
Abstract
Multiple medication use, or polypharmacy, is common in people undergoing rehabilitation. Polypharmacy is also common in older people, where it has the potential to impact on habitual physical activity. Despite this, the interactions between medication, disease, activity, and rehabilitation outcomes are insufficiently researched. In this review, we consider common classes of medications that can affect physical activity levels and outcomes of rehabilitation. We consider medications that improve disease processes and improve limiting symptoms (eg, breathlessness in heart failure and lung disease, pain in arthritis), unwanted side effects of medications (eg, central slowing caused by opioids and hypnotics), and also medication classes that might have the ability to improve activity and rehabilitation outcomes via beneficial effects on neuromuscular function (eg, angiotensin-converting enzyme inhibitors). We conclude by giving practical advice on how to review and optimise medication use to support habitual physical activity and ensure the best results from rehabilitation.
Introduction
Older people are the group for whom rehabilitation is most often needed – often not only as a result of acute illness but also in response to chronic disease and functional decline. Maintaining function and habitual physical activity in older people is not only an important end in itself but also helps to protect against cardiovascular disease, diabetes, cancer, and dementia,1–3 which thus helps to protect against the decline in physical function that often accompanies old age.
There is excellent evidence that older people can benefit greatly from exercise programmes, 4 and many studies have shown that at least some older people are both willing and able to engage in exercise programmes. However, habitual physical activity is a construct that is distinct from exercise and is associated with benefits over and above those provided by exercise. Although exercise refers to planned, structured, repetitive activity performed for the purpose of improving fitness, habitual physical activity encompasses all movement during waking life. 5 Efforts to improve the volume or pattern of habitual physical activity in older people have proven much less successful.6,7 In part, this reflects an incomplete understanding of the barriers and drivers of physical activity in older people and the fact that multiple factors appear to be important – individual level factors such as health, motivation, attitudes, and pet ownership; societal factors such as interconnectedness and the views of those around us; as well as environmental factors such as weather, green space, and perceived safety of neighbourhoods.
One important area that has been understudied to date is the relationship between medication use and both the rehabilitation process and habitual physical activity in older people. Most of the older people have more than one disease (referred to as multimorbidity) and hence take multiple medications. 8 Just as some diseases may interfere with the ability to undertake physical activity (eg, arthritis, heart failure, or lung disease), it is plausible that some medications may either enhance or interfere with the ability to undertake physical activity or rehabilitation. In this article, we review the ways in which medications might either improve or inhibit physical activity or the rehabilitation process in older people, either by direct physiological effects or by their interactions with symptoms and disease states.
To construct this narrative review, we searched electronic databases (PubMed, Embase, CINAHL) for relevant articles, supplemented by handsearching of reference lists from selected articles and by our existing knowledge of the field as active researchers and practitioners in this area. We aim to highlight existing evidence on the effects of commonly used medicines on the ability of older people to undertake physical activity and engage with rehabilitation; we also aim to highlight where evidence is lacking. This knowledge will be of benefit to all members of the multidisciplinary team involved in both rehabilitation and the promotion of physical activity in older people.
In What Ways Might Medication Use Affect Rehabilitation and Physical Activity?
Medications that affect disease processes or symptoms
Many illnesses have the potential to reduce physical activity in older people, usually by dint of specific symptoms that limit exercise capacity, but also via indirect effects – limiting opportunities or creating barriers to undertaking physical activity. Some key examples that are common in older people are shown in Table 1.
Common illnesses in older age and mechanisms for potential reduction in physical activity.
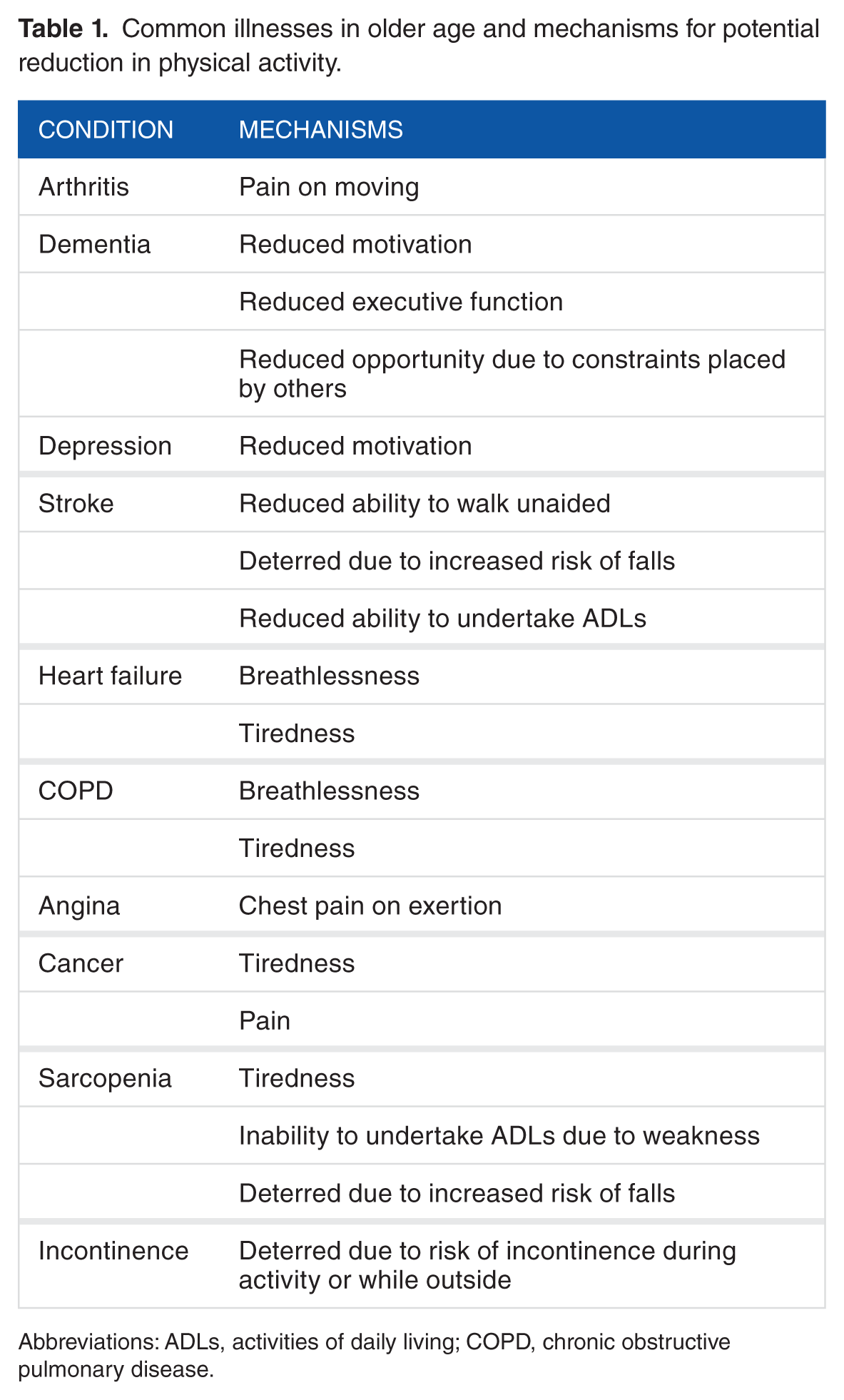
Abbreviations: ADLs, activities of daily living; COPD, chronic obstructive pulmonary disease.
For some conditions listed above, there is good evidence that medications aimed at relieving symptoms can improve exercise capacity. For instance, angiotensin-converting enzyme inhibitors (ACEi) improve exercise capacity in older patients with chronic heart failure, 9 inhaler therapy improves exercise capacity in chronic obstructive pulmonary disease (COPD), and antianginal medications improve walking distances in angina. However, simply improving exercise capacity may not necessarily translate to an improvement in habitual physical activity levels10,11; symptoms and illness, particularly when present for a long period of time, may lead to patients establishing patterns of reduced physical activity; and removal of symptoms may not always lead to a reversion to prior patterns of physical activity.
Conversely, medications have the potential to limit physical activity via worsening of existing symptoms – often as a side effect of treating another illness. Non-steroidal anti-inflammatory drugs (NSAIDs) are efficacious in treating the pain of osteoarthritis – but can also worsen fluid retention in patients with chronic heart failure, leading to increased breathlessness. Similarly, furosemide and other diuretics are effective at improving symptoms in heart failure, but this may be at the cost of worsening incontinence and urinary urge symptoms. This in turn may lead to activity restriction and a consequent reduction in physical activity.
Medication side effects that may impact on physical activity
A second important class of medication actions that may impact on physical activity are unwanted side effects. These are typically ‘off-target’ effects that are unwanted, in contrast to the effects discussed above where a beneficial effect on one body system may worsen problems in another body system or disease state. The range of side effects that medications can cause is vast, but 3 examples grounded in clinical experience will suffice to show the range of the problem:
Nausea. Medications such as iron, metformin, and chemotherapeutic agents can cause nausea, which may be worsened by movement. Such symptoms may dramatically reduce both the willingness and ability to undertake habitual physical activity.
Drowsiness. A common side effect across multiple medication classes, including opioids used for pain control, antidepressants, and anxiolytics, plus many medications with anticholinergic actions (eg, antihistamines given for allergies). Excessive daytime sleepiness is likely to reduce the ability to undertake physical activity.
Electrolyte derangement. Low potassium levels (commonly caused by diuretics) can lead directly to muscle weakness, impairing ability to undertake physical activity. Other electrolyte disturbances (eg, low magnesium caused by diuretics or proton pump inhibitors, low sodium from a wide range of drugs) can have similar effects on muscle function, drowsiness, and thus physical activity.
Potential off-target beneficial effects of medications on physical activity
Could some medications have beneficial effects on physical activity, over and above that expected from the relief of symptoms or diseases that reduce physical activity? One potential pathway by which such an effect might be mediated is via improvement in muscle function, particularly in the group of frail, older people with sarcopenia (the age-related decline in muscle mass and function 12 ). Such effects might be mediated directly or by enhancing the effects of training or rehabilitation on muscle function. A further potential mechanism by which beneficial effects might be seen is via enhancement of alertness and other central nervous functions such as volition and motivation. Potential candidate medications for all of these categories are discussed below.
What Evidence Exists?
Good quality evidence for the effects of medications on either rehabilitation outcomes or physical activity levels in older people is scanty. There is a particular dearth of evidence (both observational and interventional) regarding the interaction between medication use and habitual physical activity; similarly, little evidence exists on the relationship between activities of daily living (ADLs) and medication use. Alternative sources of evidence, particularly the effect of medications on physical performance (eg, endurance, strength, and balance) and falls risk can provide some insight, with the caveat mentioned above that an improvement in physical performance does not necessarily translate into an improvement in relevant rehabilitation outcomes such as ADLs and habitual physical activity.
Effects of Medications Used to Treat Selected Symptoms or Disease States
Chronic obstructive pulmonary disease
Although there is plenty of evidence to show that inhaler therapy (eg, β2-adrenergic agonists and muscarinic receptor antagonists) improves symptoms and exercise capacity in COPD, very few studies have attempted to evaluate the impact of these therapies on habitual physical activity. Two small uncontrolled Japanese studies have shown an improvement – use of the long-acting β-agonist indacaterol increased the number of steps taken per day by 16% over a 12-week period, 13 and optimisation of inhaled medication in a group of older patients with COPD (mean age: 71 years) was associated with an increase in moderately vigorous physical activity (≥3.5 metabolic equivalent tasks) but not in less vigorous physical activity. 14
Heart failure
Similar to COPD, there is good evidence that the major heart failure therapies (ACEi, angiotensin receptor blockers, β-blockers, and mineralocorticoid antagonists) all improve symptoms in heart failure due to reduced ejection fraction but have little effect in heart failure with preserved ejection fraction. Evidence for improvement in physical function is less clear; drug therapy does not appear to have benefit for patients with preserved ejection fraction, 15 but meta-analysis data confirm a small, but potentially useful improvement in exercise capacity for ACEi, 16 but not β-blockers 17 in patients with reduced ejection fracture. Data are lacking on whether these improvements in exercise capacity translate into increased levels of habitual physical activity, however.
For some patients, β-blockers can worsen symptoms of tiredness; available data on the impact of β-blockers on exercise training programmes for heart failure is reassuring, however, in that β-blockers do not appear to impair the benefit of exercise training on exercise capacity. 18
Depression
Anecdotally, depression is a well-known barrier to engagement with the rehabilitation process and is a particular problem for patients undergoing inpatient rehabilitation. Depression itself is associated with an increased risk of falls, 19 likely due to a combination of slowed central processing and reduced activity levels leading to deconditioning. Evidence for the effectiveness of antidepressant medication in improving rehabilitation outcomes is difficult to find, however. A recent randomised controlled trial of venlafaxine versus placebo in patients with depressive symptoms after spinal cord injury showed improvements in both depressive symptoms and disability using the Sheehan scale after 12 weeks of therapy. 20 Care is required; however, antidepressant use is associated with an increased risk of falls 19 independent of the depressive illness, and certain types of antidepressants have significant side effects including impaired levels of alertness and neuromuscular function, sedation, insomnia, and confusion 21 that could potentially reduce ability to engage with rehabilitation. Apathy has also been reported as a side effect of some antidepressants, particularly selective serotonin reuptake inhibitors 22 ; it is unclear how much of a problem this side effect causes in clinical practice, however.
The evidence for the use of antidepressants (specifically serotonin-specific reuptake inhibitors [SSRIs]) in patients recovering from stroke is somewhat stronger; systematic review data 23 suggest that in this situation, SSRI use may lead to both reduced disability and reduced dependency; these benefits may not be solely due to effects on depressive symptoms, and a series of large trials is now underway to confirm these findings. 24
Low motivation and reduced alertness can interfere with rehabilitation even in the absence of a formal depressive disorder. Medications such as modafinil and amphetamine derivatives have been used in other settings (eg, combat zones or examination revision) to increase wakefulness and alertness. A recent small trial (n = 41) investigated the treatment of post-stroke fatigue with the wakefulness promoting drug modafinal. 25 The primary end point, the multidimensional fatigue inventory-20 general fatigue score, did not differ between groups at follow-up. Patients in the modafinil group did, however, obtain better scores on the Fatigue Severity Scale and in some subscales of a stroke-specific quality of life questionnaire (P < .05). Larger studies are required in this area, need to include patients preselected for low motivational or alertness, and need also to study those patients without stroke as the reason for requiring rehabilitation.
Pain
The relationship between pain and habitual physical activity is complex; higher levels of pain are associated with lower levels of objectively measured physical activity, 26 but the perception that patients have of how pain affects physical activity levels may not correlate with the impact of pain on physical activity when measured objectively. 27 In addition, the relationship between pain and physical activity appears much stronger for self-reported physical activity measures than when objective measures of physical activity are used. 28
Both opioid and non-opioid analgesics are associated with a myriad of side effects. Opioids cause constipation, can worsen cognition, precipitate delirium, and increase the risk of falls 29 ; similar problems with falls and cognition are seen with neuropathic agents including pregabalin, gabapentin, carbamazepine, and amitriptyline. Non-steroidal anti-inflammatory drugs bring their own set of side effects including gastrointestinal bleeding, hypertension, fluid retention, and renal dysfunction – problems of particular importance in older people. Care is required to minimise the dose of analgesia and to monitor closely for side effects.
With the above caveats, however, analgesics can be effective – clearly pain relief is a valuable aim in itself, but effective analgesia can also improve both rehabilitation outcomes and physical activity. Activity as measured by actigraphy increased significantly in patients with osteoarthritis treated with the NSAID celecoxib when compared with placebo, 30 and regular administration of tramadol, when compared with as required use, was associated with better physical function on the Functional Independence Measure at discharge after hip fracture surgery. 31
Anaemia
Severe anaemia can cause tiredness and breathlessness and undoubtedly reduces both activity and the ability to engage with rehabilitation. In such cases, correction of the underlying pathology (eg, peptic ulcer) and replacement of nutrients (eg, iron, B12) are required. Many older people have a mild, chronic anaemia, and while this is commoner in patients with poor exercise capacity, there is little evidence that correction with iron is helpful. Oral iron has very little effect on haemoglobin levels (a mean increase in 0.35 g/dL was seen in a recent meta-analysis 32 ) and can cause significant constipation and nausea and is ineffective in cases of anaemia due to chronic disease. Intravenous iron may be better tolerated, and in patients with heart failure and low iron levels, it is effective at improving both 6-minute walk distance and quality of life. 33 Evidence that iron improves functional measures in patients without heart failure is, however, lacking.
For some other diseases or symptoms (eg, incontinence), the effect of medications to treat incontinence on habitual physical activity does not appear to have been studied. Incontinence is a predictor of poor outcomes from rehabilitation 34 and can contribute to the need for institutional care for many patients. It is not clear, however, how use of medications to treat incontinence affects the rehabilitation process. On one hand, effective treatment of incontinence might be expected to improve participation in daily activities including the rehabilitation process, as well as improving mood due to relief of stigmatising symptoms. Conversely, many medications used for urinary incontinence have anticholinergic side effects, which might impair cognition, reaction times and hence impair the ability to engage with rehabilitation.
Medications That May Affect Function Independently of Specific Disease Processes
Medications influencing the pathophysiology underlying sarcopenia have the potential to both enhance the rehabilitative process (by accelerating recovery from exercise) and improve physical activity levels by improving physical function. Although the pathophysiology of sarcopenia is incompletely understood, 12 a number of contributory processes may be amenable to pharmacological manipulation.
Oxidative stress has adverse effects on mitochondrial function in muscle; inhibitors of excessive oxidative stress may therefore provide a way to combat sarcopenia. Older patients taking allopurinol (a powerful inhibitor of xanthine oxidase, which generates reactive oxygen species) had better outcomes from inpatient rehabilitation as measured by the 20-point Barthel Index than those not taking allopurinol. 35 Observational studies such as this cannot, however, dissect out the effect of the medication from the effects of the underlying condition (gout) for which treatment is given. Randomised controlled trials are required to do this, which are now underway. 36
The renin-angiotensin-aldosterone system has also been implicated in sarcopenia. Observational data suggest that patients taking ACEi have a slower decline in walk speed over time, 37 although no effect on change in grip strength was seen in healthy older adults. 38 Randomised controlled trial data suggest that in some frail older adults, perindopril (an ACEi) can significantly improve exercise capacity as measured by the 6-minute walk test, 39 although this effect was not evident in a group of older people already undergoing exercise training 40 or in a group of relatively robust older adults. 41 Interestingly, neither ADLs, as measured by the Nottingham scale, nor habitual activity, as measured by triaxial accelerometry, improved with perindopril despite the improvement in exercise capacity.
Vascular disease has also been linked with sarcopenia and muscle weakness in older people, suggesting that other medications with beneficial effects on vascular health might benefit activity levels and rehabilitation outcomes. Statins remain the centre of great controversy; they are undoubtedly effective at reducing vascular events such as myocardial infarction and stroke; they are also effective at improving exercise capacity in those with peripheral vascular disease. 42 However, statins can cause myopathy, although the cause, frequency, and severity of this myopathy are still fiercely debated. Two observational studies in older patients undergoing inpatient rehabilitation43,44 suggest that statin use is associated with improved rehabilitation outcomes; it is not clear whether this reflects direct effects on vascular function, a reduced risk of vascular or inflammatory events and hence less interruption to rehabilitation, or simply residual confounding; those taking statins may simply be less frail than those not taking statins despite attempts to adjust for this. Self-reported physical function using 36-Item Short Form Health Survey (SF-36) subscales was better in statin users in 2 cohorts of older women, although no difference was seen in objective measures of physical performance.44,45 Conversely, a large longitudinal analysis from the Osteoporotic Fractures in Men study suggested that those taking statins had slightly lower (5 minutes per day) levels of moderate physical activity as measured by accelerometer than those not taking statins, 46 and an analysis of functionally impaired participants in the Lifestyle Interventions and Independence for Elders trial 47 showed that statin use neither augmented nor interfered with the exercise programme. A recent randomised controlled trial in healthy young adults (mean age: 44 years) showed no difference in objectively measured physical activity between those receiving 6 months of atorvastatin 80 mg and those receiving placebo 48 ; it is perhaps unsurprising that no improvement was noted in this healthy group, but the lack of deterioration in activity levels suggests that significant statin-mediated declines in function may be uncommon even at this high dose of statin.
Figure 1 illustrates the effects of some oral drugs on muscle function and emphasises how the clinician must carefully weigh up the pros and cons of prescribing certain medications.

Pathways by which medications may affect physical activity (PA) and rehabilitation.
Medications That May Affect Physical Activity by Improving or Worsening Other Symptoms
Hypnotics and anxiolytics
Both benzodiazepines and the so-called ‘Z-drugs’ (such as zopiclone and zolpidem) have potential adverse effects, particularly in older people. Drug effects may last well into the day after taking such medications, and the reduction in central cognitive processes leads to a 4-fold increase in the risk of falls in those taking such medications. 49 In long-term use (more than 3 weeks), such medications do not increase the amount of sleep, and sleep quality is often suboptimal.
Withdrawal of such medications may therefore improve ability to engage with rehabilitation and lead to improved physical function. Although the effect of such medications on habitual physical activity is not known, a group of older patients who successfully withdrew from these medications showed improvement not only in Berg balance scores but also in handgrip strength over a period of several months. 50
Anticholinergic medications
Anticholinergic side effects may go unrecognised in the older adult population; they can be insidious and might be attributed to ageing or disease. Symptoms may include insecure movement, falls, blurred vision, and increased anxiety; anticholinergic medications may worsen cognition, 51 particularly in those patients (eg, those with Alzheimer disease) who already have compromised central cholinergic neurotransmission. Older adults are at increased risk of anticholinergic side effects and part of the reason is due to deficient drug metabolism and elimination, as well as age-related deficits in cholinergic neurotransmission. 52
Anticholinergic burden is associated with poorer physical function and impaired ADLs (eg, as measured by chair stands, walk tests, and the Barthel Index),53,54 but it is less clear how much of this association is due to anticholinergic drugs and how much to associated disease and frailty. What is currently lacking is evidence that reducing anticholinergic burden leads to improvement in function, improvement in engagement with rehabilitation, or improvement in habitual physical activity. 55
Practical Advice
How then might practitioners and patients seek to optimise medication use so as to facilitate the rehabilitation process and enhance habitual physical activity? The principles of appropriate prescribing for older people, as exemplified by the Scottish guidelines on prescribing for older people, provide a practical template that can help optimise prescribing. 56 Entry into a rehabilitation programme, whether in hospital or in the community, provides a good opportunity to review current medication use. Key issues to consider in the context are shown in Table 2. Much of the existing evidence base available to guide practice is comparatively weak; as the examples discussed above show, much evidence comes from observational studies, and the few randomised controlled trials available are mostly small, with a limited range of relevant outcome measures. The evidence base available within stroke rehabilitation is slightly better, but even here, evidence is patchy. An understanding of pharmacology can complement the available evidence from trials and other clinical studies; quite often, however, simply starting or stopping a medication and observing the impact carefully are not only necessary but also may be the only way to proceed.
Issues to consider when undertaking medication review in rehabilitation.

Conclusions
Medication use in older people is common, particularly among older people with multiple diseases, who tend to have the lowest levels of physical activity and who are the main users of rehabilitation services. A better understanding of the effects of medications on activity and rehabilitation could therefore help to enhance outcomes older people – by better treatment of symptoms, by avoidance of side effects that might limit physical activity, and potentially using medications with beneficial effects on muscle function. As will all rehabilitation activities, this requires training and education of all members of the multidisciplinary team – medications not only may modify the rehabilitation process but may also affect pre-rehabilitation function and thus influence decisions as to who will benefit from rehabilitation. There has been little work on the association between medication use and habitual physical activity; similarly, most drug trials do not measure the effect of medication on physical function. Future research should therefore focus both on observational work to better understand the association between medication use, illness, and activity levels and on intervention packages to optimise medication use in people with low physical activity levels and those undergoing rehabilitation. Such work would facilitate the implementation of better informed objective physical activity monitoring studies, which are much needed in the older adult patient group.
Footnotes
Peer review:
Four peer reviewers contributed to the peer review report. Reviewers’ reports totalled 1323 words, excluding any confidential comments to the academic editor.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Clare L Clarke is a research fellow funded by the Dunhill Medical Trust (grant number: R315/1113).
Declaration of conflicting interests:
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Both authors are investigators on the ALFIE trial, funded by the Dunhill Medical Trust (ISRCTN03331094).
Author Contributions
CLC and MDW divided the work equally for this article.