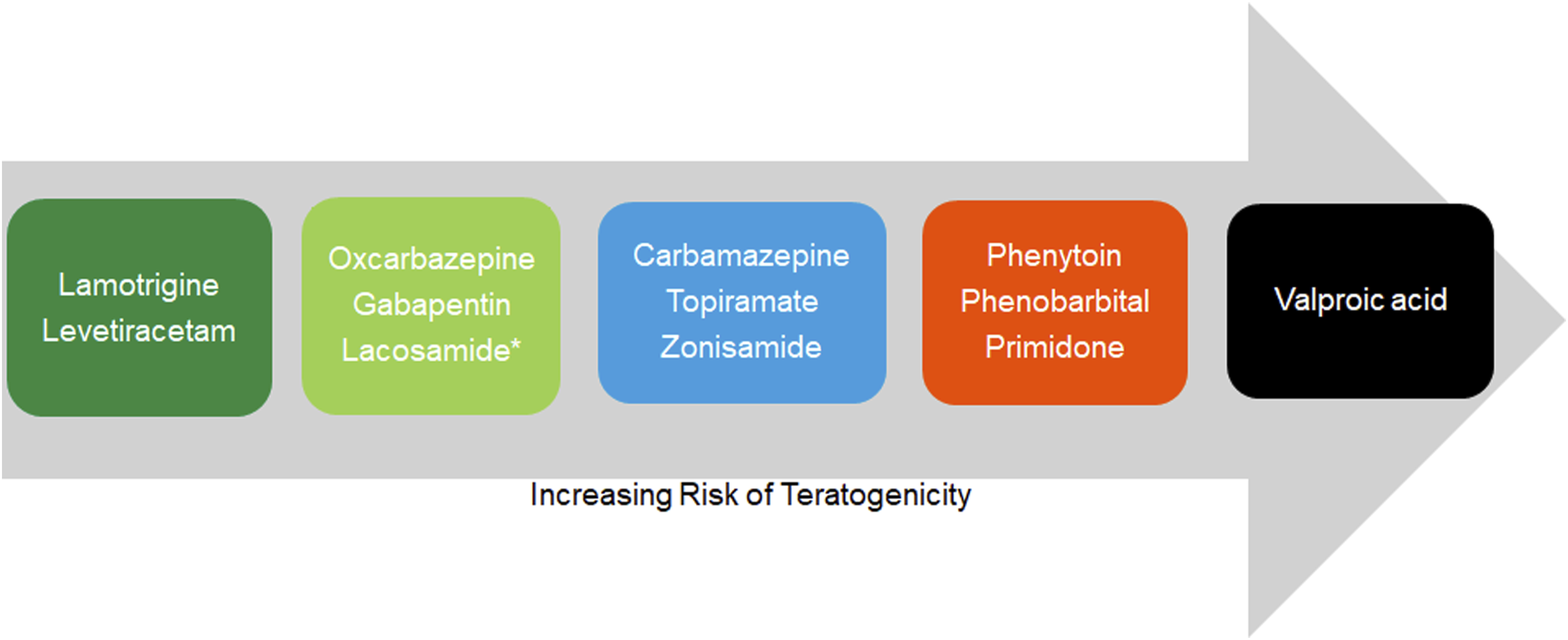
ASM treatment during pregnancy is a precarious balancing act between teratogenic risks to the fetus and maintaining maternal seizure control. Thus, when prescribing ASMs to WCP, the spectrum of potential teratogenicity should be taken into consideration. Lamotrigine and levetiracetam are considered the first line.36,37 Small studies have also shown that oxcarbazepine may be considered favorable concerning the risk of major congenital malformations.36,38,39 At the other end of the spectrum, in utero, exposure to valproate has been associated with three times the risk of major congenital malformations and should be ideally avoided.
36
In between lie several ASMs that can be associated with an elevated risk of teratogenicity in a large meta-analysis evaluating the risk of major congenital malformations: ethosuximide, topiramate, phenobarbital, phenytoin, and carbamazepine.37,40,41 While studies have found that clobazam and zonisamide are potentially associated with an increased risk of major congenital malformations, studies of other third-generation ASMs, including eslicarbazepine, lacosamide, perampanel, and gabapentin have mainly been equivocal.42-47 Polytherapy involving two or more ASMs poses a more significant risk than ASM monotherapy. One study found that the risk of major congenital malformations was 1.6 times greater in pregnancies involving two ASMs.
48
Figure 3 summarizes the relative teratogenic risk profiles of ASMs based on available data.
36
In addition to the risk for teratogenicity, the potential effects of ASM exposure on children's long-term neurodevelopmental and cognitive outcomes should also be considered. 36 Valproate exposure, in particular, has been associated with an increased risk of autism spectrum disorders, attention-deficit/hyperactivity disorder, intellectual disability, and developmental delay.49-51 Developmental delay and intellectual disability have also been associated with exposure to phenobarbital, phenytoin, carbamazepine, clonazepam, and pregabalin.50,52-54 Other ASMs, including gabapentin, topiramate, zonisamide, eslicarbazepine, lacosamide, and perampanel, have been insufficiently investigated concerning their effects on neurodevelopmental outcomes. 55 Other factors to consider include restricted intrauterine growth with valproate, reduced gestational age at delivery with carbamazepine and gabapentin, small gestational age with topiramate, and preterm birth with gabapentin.47,56,57
Race
Race and ethnicity should also be taken into consideration when prescribing aromatic ASMs, including phenytoin, carbamazepine, oxcarbazepine, and lamotrigine, given the predisposition of specific human leukocyte antigen (HLA) alleles to severe drug reactions, including Stevens-Johnson syndrome (SJS), toxic epidermal necrolysis (TEN), and drug reactions with eosinophilia and systemic symptoms (DRESS). 58 The HLA-B*1502 allele was initially found to be associated with SJS/TEN among Han Chinese patients exposed to carbamazepine. 58 This allele has also been associated with SJS/TEN among patients exposed to phenytoin, lamotrigine, and oxcarbazepine in other Asian ethnic groups.59,60 Given the concern for cross-reactivity among aromatic ASMs, while genotype testing is recommended in Han Chinese and Southeast Asian patients, it should be strongly considered in any patient of Asian ancestry, including South Asians, before initiating an aromatic ASM. 60
Etiology
The etiology of epilepsy plays a vital role in its management, including the selection of ASM therapy. For those with structural causes of epilepsy amenable to surgical resection, early referral of patients with drug-resistant epilepsy (DRE) to level IV epilepsy centers is recommended. On the other hand, for patients with immune-mediated seizures, early initiation of immunotherapy has been shown to favor a better prognosis regarding seizure control and cognitive outcomes. 61
While some ASMs are favored, others must be used cautiously, depending on the etiology. For example, in patients with Alzheimer’s disease, levetiracetam and lamotrigine have been demonstrated to have superior efficacy and tolerability. 62 Similarly, for poststroke epilepsy, expert recommendation favors using third-generation ASMs, gabapentin, levetiracetam, and lamotrigine due to low seizure recurrence and fewer side effects and interactions. 63 Conversely, combining strong enzyme-inducing ASMs, including carbamazepine and phenytoin, with new oral anticoagulants, such as apixaban or dabigatran, is discouraged. In patients with glioma-related epilepsy, levetiracetam and valproic acid are the preferred first-line agents. 64 In a recent observational cohort study, valproate and levetiracetam were tolerated well and more effective than any other combination of levetiracetam or valproate. 65 Lastly, adjunct ASM therapy with sodium channel-blocking properties is preferable in patients with autoimmune-associated epilepsy. 66
Comorbidities
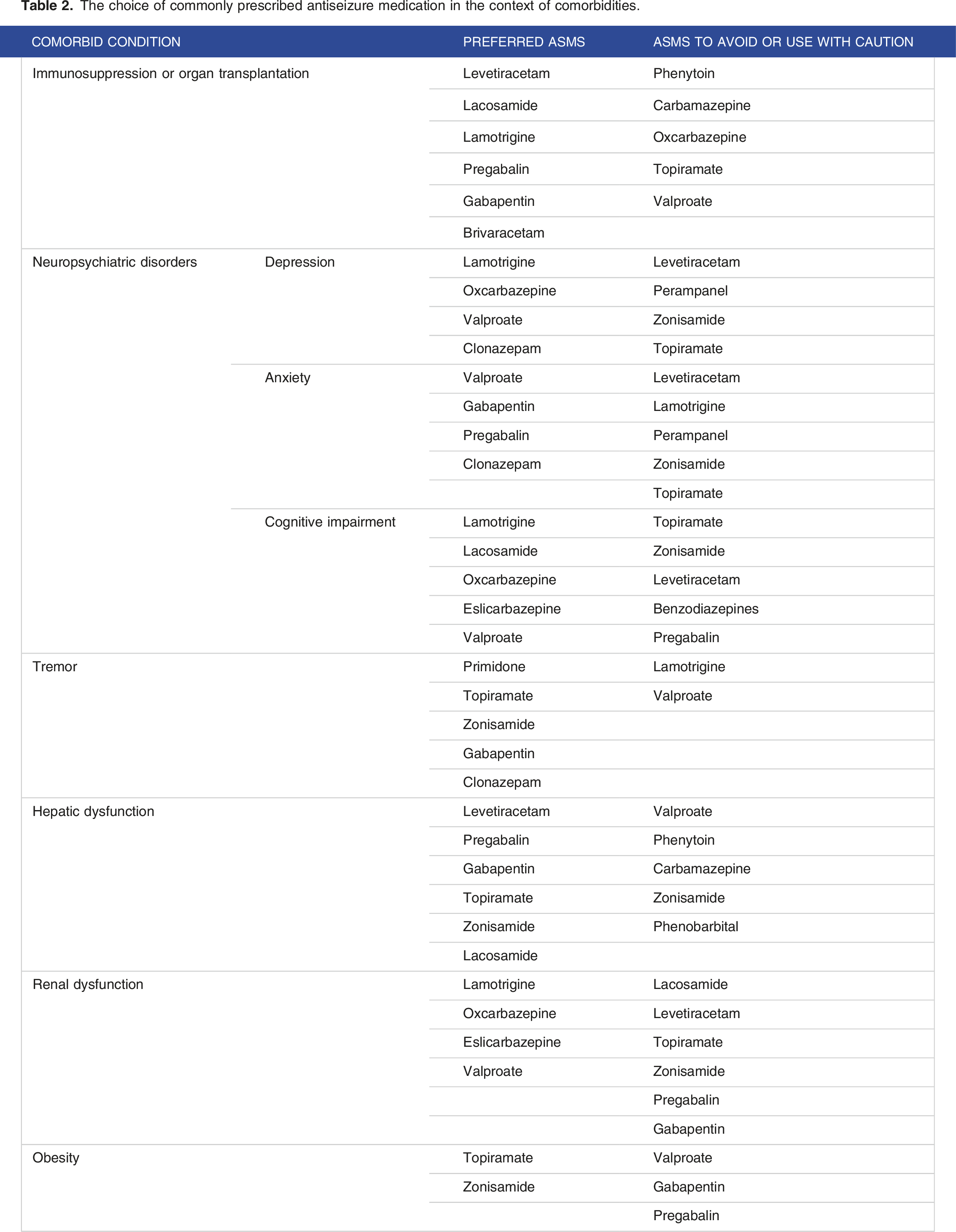
The choice of commonly prescribed antiseizure medication in the context of comorbidities.
Future of ASM therapy
With more than 30 ASMs available for treating epilepsy, ASM selection in clinical practice remains largely empirical and based on trial and error. It is impossible to predict which ASM will be most effective and tolerated for a given patient, and typically, various ASMs are sequentially trialed if seizures persist. Under the current approach, patients may endure multiple trials of ineffective treatments before finding the right ASM. Soon, physicians could consult web-based practical algorithms or deep machine learning (ML) models to aid individualized ASM selection and identify patients with a high risk of drug resistance or adverse events. Besides, the recognition of epilepsy as a network disorder and the integration of personalized altered network structure and function68,69 in future ML platforms could help predict ASM response. These platforms promise personalized pharmacotherapy in epilepsy, an elusive goal for decades.
70
A simplified conceptual view of how personalized ASM therapy through ML and novel drug delivery methods may be applied in clinical epilepsy is illustrated in Figure 4.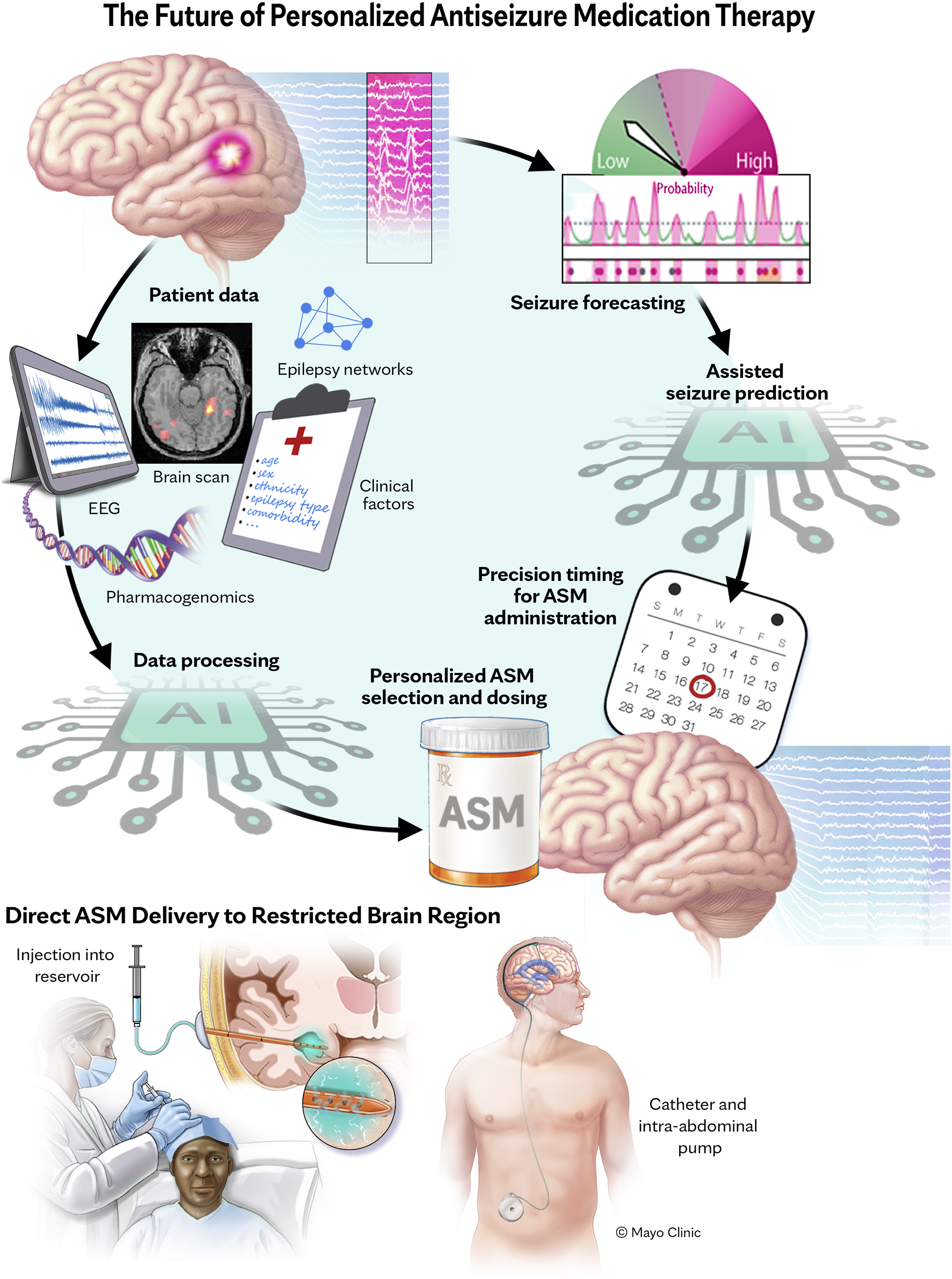
Web-based decision support systems
Web-based decision support systems have been developed to facilitate appropriate ASM selection.71,72 These consider several patient-specific variables and rank ASMs in order of likely appropriateness for an individual patient based on the best available scientific evidence. Algorithms such as EpiPick have been recently developed to guide the selection of first-line ASMs. 71 An external validation study of the EpiPick algorithm has found that patients prescribed the first-line ASMs selected by the algorithm experienced higher rates of seizure freedom and lower rates of ASM discontinuation due to adverse effects. 72
Artificial Intelligence-tailored ASM selection
Recent advances in the ability to generate molecular data and parallel advances in AI, specifically ML and high-performance computing, offer novel ways to develop more accurate prediction models. Such ML models can be used to make individual patient-level predictions. Their interpretation can drive the development of a more holistic understanding of ASM efficacy and tolerability for the individual patient. Integrating data on personalized epileptic networks to AI models could also facilitate predicting ASM response. Besides, these models can also be instrumental in translating precision medicine into clinical practice in epilepsy. Moreover, these advances could help primary care physicians in their ASM prescribing, especially in rural areas with limited access to neurologists.
AI-based prediction of clinical response
Many recent studies have developed ML models for identifying the best choice of ASMs for patients with epilepsy.73-77 In one study, the use of ML predicted ASM regimens associated with improved outcomes and reduced costs due to lower healthcare utilization rates. 74 A recent study, using data from nearly 1800 adults with newly diagnosed epilepsy across four countries, developed a deep ML model 77 to predict the effectiveness of an ASM, defined as at least one year of seizure freedom. 75 The model considered lamotrigine, valproate, carbamazepine, levetiracetam, oxcarbazepine, topiramate, and phenytoin. Several variables were fed into the model, including sex, age at the onset of treatment, clinical history including the presence of febrile convulsions or significant head trauma, the presence of cerebrovascular disease or intellectual disability, number of seizures, seizure classification, and EEG and brain imaging findings. Overall, the authors reported that the performance metrics across these 6 ML algorithms appeared to be modest, with the area under the receiver operating characteristics curve (AUCOC) ranging from the high .50s to the low .60s in the first experiment and from the mid-.40s to the low .60s in the second experiment, with sensitivities and specificities within a similar range.
The AI platform could also help identify the most essential factors in predicting ASM treatment success by epilepsy type.76,77 Wu et al 77 developed an AI model to predict response to ASMs in patients with idiopathic generalized epilepsy. They found that the number of seizure types and pretreatment seizure frequency were among the most effective predictors of ASM response. In a study investigating an AI model to predict ASM response in patients with focal epilepsy, Lee et al 76 found that clinical factors were a more useful indicator of ASM success than imaging findings, such as diffuse tensor imaging.
Integration of personalized epilepsy networks in AI-based platforms
Epilepsy is increasingly conceptualized as a disorder of brain networks.68,69,78,79 The epileptic brain network comprises structurally and functionally connected cortical and subcortical brain regions whose connections and dynamics evolve.68,69 The network approach offers a robust framework to improve understanding of the epileptic brain's spatial–temporal dynamics, which provides essential clues for the success or failure of network-based seizure control and prevention measures. 68 Prior studies have demonstrated the impact of ASM on brain function or network. 80 Significantly, some have speculated that the therapeutical effect of ASMs on epileptic seizures is underpinned by their effects on neural networks. 81 With network-centric interventions such as ASM therapy, adequate long-term seizure control could be reached in about 70% of treated patients with epilepsy. 2 The integration of personalized altered networks in future AI platforms has the potential to predict response to ASMs.
Prior studies have also explored the characteristics of neuronal networks in patients who achieve persistent seizure freedom with ASMs. 81 Tan and colleagues 81 investigated the characteristics of brain function and neural networks for chronic epilepsy patients with long-term seizure freedom before and after ASM withdrawal. They found that the local functional activity or nodal metrics of neural networks in some brain areas differed between groups. Quantifying changes in the epileptic network before and after epilepsy surgery can also elucidate network reorganization, augmenting clinical decisions such as whether to wean ASMs. 69 Epileptic networks might be more altered in DRE patients, and measuring these alterations can be a marker for the prognosis of ASM resistance in the early stages of epilepsy treatment. 69 Even in non-lesional newly diagnosed focal epilepsy patients, those with DRE were shown to have bilateral structural network impairment compared to patients who were seizure-free with ASMs at 24 months since diagnosis. 82 These studies suggest that mapping altered epileptic networks could potentially facilitate decisions on ASM therapy, thereby allowing early referral to epilepsy surgery or consideration of ASM wean. However, further studies analyzing the longitudinal changing characteristics of brain function and neural networks during ASM therapy are needed to provide further insights.
AI-based prediction of adverse drug reactions
Despite numerous attempts to develop safe, harmless ASMs, ADRs are unavoidable. ADRs complicate seizure control and adherence and contribute to treatment withdrawal in approximately 25% of patients. 83 In addition to affecting the patient's quality of life, there is also an economic burden associated with ADRs. Genetic polymorphisms in drug-metabolizing enzymes such as CYP enzymes, drug transporters, and the HLA system have been shown to influence ADR occurrence. 26 Knowledge of genetic polymorphisms could also guide the tolerated maximum daily dose of an individual ASM. In addition, genetic factors may contribute to the high variability in response to ASMs across people with epilepsy. Integrating these pharmacogenetic biomarkers in future AI platforms could enable us to predict ADRs and the efficacy of ASMs.
Is AI-assisted ASM selection ready for prime time?
The recently developed ML models for predicting treatment response on initial ASM monotherapy in patients newly diagnosed with epilepsy have shown the feasibility of an individualized treatment approach. The question remains whether the modest performance attained by these algorithms exceeds the intuition of experienced clinicians. After all, two-thirds of people with epilepsy currently achieve seizure control with pharmacotherapy using clinician experience alone. Additional improvements will be needed before ML methods for personalized prediction of ASM response are considered ready for primetime clinical practice. Studies are also needed to explore more advanced and complex graphical AI models and use data from large, longitudinal epilepsy registries so that comprehensive information can be mined from patients’ medical records. Besides, future studies should explore ML models to guide treatment decisions for second and subsequent ASM regimens in a personalized manner for those with DRE.
Seizure forecasting with AI tailoring ASM dosing and frequency
AI is also being explored in epilepsy to forecast and detect seizures. Seizure forecasting could influence ASM therapy dosing and frequency. Patients can be relieved from the adverse consequences of epileptic seizures if predicted in advance. Besides, accurately predicting seizures before they occur can obviate the need for year-round ASM administration in patients with infrequent seizures. Conversely, for patients only able to tolerate a low dose, higher doses could be used on days when the risk for seizures is higher. With accurate seizure forecasting, the possibility of anticipatory administration of ASMs also has the potential to reduce the financial burden of ASMs and morbidity associated with the short and long-term ADR associated with their use. There have been exciting new developments in AI-based algorithms in the early and accurate prediction of epileptic seizures, which could alter ASM therapy practice.84,85 However, more work must be done, including ensuring forecasting is as accurate as possible and determining how patients wish to receive the seizure forecasts before these are integrated into clinical decision support systems.
Novel modes of ASM delivery
Improving the delivery of ASMs is another area of exploration. Applying ASMs to a restricted brain region can produce high drug concentrations in the region of seizure onset and spread. 86 This approach may control seizures while avoiding the peripheral and central side effects that limit oral drug administration. Direct drug delivery is an appealing treatment alternative for patients with DRE. In a recent proof-of-concept study, Cook and colleagues 87 demonstrated that chronic intraventricular administration of valproic acid is safe and effective in subjects with DRE over many months. High cerebrospinal fluid levels were achieved with corresponding low serum levels. The intraventricular drug delivery was effective despite the unsuccessful earlier use of oral valproate preparations. Nevertheless, future studies are needed to determine whether such invasive routes of administration of already established ASMs are safe and effective before adopting these in the clinic.
Conclusions
Recommending the most appropriate ASM for an individual can be challenging, and weighing key clinical variables requires experience and expertise, which may be limited in some settings. Moreover, it can be difficult for clinicians to apply objective criteria consistently when making treatment decisions, leading to variability in clinical management. A complex tapestry of patient and medication-related factors must be considered when tailoring a patient’s ASM regimen. As new ASMs and drug delivery systems are being investigated, AI is a burgeoning area of inquiry that may soon yield an indispensable resource in the era of personalized medicine, including selecting the most effective and tolerated ASM regimen. Besides, integrating data on epilepsy networks in future AI platforms could help predict ASM response, thereby informing clinical decisions such as whether to wean ASMs or early referral to epilepsy surgery. Augmenting the conventional approach of ASM selection with AI opens the door to personalized pharmacotherapy in epilepsy, an elusive goal for decades. However, a rigorous validation pipeline is required before these models can be moved into clinical practice. Future studies integrating broader clinical biomarkers, including genetic, EEG, epileptic networks, and imaging data in these platforms, are also needed to improve their accuracy.
Footnotes
Acknowledgements
We thank Joanna King, MSMI, Creative Director, Biomedical & Scientific Visualization at Mayo Clinic, Rochester, for creating illustrative figures in this article.
Author contributions
Editing. Dr. Sirven: Conceptualization; Supervision; Writing – review & editing. Dr. Feyissa: Conceptualization; Data curation; Methodology; Supervision; Writing –
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.