
Abstract
Background:
People with neurological disorders are found to have abnormal resting-state functional connectivity (rsFC), which is associated with the persistent functional impairment found in these patients. Recently, transcranial direct current stimulation (tDCS) has been shown to improve rsFC, although the results are inconsistent.
Objective:
We hope to explore whether tDCS induces rsFC changes among patients with neurological disorders, whether rsFC is clinically relevant and how different tDCS parameters affect rsFC outcome among these individuals.
Methods:
A systematic review was conducted according to PRISMA guidelines (systematic review registration number: CRD42020168654). Randomized controlled trials that studied the tDCS effects on rsFC between the experimental and sham-controlled groups using either electrophysiological or neuroimaging methods were included.
Results:
Active tDCS can induce changes in both localized (ie, brain regions under the transcranial electrodes) and diffused (ie, brain regions not directly influenced by the transcranial electrodes) rsFC. Interestingly, fMRI studies showed that the default mode network was enhanced regardless of patients’ diagnoses, the stimulation paradigms used or the rsFC analytical methods employed. Second, stimulation intensity, but not total stimulation time, appeared to positively influence the effect of tDCS on rsFC.
Limitations and conclusion:
Due to the inherent heterogeneity in rsFC analytical methods and tDCS protocols, meta-analysis was not conducted. We recommend that future studies may investigate the effect of tDCS on rsFC for repeated cathodal stimulation. For clinicians, we suggest anodal stimulation at a higher stimulation intensity within the safety limit may maximize tDCS effects in modulating aberrant functional connectivity of patients with neurological disorders.
Keywords
Introduction
Neurological disorders encompass a wide range of diseases involving abnormalities in the central and peripheral nervous systems. 1 These disorders contribute to the leading causes of disability and death, contributing to nearly 12% of global disabilities and approximately 17% of global deaths. 2 Although the etiologies of different neurological disorders are inherently distinctive, which results in a great variety of physical/mental dysfunctions, aberrant network functioning in the brain is a common issue that has been associated with the persistence of impairments among these individuals. 3
Neural network functioning can be quantified in multiple ways, of which functional connectivity (FC) is one of the indicators commonly used in academia. FC is defined as the statistical dependencies among remote neurophysiological events, which reflects the degree of the nondirectional synchrony between 2 brain regions. 4 FC can be broadly categorized into 2 types—task-based FC and resting-state FC (rsFC). Rather than recording brain network activity during performance of a task that engages certain neural processes (eg, motor network recruited during the finger tapping task), measurements of rsFC, which results in the discoveries of resting-state networks, 5 are taken when an individual’s task engagement is minimal (eg, eye-closed rest, passive fixation), that is, when the person is “at rest.” 6 Due to the great variety of experimental paradigms adopted in different studies, comparing task-based FC between studies could be challenging; rsFC serves as an alternative option that makes a comparison more feasible by minimizing the impact from paradigm designs. 7 In terms of measurement, rsFC can be studied with neurophysiological (eg, electroencephalography, EEG) or neuroimaging (eg, functional magnetic resonance imaging, fMRI) methods, which complement the limitations of each other, 8 leading to a more holistic understanding of brain functions. 9 While EEG rsFC measures the phase synchronization between 2 electrical signals measured by 2 scalp electrodes located in different positions, 10 fMRI rsFC is determined by the synchrony of the low-frequency fluctuations in blood-oxygen-level-dependent (BOLD) signals detected in 2 different brain regions. 11 To determine the degree of synchrony, there are a number of analytical approaches for each measurement method; while coherence, phase-locking value and graph theory approaches are commonly utilized to evaluate EEG data, 12 independent component analysis (ICA), seed-based FC analysis and graph analysis are widely adopted in the fMRI research world. 13
A growing body of evidence indicates that rsFC is closely associated with specific neural processes that support motor, cognitive and perceptual functions, 14 which also predicts recovery from diseases as well as success in one’s daily life functioning. 15 People with neurological disorders who manifest different types and levels of functional impairments are found to have abnormal rsFC when compared to their healthy counterparts, which has also been shown to correlate with the severity of signs and symptoms. For instance, from a meta-analysis studying rsFC among people with depression when compared to healthy controls, patients were found to have a hypoconnected brain network for cognitive control and attention and a hyperconnected network for self-referential thoughts. 16 Another meta-analysis showed internetwork hypoconnectivity in patients with schizophrenia when compared to controls. 17 Other diagnoses with individuals who manifest different kinds of intra/internetwork rsFC abnormalities include but are not limited to attention-deficit/hyperactivity disorder, 18 stroke, 19 Parkinson’s disease, 20 and fibromyalgia. 21 These studies collectively imply that rsFC abnormalities can be identified in many neurological disorders, which are found to be a problem underlying persistent cognitive/motor/perceptual dysfunctions.
In recent decades, increasing efforts have been made regarding the development of treatment techniques that potentially alleviate rsFC abnormalities among people with neurological disorders. One of the potentially promising techniques is transcranial direct current stimulation (tDCS). 22 During tDCS application, a weak direct current (1-2 mA) is passed through the brain by connecting a battery with 2 electrodes that are placed over the scalp. 23 The transcranial electric current has been found to modulate neuronal excitability in humans. 24 Sustained stimulation has been found to result in long-lasting cortical excitability, a phenomenon that resembles the putative neurophysiological mechanism of learning and memory—long-term potentiation. 25 Most of the previous electrophysiological and neuroimaging studies have focused on the regional effects of tDCS in both healthy people and those with neurological disorders (eg, epilepsy 26 and depression 27 ), showing encouraging results that indicate tDCS can indeed alter neuroplasticity, which correlates with cognitive and motor function improvements. 28 With the understanding that brain regions do not act separately but rather are functionally connected, more researchers have started to investigate the effect of tDCS on network connectivity via rsFC in healthy individuals and patients with neurological disorders.29,30
Despite the fact that some studies reported significant changes in rsFC after patients received tDCS,30,31 others reported negative results. 32 It has been suggested that interindividual variability in brain structures, 22 study designs, 33 variations in tDCS stimulation protocols used among different studies 34 or even differential analytical methods for rsFC 35 could result in inconsistent results between studies. To the best of our knowledge, there is no previously published paper that synthesizes the available studies that investigate tDCS effects on rsFC among people with neurological disorders, leaving these inconsistencies unexplained. Thus, we hope to address 3 questions by conducting a systematic review: (1) whether tDCS induces rsFC changes among patients with neurological disorders, (2) whether these rsFC changes correlate with clinical outcomes (representing the clinical relevance of tDCS effects on rsFC), and (3) how different tDCS parameters affect rsFC outcome among these patients.
Methods
Literature search
This systematic review was performed with guidance from the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) 36 and was registered in the International Prospective Register of Systematic Reviews system (PROSPERO; register ID: CRD42020168654). A preliminary search was conducted in early February 2020 to confirm the choice of keywords and electronic databases among all authors. A main literature search for retrieving relevant records was conducted on 18-19 February 2020 with the search terms “transcranial direct current stimulation,” “tDCS,” “functional magnetic resonance imaging,” “fMRI,” “electroencephalography,” and “EEG” from the electronic databases PsycINFO, Scopus, Embase, and Web of Science. No limit was set for the publication dates. Hand searching of the reference lists of the relevant articles was performed to identify additional records.30,31
Study inclusion
Randomized parallel group/crossover trials, which administered active tDCS stimulation in the experimental group and sham tDCS stimulation in the control group, on patients with neurological disorders as defined in The International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10), 37 with functional connectivity outcomes measured by either resting-state EEG/fMRI were included in this review. The article screening process could be divided into 3 parts. First, duplicated records were removed. Then, titles and abstracts of the articles were screened; non-English papers, studies without peer-reviewed empirical data (eg, review, conference proceedings, book chapters, and editorial), observational studies (eg, case series, nonrandomized studies, and studies without a sham-tDCS control group), nonhuman studies, studies that did not apply tDCS to patients with any kinds of neurological disorders and studies that did not use tDCS as the sole brain stimulation technique were excluded. Finally, the full texts of the remaining studies were examined for systematic review eligibility. A paper would be included if (1) functional connectivity measures, recorded by either resting-state EEG or fMRI, were reported, (2) the functional connectivity measures were conducted at both baseline and after the treatment, and (3) between-group (ie, active- vs sham-stimulation) comparisons that reflected tDCS effects were reported. The above screening processes were independently conducted by the first author and an experienced research assistant, and their decisions were recorded in separate Excel spreadsheets. When there were discrepancies, the second author made the final decision regarding study inclusion.
Data extraction
After final decisions regarding the paper selection issues were made, the demographic data and experimental and outcome measurement details of the included papers were extracted and entered into an Excel spreadsheet by the first author, which was checked by the second author to minimize errors. Demographic data included the diagnosis, number of participants in each group (N), age, and whether participants were on concurrent medication within the experimental period. Experimental details included the montage placement, tDCS stimulation current intensity (mA), duration of stimulation for each session (minutes), total number of treatment sessions, and concurrent task accompanied during tDCS stimulation. Outcome measures included the assessments used for measuring the clinical effect, posttreatment between-group difference of fMRI/EEG rsFC data (or between-group contrast showing changes of rsFC from pretreatment to posttreatment) and the description/statistics showing the association between the change in rsFC measures and the change in clinical outcomes. Electronic mail was sent to the corresponding authors to ask for additional information/clarification if the data to be extracted were not complete.
Data coding and synthesis
Extracted data were coded by the first author and then checked and confirmed by the second author. Participant age was recoded into 3 age groups (adolescent, adult, elderly), and montage placement was coded as an addition variable, “stimulation type,” according to a previously proposed framework. 38 We coded the “total stimulation time” by multiplying the total number of sessions by the stimulation time of each session, while the current density at the electrode (A/m2), which is a widely adopted parameter in animal research representing the current applied to the participants, 39 was calculated by dividing the current intensity by the electrode’s surface area. Based on the purposes of the clinical assessments used by each study, the clinical outcome would be categorized into 3 categories—symptomatic relief, enhancement of specific/global neurological function, and description/statistics showing the association between the change in rsFC and the change in clinical outcome recoded to be a dichotomous outcome (yes/no). For fMRI peak coordinates, recoding according to MNI space would be done if Talairach coordinates were given, followed by categorizing these brain regions within a priori rsFC networks (at a resolution of 400 parcels) defined by a local-global network parcellation in 1489 subjects. 40
In view of the marked diversity in the subdiagnoses under the branch of neurological disorders, as well as that regarding the rsFC analytical methods, meta-analysis was not planned. To answer whether tDCS induces rsFC changes, we provided a narrative synthesis of the results, supported by a forest plot that provides readers with a visual impression of the data. The effect size calculation and generation of the forest plot were performed using Comprehensive Meta-Analysis (CMA; Biostat, Englewood, NJ) software. Effect sizes for coordinate-based fMRI rsFC studies would be calculated for all reported T-values of the peak coordinates/P-values for all reported clusters. For the remaining studies, a combination of test statistics (eg, f-values, t-values, P-values) was used. 41 For studies that presented non-parametric statistics, effects sizes would be calculated manually according to the previously published formulae.41,42 For studies that did not report a pre-post correlation while reporting pre/posttreatment between-group contrast, a conservative estimation of pre-post correlation of r = .7 would be used.43,44 If test statistics were unable to be obtained after contacting the corresponding authors but the results were described in text, nonsignificant results would be assumed to have P-values of .5 (1-tailed) and significant results were assumed to have P-values of .05 45 ; these P-values were chosen as we opted to keep our estimation as conservative as possible. The forest plot was generated with the Hedges’s g effect size with 99% confidence intervals. A follow-up narrative synthesis would summarize whether the documented rsFC changes correlate with the clinical outcomes. To explore the effects of different tDCS parameters on rsFC outcomes for continuous data (ie, stimulation time and current density), we conducted meta-regressions with CMA software by plotting these parameters against g. For rsFC changes for discrete data (ie, stimulation type), narrative syntheses would be given. The risk of bias in individual studies was assessed by the Cochrane Collaboration’s tool. 46 Publication bias was evaluated by visual inspection of the funnel plot, 47 with a small-study effect evaluated with Egger’s test. 48
Results
Study selection
A total of 15 studies were included in this review. The electronic database search yielded a total of 3613 neurophysiological and neuroimaging studies (2226 EEG and 1387 fMRI records, respectively), with 2609 records remaining for abstract screening after the removal of 1004 duplicated records. A total of 2488 studies were excluded after exclusion criteria were applied at this stage. The full text of 121 records was further assessed for inclusion in the systematic review. One hundred studies were excluded as the primary outcome of our systematic review (ie, resting-state functional connectivity) was not reported in the papers (88 EEG and 12 fMRI records, respectively); 3 other studies were excluded because the primary outcome measure was not conducted at both baseline and after treatment. Between-group rsFC contrasts could not be obtained from 3 studies, and they were also excluded from the review. See Figure 1 for the diagram illustrating the article screening procedure and Supplemental Table A for the details of the 106 records excluded during full-text screening.

Flowchart of the article screening process.
Risk of bias within studies
A majority of studies showed unclear bias in random sequence generation, allocation concealment, incomplete outcome data. More than half of the studies adopted blinding procedures during treatment administration and outcome assessments. Although most of the studies reported both significant and non-significant results of between- and within-group comparisons, 4 studies did not report their data as planned in the methods section. Figure 2a displays the risk of bias items presented as percentages across all included studies, and Figure 2b shows the risk of bias summary for each included study. Supplemental Table B presents all of the authors’ judgment details for each study.
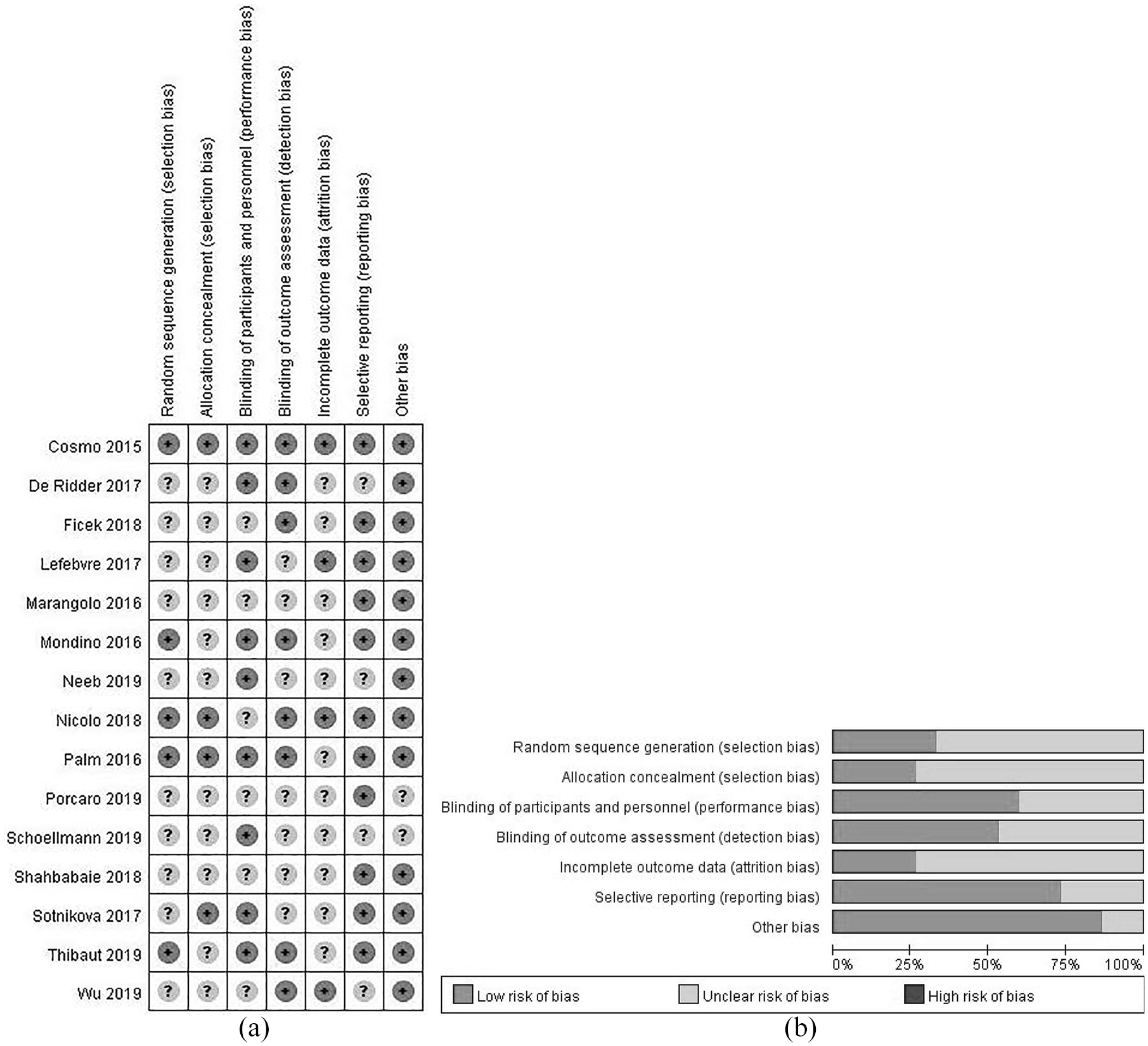
(a) Risk of bias graph: review authors’ judgments about each risk of bias item presented as percentages across all included studies. Note that an item was rated “+” (ie, low risk of bias) only when the measure taken to prevent certain risk of bias was clearly stated in the paper; when evidence/quotes or explanation were not available in the text or after clarifying with the authors of the included studies, a rating of “?” (ie, unclear risk of bias) was given and (b) review authors’ judgments about each risk of bias item for each included study. Note that “other bias” was defined as other sources of risk on top of selection, performance, detection, attrition, and reporting biases. Specifically, carry-over effects in cross-over trials and baseline imbalance between groups were considered as “other bias.”
Study characteristics
The included RCTs involved 348 patients in total from different age groups who suffered from a broad range of neurological disorders, including fibromyalgia, 49 inflammatory bowel disorder 50 and neuropsychiatric disorders (ie, schizophrenia,51,52 substance abuse 53 ), neurodegenerative disorders (ie, multiple sclerosis, 54 Parkinson’s disease, 55 primary progressive aphasia 56 ), neurodevelopmental disorders (ie, attention-deficit/hyperactivity disorder57,58), stroke,59,60 and disorders of consciousness. 61 These studies adopted a great variety of tDCS protocols and adopted a variety of rsFC analytic methods. A brief summary of the demographic, experimental and outcome measurement details of individual studies is shown in Table 1.
Summary of the demographic, experimental, and outcome measurement details of the included studies.

Abbreviations: A, active-tDCS; ADHD, attention-deficit/hyperactivity disorder; EEG, electroencephalography; fMRI, functional magnetic resonance imaging; N, number of participants; N/A, not applicable; rsFC, resting-state functional connectivity; S, sham-tDCS.
Effects of tDCS on inducing changes in rsFC and its clinical relevance
Figure 3 provides the overall summary of the included studies with a forest plot. All of the effect sizes were computed with the reported test statistics/P-values except for 4 studies,49,52,53,63 hypothetical P-values were assigned for these studies as planned. The plot indicated that tDCS could induce rsFC changes in patients with neurological disorders, as evident from neuroimaging and neurophysiological studies.
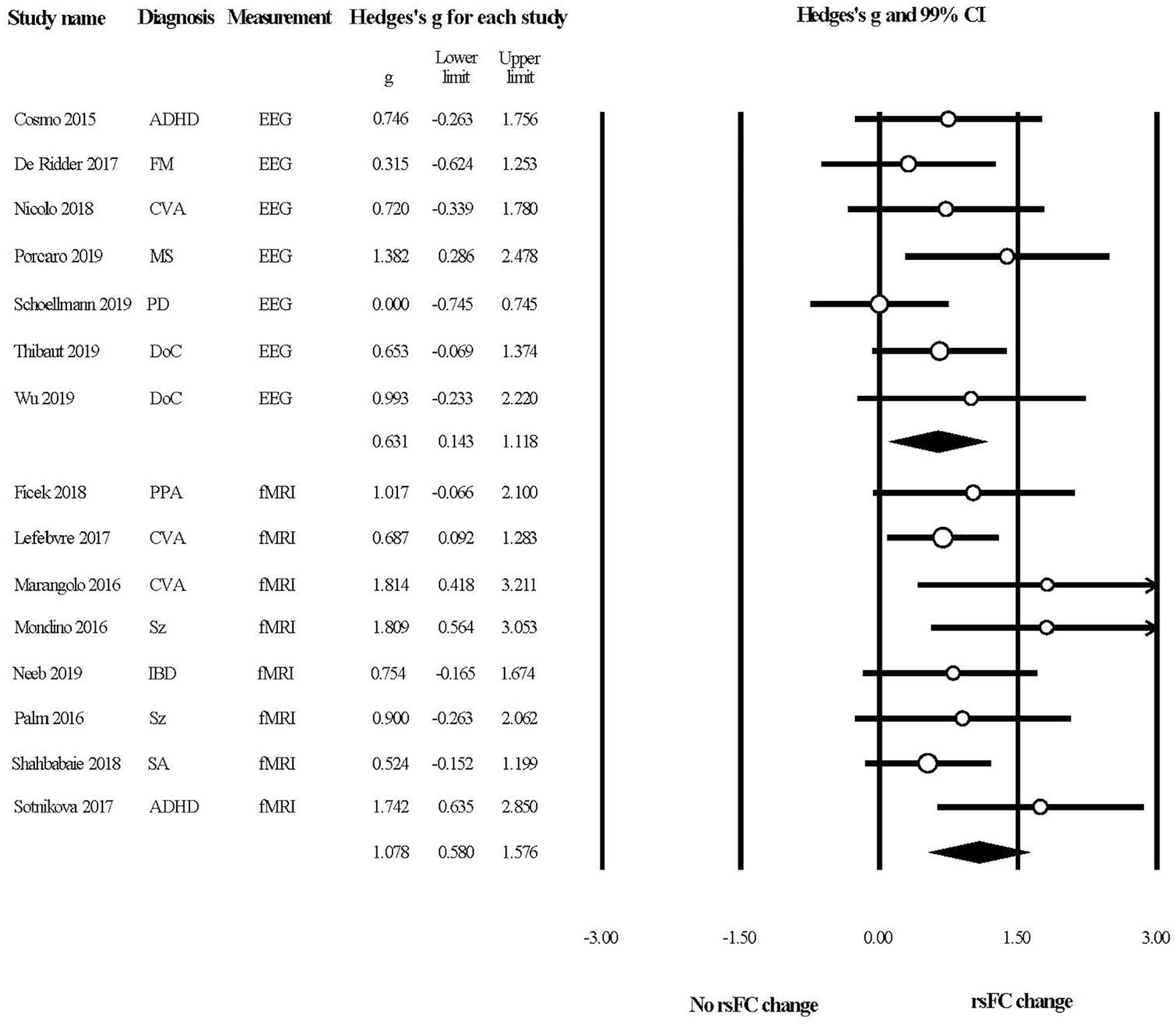
A forest plot summarizing the effects of tDCS in modulating rsFC in patients with neurological disorders.
The results from electrophysiological studies (Table 2) showed that rsFC near electrodes could be modulated by tDCS. Thibaut et al 61 reported an increase in rsFC between C3 and C4 electrodes (where the cathodes were placed), as well as between C4 (cathode placement) and F3 (anode placement) among patients with disorders of consciousness with multichannel bilateral stimulation. Similar changes could be found in the study conducted by Nicolo et al 60 on stroke patients, who reported an increase in the weighted node degree of C3/4 (cathode placement) for the beta, but not the alpha frequency band. However, negative results were reported by Cosmo et al 58 in which stimulation was applied to adults with ADHD over the dorsolateral prefrontal cortex. The local rsFC showed nonsignificant changes after active tDCS when compared to the sham group although this study was of the largest sample size (N = 30 for both the active and sham groups) among all included studies.
Summary of resting-state functional connectivity results from the functional magnetic resonance imaging (fMRI) studies.
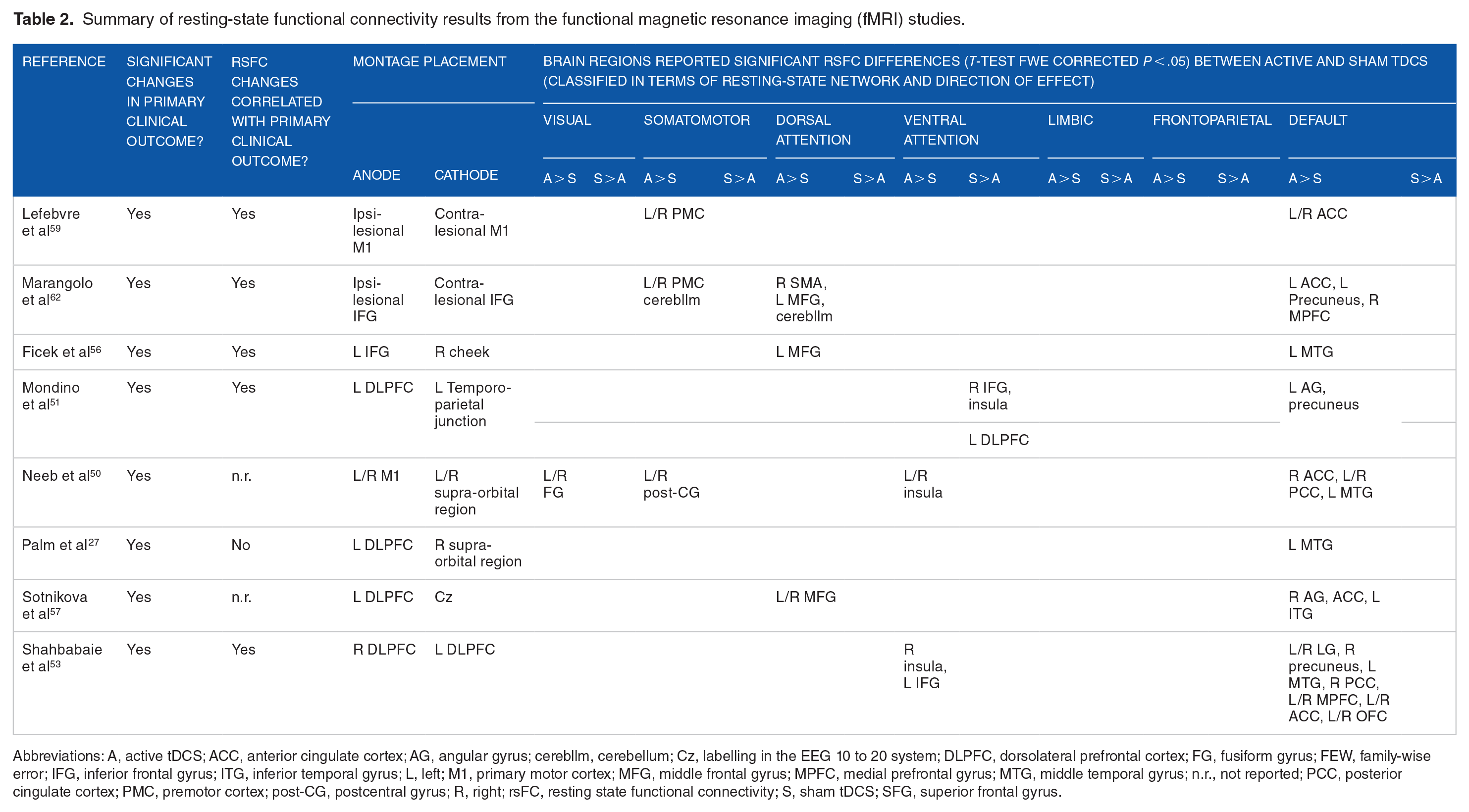
Abbreviations: A, active tDCS; ACC, anterior cingulate cortex; AG, angular gyrus; cerebllm, cerebellum; Cz, labelling in the EEG 10 to 20 system; DLPFC, dorsolateral prefrontal cortex; FG, fusiform gyrus; FEW, family-wise error; IFG, inferior frontal gyrus; ITG, inferior temporal gyrus; L, left; M1, primary motor cortex; MFG, middle frontal gyrus; MPFC, medial prefrontal gyrus; MTG, middle temporal gyrus; n.r., not reported; PCC, posterior cingulate cortex; PMC, premotor cortex; post-CG, postcentral gyrus; R, right; rsFC, resting state functional connectivity; S, sham tDCS; SFG, superior frontal gyrus.
Changes in rsFC are also shown within the brain regions that are functionally connected with the stimulated region. An EEG study by Porcaro et al 54 which applied tDCS to individuals with multiple sclerosis over the somatosensory region using a personalized anode, reported an increase in interhemisphere rsFC over the bilateral primary motor cortex. For fMRI studies (Table 3), when electrodes are placed over the primary motor cortex (M1), the rsFC of the somatomotor network, comprising brain regions such as the premotor cortex and the postcentral gyrus that are functionally connected to M1, increases50,59; when electrodes are placed over the inferior frontal gyrus,56,62 a brain region within the dorsal attention network, rsFC increased in the dorsal attention network.
Summary of resting-state functional connectivity results from the electroencephalography (EEG) studies.
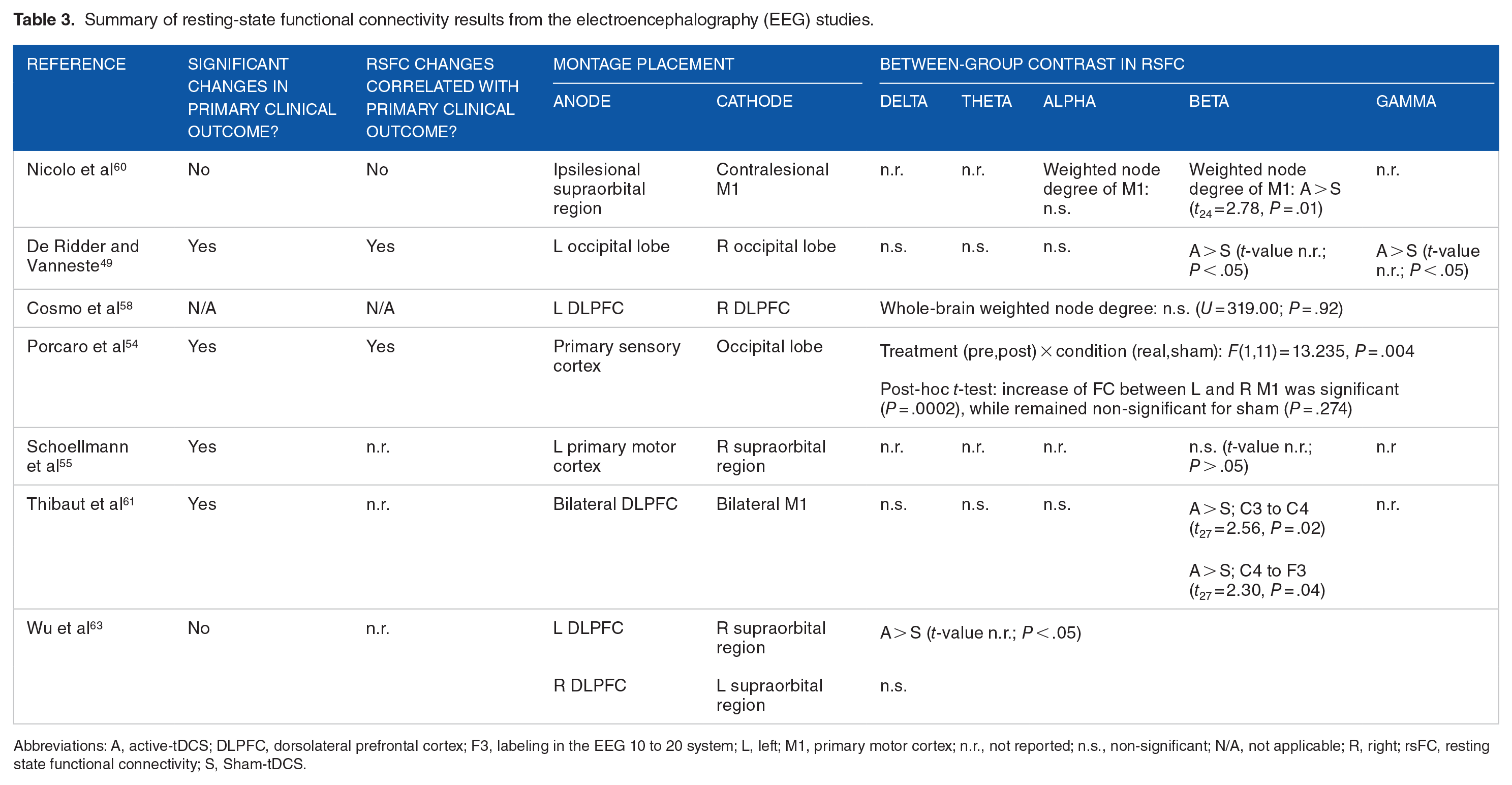
Abbreviations: A, active-tDCS; DLPFC, dorsolateral prefrontal cortex; F3, labeling in the EEG 10 to 20 system; L, left; M1, primary motor cortex; n.r., not reported; n.s., non-significant; N/A, not applicable; R, right; rsFC, resting state functional connectivity; S, Sham-tDCS.
Notably, rsFC modulation was found in brain networks that were not functionally connected to the brain regions directly under the scalp electrodes. Notably, all of the included fMRI studies induced rsFC changes to the default mode network (DMN; Table 3) regardless of the mode of stimulation and electrode placements. Another study conducted by De Ridder and Vanneste 49 reported an increase in lagged phase synchronization specifically at the beta and gamma frequency bands over the pregenual and dorsal anterior cingulate cortex when electrodes were placed over the bilateral occipital lobes for patients with fibromyalgia. Studies that applied tDCS over the dorsolateral prefrontal cortex, a brain region that has been considered to be part of the ventral/dorsal attention network, showed a more diverse pattern of rsFC modulation. For instance, Sotnikova et al 57 found that the dorsal attention network was modulated in patients with ADHD, while the ventral attention network was modulated in patients with schizophrenia and substance abuse.51,53
At the whole-brain level, Wu et al 63 identified an increase in EEG coherence after applying stimulation over the left dorsolateral prefrontal cortex among 5 patients with disorders of consciousness. In contrast, another study of a larger sample size conducted by Schoellmann et al 55 found no significant differences between active and sham tDCS groups in rsFC, as indicated by imaginary corticocortical coherence across beta frequency bands among patients with Parkinson’s disease.
Regarding the correlation between rsFC changes and clinical outcomes, 14 studies involved clinical assessments as their outcome measures (Table 1), with 7 out of 14 studies reporting a significant correlation between rsFC changes and clinical outcomes, 2 out of 14 of studies reporting a nonsignificant correlation, and 5 out of 14 studies did not report such correlation as such analysis was not planned in their studies (Tables 2 and 3).
Effects of different tDCS parameters on changes in rsFC
Meta-regressions reveal a statistically significant, positive relationship between current density and changes in rsFC (B = 2.01, SE = 0.794, P < .05; Figure 4). Meanwhile, total stimulation does not appear to modulate changes in rsFC, as indicated by a non-significant correlation between these 2 factors (B = 0.0014, SE = 0.0015, P < .35; Figure 5). Of note, due to the limited number of studies available and the marked heterogeneity across studies, these observations should be interpreted with caution.

The relationship between tDCS current density and its modulatory effects on rsFC.
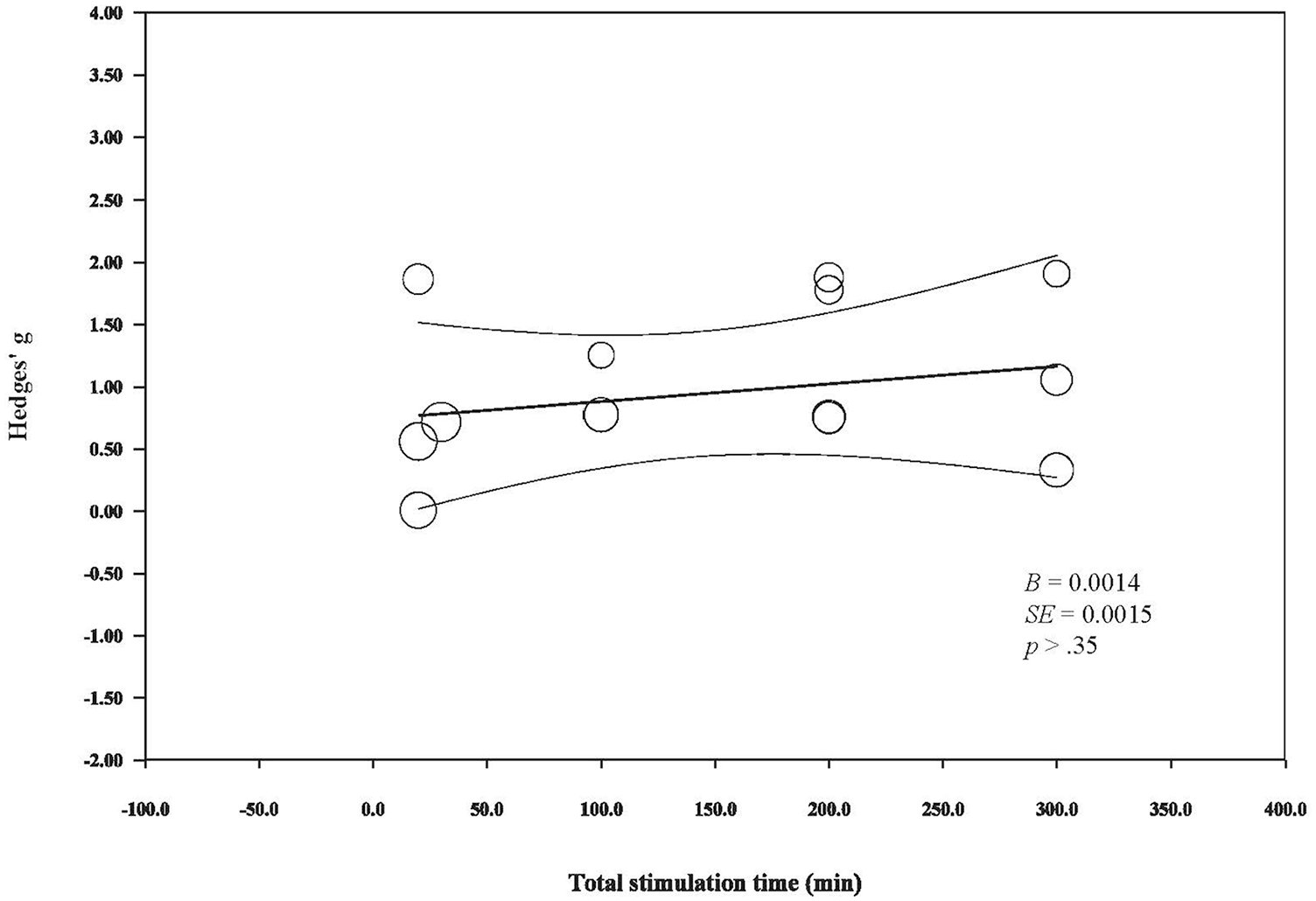
The relationship between tDCS total stimulation time and its modulator effects on rsFC.
Regarding the effects of stimulation type on rsFC, both anodal and bilateral stimulation were found to enhance rsFC, while cathodal stimulation resulted in mixed findings. For instance, when cathodal stimulation was given to patients with schizophrenia, the rsFC of the DMN increased and rsFC in the ventral attention network was reduced. However, the beta coherence was found to be higher than that of the sham-stimulated group in another study. 60
Risk of bias across studies
The funnel plot (Figure 6) showing the effect sizes of both EEG and fMRI studies plotted against standard error was asymmetric, which illustrated the presence of publication bias. Egger’s test was highly significant (P < .01, 2-tailed), which was a clear indication of a small-study effect.

A funnel plot for the inspection of publication bias across studies.
Discussion
This systematic review aimed to investigate the effectiveness of active tDCS in modulating resting-state functional connectivity among individuals with neurological disorders. By conducting a comprehensive literature search using multiple electronic databases and performing manual searches in reference lists of previously published papers, 15 RCTs with either crossover or parallel group designs, comparing active tDCS with sham stimulation, that also reported between-group resting-state functional connectivity results were included. In conclusion, this systematic review indicated 2 main points. First, the currently available neurophysiological and neuroimaging studies provided some evidence that active tDCS can induce changes in both localized (ie, brain regions under the transcranial electrodes) and diffused (ie, brain regions not directly stimulated by the transcranial electrodes) rsFC. Interestingly, fMRI studies showed that the DMN was enhanced regardless of patients’ diagnoses, the stimulation paradigms used or the rsFC analytical methods utilized. Second, stimulation intensity, but not duration, appeared to positively influence the effect of tDCS on rsFC.
Effects of tDCS on functional connectivity
Despite the great heterogeneity in the rsFC analytical methods used among studies included in this review, the data provided converging evidence that tDCS is effective in modulating rsFC in patients suffering from various kinds of neurological disorders. For instance, rsFC was not only found to be modulated in the local brain network where the electrodes were placed, but a network that encompasses brain regions not directly stimulated by the electrodes also exhibited alterations in rsFC. Consistent with previous studies that investigated the rsFC effects of tDCS in healthy individuals, 64 we demonstrated that tDCS is capable of inducing network-based effects in patients with various kinds of neurological disorders. Given that many neural functions are supported by functional networks rather than a particular brain region 29 and functional impairments among people with neurological disorders are usually found to be influenced by the disordered connectivity, 16 the network modulatory effects engendered by tDCS can serve as an important rationale that supports the clinical use of such neurostimulation techniques. Regarding the clinical relevance of rsFC, of the 9 papers that reported relevant data for analysis, the majority of studies showed a significant correlation between rsFC and clinical outcome changes. This observation lays a preliminary foundation for future studies to regard tDCS as a clinically relevant and effective technique for the betterment of patients with neurological disorders.
Possible physiological and biophysical mechanisms of tDCS in functional connectivity modulation
As evident from the EEG studies, enhancement in local rsFC (ie, rsFC confined to the stimulated brain regions only) induced by anodal tDCS were particularly reflected in the higher frequency bands (ie, beta and gamma) but not in the lower (ie, delta, theta, alpha) frequency bands, in which these findings are in line with the results from previous studies in healthy individuals during task-based FC studies 65 and animal studies. 66 The rsFC enhancement particularly at the higher frequency bands might be an important finding supporting the effects of anodal tDCS on local inhibitory network activity. Previous study reported that anodal tDCS applied over the primary motor cortex reduce local gamma-aminobutyric acid (GABA) concentration 67 over the stimulated brain region, of which GABA concentration was negatively correlated with rsFC in the somatomotor network.35,68 Interestingly, synaptic activities at the GABA type A (GABAA) receptors was found to be positively associated with beta peak frequency 69 and gamma power, 70 but not for other frequency bands, in which both beta/gamma peak frequency 71 and gamma power 72 around the anodal electrode have been found to be reduced by tDCS over the primary motor cortex. Importantly, our results further show that the rsFC enhancement effect by anodal tDCS does not limit to studies that applied anodal stimulation over the primary motor cortex but those applying tDCS over other brain regions (ie, prefrontal/occipital cortex). These studies and our results collectively postulate that, anodal tDCS suppresses local inhibitory synaptic network activity to bring about network-level changes (ie, enhancement in rsFC). Further studies are warranted to validate the relationships between GABA synaptic activity, beta/gamma oscillatory power/frequency, rsFC and anodal tDCS applied beyond the primary motor cortex, the negative association between beta/gamma power and peak frequency with beta/gamma functional connectivity, as well as to investigate the physiological mechanisms of cathodal tDCS stimulation.
Our review presented studies showing enhancements in the resting-state networks that were functionally connected to the stimulated brain region. For instance, stimulation in the primary motor cortex resulted in changes in rsFC within the somatomotor network, 54 while stimulation at the IFG resulted in changes in the dorsal attention network. 51 In line with the GABA hypothesis, increasing evidence, although limited to the somatomotor network, has shown that tDCS could enhance the connectivity of highly correlated brain regions that were associated with the local GABA reduction at the stimulated site.64,73 Surprisingly, all of the included studies showed the enhancement of the DMN, a resting-state network that has been found to be anti-correlated with task-based networks such as the somatomotor and ventral/dorsal attention networks, 74 regardless of the differences in tDCS protocol and patients’ diagnoses between studies. It might be possible that local beta/gamma oscillation enhancement modulates long-range functional connectivity. 75 It might also be possible that tDCS induces consistent electric fields not only limited to the coverage of the electrodes but also far from the electrodes. A computer simulation study that estimated the electrical field changes for different montage placements also indicated that the medial brain structures, where most of the key DMN regions are situated,40,76 exhibited consistent strength and direction of the electric field regardless of the mode of stimulation and electrode placements whether it was placed at C3, C4, F3, or F4. 77 Furthermore, a recently published study has shown that tDCS-induced changes in rsFC within and between networks appear to be related to the electric field strength over the targeted brain regions. 73 Therefore, it is conceivable that that the neuromodulatory effects on DMN may be results of the electrical fields generated in the brain by tDCS over the intended target. Future studies investigating spatial specificity are needed to verify this speculation and to elucidate the complex interaction between electrical field intensity and modulation of rsFC by tDCS.
Factors contributing to the differential tDCS rsFC effects
We inspected how current density and stimulation time affect tDCS rsFC outcomes by conducting meta-regressions and showed that current density, but not total stimulation time positively and linearly affect the rsFC effect by tDCS. In line with the discussion that the electric field is associated with the observed rsFC effects, given that the current density is directly proportional to the electric field as defined by Ohm’s law (
Limitations
As planned, we conducted a systematic review to summarize the current research trends in EEG and fMRI research that investigates the effects of tDCS on functional connectivity among people with neurological disorders. However, some limiting factors hinder us from giving a firm conclusion regarding the effects of tDCS in modulating rsFC. First, it should be noted that the number of previously published papers relevant to this topic, as well as for the respective brain diseases, is limited. Second, the marked heterogeneity among available studies, including differences in clinical diagnoses and gender of participants, variations in study outcomes and methodological issues such as tDCS protocol, could mediate patients’ responses to tDCS. Third, as our understanding of neurological disorders are still evolving, the etiology of some disease groups included in our review (ie, inflammatory bowel disorder 50 ) might not be considered strictly neurological. Further empirical studies investigating tDCS effects on rsFC in brains with specific neurological diseases, how gender difference mediates tDCS effects and how various tDCS treatment protocols modulate the brains differentially, are warranted to address these questions; due to the inherent variations in brains with various neurological disorders, further studies on healthy brains will also be helpful for us to understand the modulatory effects of tDCS on rsFC. In addition, the possible underestimation of the effect sizes for some studies in which P-values could only be assumed for the calculation of effect sizes. We have taken several measures to minimize such effects and to avoid misinterpretation. For instance, we did not attempt to provide a summary estimate of the effect; the forest plot we presented showed the maximum confidence intervals (ie, 99%) of g for each study. Moreover, incomplete reporting of some of the primary studies may pose another limitation. Although we have contacted the authors of eligible studies to obtain additional information on unreported or missing data, some research data remained unavailable for our analyses. Specifically, between-group rsFC differences were not reported in 3 of the primary studies, we had to exclude these studies as a result. Additionally, the analysis for clinical relevance was not completed as over 30% of reports omitted the necessary data. To scrutinize this issue, we suggest that future studies can minimize the risks of bias by reporting both significant and nonsignificant results as planned in the methods, as well as investigate and report the brain-behavior relationship, which is particularly essential for the development of advanced and effective evidence-based treatments for the betterment of this group of patients.
Conclusion
To the best of our knowledge, this is the first systematic review that investigates the tDCS effects on rsFC among patients with neurological disorders. Here we provide some evidence that tDCS can enhance rsFC, which is correlated with functional enhancements. Preliminary observations also support that higher current density contribute to greater rsFC changes. We recommend that future studies could investigate the effect of tDCS on rsFC, especially for cathodal stimulation. For clinicians, we suggest that anodal stimulation at a higher stimulation intensity, which is within the safety limit, might maximize tDCS effects in modulating aberrant functional connectivity, a shared problem among patients with different neurological diagnoses that contribute to the manifestations of their physical/cognitive dysfunctions.
Supplemental Material
sj-docx-1-cns-10.1177_1179573520976832 – Supplemental material for The Effect of Transcranial Direct Current Stimulation in Changing Resting-State Functional Connectivity in Patients With Neurological Disorders: A Systematic Review
Supplemental material, sj-docx-1-cns-10.1177_1179573520976832 for The Effect of Transcranial Direct Current Stimulation in Changing Resting-State Functional Connectivity in Patients With Neurological Disorders: A Systematic Review by Melody MY Chan and Yvonne MY Han in Journal of Central Nervous System Disease
Supplemental Material
sj-docx-2-cns-10.1177_1179573520976832 – Supplemental material for The Effect of Transcranial Direct Current Stimulation in Changing Resting-State Functional Connectivity in Patients With Neurological Disorders: A Systematic Review
Supplemental material, sj-docx-2-cns-10.1177_1179573520976832 for The Effect of Transcranial Direct Current Stimulation in Changing Resting-State Functional Connectivity in Patients With Neurological Disorders: A Systematic Review by Melody MY Chan and Yvonne MY Han in Journal of Central Nervous System Disease
Footnotes
Acknowledgements
We thank Miss Kris Chan, Mr Marco Cheng, Mr Alex Chu, Mr Paul Hui, Mr Eddie Li, and Ms Michelle Cheung for their efforts in supporting the study inclusion and data extraction processes.
Author Contributions
MC designed the study, performed literature search and screening, conducted statistical analysis, interpreted the data and drafted the manuscript. YH contributed to the conception of the study and assisted with study inclusion, data extraction and data interpretation. All authors read and approved the final manuscript.
Funding:
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was partly supported by the Health and Medical Research Fund [HMRF06173096] from the Health and Medical Research Fund, the Food and Health Bureau, The Government of the Hong Kong Special Administrative Region.
Declaration of conflicting interests:
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.