
Abstract
Background:
Fingolimod, an oral drug used in multiple sclerosis (MS) treatment, exerts its action through S1P-receptor engagement. These receptors are also expressed in heart and endothelial cells. The engagement of receptors on the atrial heart myocytes may cause a slowing effect on heart rate (HR). We aimed to explore the acute effect of fingolimod on the cardiac autonomic control, a side-effect of the drug that still needs to be clarified.
Methods:
In 10 MS patients, we investigated the influence of the first administration of fingolimod (0.5 mg) on sympathetic and parasympathetic indexes via the analysis of the HR variability, and on the baroreflex sensitivity via sequence and alpha coefficient techniques.
Results:
Fingolimod produced an average HR maximal drop of 12.7 (7.8) beats/min and the minimal HR occurred after 2.73 (0.38) hours from the dose administration. The pulse interval (PI) mean value and the pNN50 and RMSSD indexes of parasympathetic drive to the heart significantly increased. Interestingly, in 6 out of 10 patients also the power in the low-frequency band (LF) increased. The baroreflex sensitivity was not modified by the first dose of the drug.
Conclusions:
Our findings indicate that although the first dose of fingolimod invariably activates the parasympathetic system, in several subjects, it may induce also a surge in the sympathetic cardiac drive. This suggests that not only the vagal, as usually assumed, but also the sympathetic autonomic branch should be considered in the risk profile assessment of MS patients starting treatment with fingolimod.
Introduction
Multiple sclerosis (MS) is a very relevant cause of disability in adults. Fingolimod is an oral agent developed as disease-modifying therapy for patients affected by MS, 1 and it is widely used in patients with the relapsing remitting form (RRMS) with high disease activity or suboptimal response to other treatments.
Its efficacy was established in clinical trials2-4 and its use in clinical practice progressively increased. Evidence from the real world, gathered in unselected patient populations, confirmed the mid- and long-term effects of this drug on a large variety of end points, in terms of effectiveness and safety.5,6
However, in clinical practice, clinicians have to face with occasional significant cardiovascular effects after the first-dose administration. In phase 1 studies on healthy subjects, some cases of marked bradycardia were observed, 7 whereas in clinical trials, a slowing of atrioventricular conduction and onset of first- or second-degree atrioventricular blocks were documented in MS patients. 8 In clinical studies, most of these events were asymptomatic and transient, usually occurred in the first 6 hours following the first administration of the drug and did not recur throughout the continuation of the treatment. However, a case report of 7.5-second asystole was published 9 and a patient died after a single dose of fingolimod. 10 The European Medicines Agency promptly revised the recommendations regarding cardiovascular monitoring after the administration of the first dose of fingolimod. 11 In addition, a subsequent sudden death of a subject in the fifth month of treatment, likely due to arrhythmia induced by autonomic dysfunction, 12 led to limitations on the use of fingolimod in MS patients with cardiological comorbidities. A case of ventricular tachycardia after 15 days of fingolimod treatment was recently reported. 13 In addition, a moderate reduction of left ventricular systolic function was also observed, in subjects with previous or concomitant cardiac disorders. 14 At present, several cardiovascular conditions are considered as absolute contraindications: history of recent myocardial infarction, unstable angina, stroke, transient ischemic attack, decompensated heart failure, history or presence of Mobitz type II second- or third-degree atrioventricular block or sick sinus syndrome (unless patient has a functioning pacemaker), baseline QTc interval ⩾ 500 ms, and treatment with class Ia or III anti-arrhythmic drugs.
Mechanisms of action
The structure of fingolimod is similar to sphingosine, a lipidic component of cellular membranes. After oral intake, it is phosphorylated and the engagement of sphingosine 1-phosphate (S1P) receptors becomes possible. S1P mediates diverse physiological functions, as lymphocyte recirculation, neurogenesis, neural cell migration, natural killer cell migration,15,16 angiogenesis and vascular maturation, 17 endothelial cell function, and regulation of the vasomotor tone. 18 The S1P receptors are widely and differentially expressed in many tissues including the cardiovascular system. 19 The engagement of receptors on the atrial myocytes in the heart by fingolimod causes a slowing effect on heart rate (HR), 20 mediated by S1P1 and S1P3. Repeated administration of fingolimod results in internalization and degradation of the S1P receptors and has minimal or no effect on HR due to cessation of signaling. 21 Bradycardia may reappear if the drug is re-administered more than 2 weeks after its discontinuation. 22
Interestingly fingolimod has been shown to reduce the myocardial injury induced by reperfusion after ischemia, to decrease the infarct size and to improve left ventricular ejection fraction after myocardial infarction in a porcine model. 23
Fingolimod vs cardiovascular autonomic control
Previous studies have shown that the pretreatment assessment of the parasympathetic heart response to Valsava maneuver and deep breathing may be predictive of the bradycardic effect after the first fingolimod dose and its possible prolongation over time (ie, beyond 6 hours).24,25 A negative correlation was also observed between pretreatment noninvasive indices of sympathetic activation and the fingolimod-induced PR interval lengthening in the electrocardiogram (ECG) tracings. 24 These studies make it clear that the pretreatment autonomic profile of the patient may influence the first-dose effects of fingolimod.
In addition, it was reported that noninvasive indices of parasympathetic heart regulation averaged over 24 h time windows increase at the day of the first-dose administration with respect to pretreatment, whereas sympathetic control tends to prevail after 3 months of continuous fingolimod treatment. 26 The enhancement in cardiac parasympathetic regulation starts 1 hour after the first dose of fingolimod, by the analysis of HR variability through a continuous ECG, as assessed by ECG, recording, 27 thus confirming previous findings. Much less clear is the effect of drug initiation on the sympathetic cardiac modulation. Indeed, 1 study observed that both the RRI power in the low-frequency band (LF) and the RRI low-frequency/high-frequency (LF/HF) ratio progressively lowered throughout the 6 hours, 26 whereas another study observed a temporary increase in the sympathetic autonomic modulation after 1 hour from the drug administration. 28
On the basis of those discordant findings, in this study, we aimed at further investigating the interaction between fingolimod and the autonomic cardiovascular control during the first 6 hours from the first dose.
For this analysis, we took advantage of data collected in the past from 21 patients affected by RRMS before treatment, at the first drug administration and after 6 months. We exploited those data in a previous study 29 to investigate how fingolimod treatment after 6 months can influence the autonomic heart control and the arterial baroreflex function. In a subgroup of 10 patients, we also collected data during the first 6 hours after the first dose. At that time, data referring to the acute effects of fingolimod were not considered and are exploited in this study.
Methods
The study was conducted in the Rehabilitative Cardiology and Multiple Sclerosis Units of Don Carlo Gnocchi Foundation, in accordance with the Helsinki Declaration. The study protocol was approved by the Ethics Committee of our institute. The patients signed an informed consent form (protocol number: 14/2014/CE_FdG/SA).
We analyzed the database reporting the results obtained on 21 subjects, 10 women and 11 men, affected by RRMS, consecutively recruited at the beginning of the fingolimod therapy, at the single daily dose of 0.5 mg.
We excluded patients affected by or with a past history of cardiac disease, with abnormal ECGs, or affected by respiratory or renal disease. All of them had at least 1 documented relapses in the past 12 months or at least 2 of them in the previous 2 years, with a score between 0 and 5.5 on the Expanded Disability Status Scale (EDSS), which can range from 0 to 10, with higher scores indicating greater disability. 30
Concomitant medications were monitored and registered. Details on the study population are shown in Table 1.
Baseline clinical characteristics of the patients.

Abbreviations: MS, multiple sclerosis; EDSS, Expanded Disability Status Scale.
Study protocol and measurements
At the day of the first fingolimod administration, the patient reached the Rehabilitative Cardiology Unit early in the morning. At 9:00
At the end of the session, the patients were discharged and were asked to periodically report to the Unit for medical checks. In each patient, the 12-lead ECG was assessed before beginning the fingolimod treatment (T0) and after 6 hours from the first drug administration (T6). From each ECG paper strip, PQ and QT intervals were measured. The QT HR correction (QTc) was also calculated by the Bazett formula.
In addition, ECG was also continuously monitored during the 6-hour observation period to detect any excessive decrease in the HR and possible prolongations in the PQ and QT intervals. In absence of alarms from the monitoring device, the HR value was annotated every hour.
In all patients, a 10-minute continuous finger arterial blood pressure (by Finometer; FMS, Amsterdam, The Netherlands) was measured at T0 to investigate the influence of fingolimod on the baroreflex and the other autonomic indexes hereafter specified. The Finometer finger cuff was placed around the middle finger of the right hand and kept at the heart level by a sling. All continuous blood pressure recordings were made while the subjects were in reclined position and were calibrated using the average of 3 manual measurements taken with a sphygmomanometer just before the monitoring.
In the first 10 patients, finger blood pressure was also continuously recorded throughout the 6-hour observation period to quantify the acute effects of the drug. From each pressure recording, we first identified the lowest HR value occurring within 3.5 hours from the start of the observation period, and for the subsequent analyses, we considered a 10-minute data segment centered around the time of occurrence, TOCC, of this lowest HR value. The 3.5-hour time limit was set because, after this period, the patients had the necessity to void, move, and eat, and those activities are known to induce autonomic responses that would have interfered with the assessment of the drug influence on the autonomic control.
Data analysis
Each finger pressure recording was segmented into individual pressure pulses; the systolic blood pressure (SBP) and diastolic blood pressure (DBP) were estimated as the maximal and minimal pressure values occurred in each beat, respectively. The length of cardiac cycle was calculated on a beat-to-beat basis by the pulse interval (PI), that is, the time interval between 2 consecutive systolic peaks. In the following, HR was derived from PI by the formula

Preliminarily to the analyses described in the next sections, the SBP, DBP, and PI mean value and standard deviation were estimated over each pressure recording at T0 and TOCC.
Estimation of autonomic indexes from the HR variability analysis
Autonomic indexes were estimated from the analysis of the PI beat-to-beat series. 30 We computed the pNN50 (ie, the percentage of normal beats differing for more that 50 ms from the preceding normal beat) and the RMSSD (ie, the root mean square of successive PI differences). Both these time-domain measures of HR variability are reported to be influenced by the parasympathetic control of the heart. We also estimated the spectral characteristics of the PI series via the fast Fourier transform (FFT). From each spectrum, the power density was integrated over the LF (0.04-0.15 Hz) and the HF (0.15-0.4 Hz) bands. 31 The power ratio between the power in the LF and HF bands (LF/HF) was also calculated.
The PI powers in the LF and HF bands are associated with the sympathetic and parasympathetic control on the heart, respectively, whereas the LF/HF ratio represents the sympathovagal balance. 32
Estimation of spontaneous baroreflex function
From the 10-minute finger pressure recordings made at T0 and TOCC, spontaneous baroreflex sensitivity (BRS) was estimated by the sequence 33 and the alpha coefficient 34 techniques.
The sequence technique
It consists in the identification of sequences of 3 or more consecutive cardiac beats in which a progressive increase in SBP is observed, followed by a progressive lengthening in PI (PI+/SBP+ sequences) with a 1-beat delay, or, on the contrary, progressive decreases in SBP are followed by a progressive shortening in PI (PI–/SBP– sequences). The slope of the regression line between the SBP and PI values included in each sequence is taken as a local estimation of BRS, as done when SBP and PI changes are induced by vasoactive drug injections.33,35 A previous study in animals demonstrated the baroreflex nature of these spontaneous PI/SBP sequences. 35 In this study, we considered sequences of 3 or more consecutive heart beats in which beat-to-beat SBP and PI changes were at least 1 mm Hg and 5 ms, respectively. For each recording, a single BRS value was obtained by averaging the local slopes of all sequences occurred within the whole data set.
The alpha coefficient technique
This second technique for the BRS estimation is based (1) on the splitting of SBP and PI beat-to-beat series into short-term data segments, (2) on the subsequent computation of the spectral characteristics of each data segment by the FFT, and (3) on the final computation of the squared ratio of the PI and SBP spectral powers in the LF (alphaLF) and HF (alphaHF) bands, whenever the squared coherence modulus between PI and SBP was >0.5. These alpha coefficients are considered as 2 additional indexes of spontaneous BRS. 34
The Baroreflex Effectiveness Index
The baroreflex effectiveness in controlling the HR, aside from the baroreflex sensitivity, was evaluated using the Baroreflex Effectiveness Index (BEI), 36 defined by the formula

where the “total number of PI/SBP sequences” is the sum of both PI+/SBP+ and PI–/SBP– sequences with a time delay between the SBP and PI changes of 0, 1, and 2 heart beats and threshold values of 1 mm Hg and 5 ms; and the “total number of the SBP ramps” is the sum of ramps of 3 or more consecutive beats in which SBP progressive increase (SBP+) or progressive decrease (SBP–) for more than 1 mm Hg, independent of whether they are or are not followed by PI changes. We estimated BEI index to quantify the possible fingolimod influence on the effectiveness of the baroreflex in getting the control of the sinus node.
Statistical analysis
Results are expressed as mean (standard deviation) unless otherwise indicated. The Kolmogorov-Smirnov test was used to verify the normality of the distribution of the variables. Only the pNN50 did not pass the test, and its values were log-transformed before the statistical analysis.
To verify the acute and mid-term effects of fingolimod on the variables, we evaluated the statistical significance of the difference in their values at T0 vs TOCC using the 2-tailed paired t-test. A P-value < 0.05 was considered statistically significant.
Results
Over the whole group of 21 patients, fingolimod produced an average HR maximal drop of 12.7 (7.8) beats/min. Individual absolute HR drop values are reported in Figure 1, whereas the frequency distributions of drop magnitudes are shown in Figure 2. The bradycardic effect was transient; after 6 hours, only a minority of patients (19%) still presented a HR significantly lower (more than 20% less) than at T0.

Maximal bradycardic effect of the first fingolimod dose. Details of the maximal bradycardic effects of the first dose. Individual heart rate values at T0, at the moment of maximal bradycardia and at the end of the 6 hour observation period.

Frequency distribution of the heart rate drop with respect to baseline. The drop levels have been categorized as follows: low (0-10); medium (11-20); high (21-30); and very high (>30) beats/min.
As indicated in Table 2, SBP and DBP did not change from T0 to TOCC. The PR interval remained within the normal range (<0.20) in all subjects with only a small and not significant increase after 6 hours after first drug administration from 0.16 (0.02) seconds to 0.17 (0.02) seconds. The QT interval substantially remained at the baseline value (0.37[0.03] seconds) after the 6-hour observation period (0.39[0.02] seconds).
Changes induced by the first dose of fingolimod on blood pressure, cardiac rhythm, indexes of cardiovascular autonomic control, and baroreflex function.
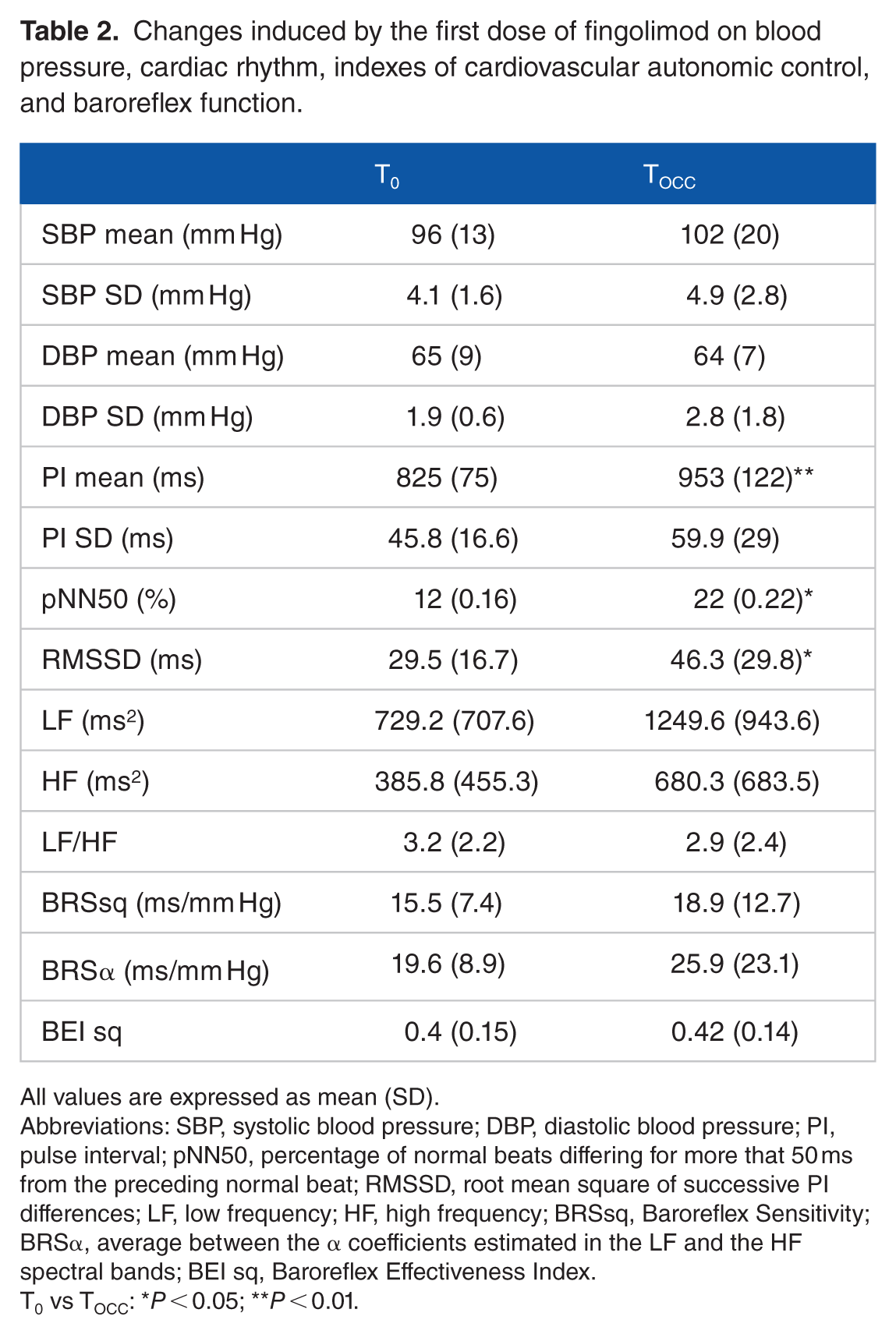
All values are expressed as mean (SD).
Abbreviations: SBP, systolic blood pressure; DBP, diastolic blood pressure; PI, pulse interval; pNN50, percentage of normal beats differing for more that 50 ms from the preceding normal beat; RMSSD, root mean square of successive PI differences; LF, low frequency; HF, high frequency; BRSsq, Baroreflex Sensitivity; BRSα, average between the α coefficients estimated in the LF and the HF spectral bands; BEI sq, Baroreflex Effectiveness Index.
T0 vs TOCC: *P < 0.05; **P < 0.01.
Fingolimod autonomic effects
Results shown in the following sections refers to the subgroup of 10 patients and are obtained by a comparison of values observed at baseline (T0) vs TOCC (ie, the time of occurrence of the relative HR drop within 3.5 hours). On average, the relative HR drop occurred after 2.73 (0.38) hours from the dose.
Autonomic heart control
Table 2 also reports the values of the indexes of autonomic cardiac control at T0 and TOCC.
The pNN50 and RMSSD indexes of the parasympathetic drive to the heart significantly increased at TOCC. As shown in Figure 3, these indexes invariably rose in all subjects. Also, the average PI power in the HF band almost doubled (+80%) over the group, although this change did not reach the statistical significance.

Individual changes in the pNN50, RMSSD, and PI LF power at T0 and TOCC.
Interestingly, at TOCC, also the power in the LF band markedly increased on average (+71%) over the group. From Figure 3, it is apparent that this rise occurred in 6 out of 10 patients, indicating that the fingolimod first dose not only invariably activates the parasympathetic system but also, in several subjects, elicits the sympathetic drive to the heart.
Baroreflex function
We did not observe any significant change at TOCC, in the BRS value, either estimated by the sequence or the alpha coefficient techniques. Also, BEI index remained unchanged with respect to baseline.
Discussion
We observed that at the moment of maximal HR drop from the first dose, indexes of parasympathetic activity (pNN50 and RMSSD) significantly increased. This result indicates that the acute bradycardic effect of the treatment in most patients occurs as part of a wider parasympathetic activation, and this is in line with previous observations.26,27
In addition, we also observed that in a number of subjects, the drug actually produced a generalized autonomic surge involving not only the parasympathetic but also the sympathetic systems.
The latter finding may be interpreted as a further evidence of the complex interrelation between fingolimod and autonomic cardiac control. Focusing on the parasympathetic response, previous studies24,25 suggested that the pretreatment autonomic profile of the patient influences the strength of his or her vagal response to the first administration of the drug. We may speculate that the same reasoning might be extended to the sympathetic response to the first dose. In this line, the only-parasympathetic or the combined parasympathetic-sympathetic response during the first administration of the drug might also depend on the individual autonomic profile.
Our results are in disagreement with what observed by Simula et al, 27 who found a decrease in sympathetic activity just after the first dose. On the contrary, our data are compatible with Hilz et al, 28 who found an increase in indexes of sympathetic activity in a time window from the first to the second hour after the dose. In our population, the moment of the maximal HR drop when we measured the sympathetic activity occurred after 2.73 hours, thus not too far from the time window observed by Hilz. At this time, we actually observed that the PI LF power when averaged over the whole group was importantly increased with respect to T0. However, as detailed above, the sympathetic surge actually occurred only in a subset of patients. The baroreflex function does not appear to be affected by the first dose, in spite of the parasympathetic activation.
Taking advantage of the results obtained in our previous study on the effects of a prolonged fingolimod treatment, 29 it appears that after 6 months of treatment, these patients displayed a significant decrease in the baroreflex sensitivity and effectiveness in getting the control of the sinus node, and an impairment in the parasympathetic and sympathetic cardiac control. The paradoxical results of increased autonomous activation in the acute phase of fingolimod are in contrast with the reduced autonomous activation in the chronic phase of fingolimod. This suggests that, independently from the acute response to the first drug dose, the prolonged treatment produces a global autonomic dysfunction, at least on the 6-month time scale. It is worth noting that a recent placebo-controlled MS trial with siponimod, 37 a more selective sphingosine receptor modulator, was conducted with a different strategy (dose titration) to prevent cardiovascular side-effects. Nevertheless, a significant proportion of patients treated with siponimod experienced side-effects or adverse events that has been associated with S1P-receptor engagement, such as bradycardia after the first dose and hypertension. These findings seem to confirm that sphingosine receptor modulation, while exerting a positive effect on MS course, needs a careful management on a cardiovascular ground.
Study limitations
This is an observational study and the results may have been partially affected by the small number of patients enrolled. It cannot be excluded that the increase in baroreflex sensitivity resulted not significant, due to the small sample size.
Conclusions
Our study indicates that in some subjects, the first fingolimod dose may enhance the sympathetic heart modulation in addition to the expected parasympathetic activation. This aspect should be considered in the risk profile assessment of MS patients starting the treatment with fingolimod.
Footnotes
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/ or publication of this article: The study was funded by a grant from the Italian Ministry of Health and the Don C. Gnocchi Foundation.
Author Contributions
VR: carried outconception and design of the study, design of the study, interpretation of data and drafted the manuscript
MR: carried out interpretation of the data and revised manuscript
RC: collected the data
EV: carried out statistical analysis
AT: collected the data
MDR: carried out interpretation of data and drafted the manuscript.