
Abstract
Background:
Foetal alcohol spectrum disorders (FASDs) are one of the most common preventable forms of developmental disability and congenital abnormalities globally, particularly in countries where alcohol is considered socially acceptable. Screening for alcohol use early in pregnancy can facilitate the detection of alcohol-exposed pregnancies and identify women who require further assessment. However, only a small percentage of children with FASD are identified in the United Kingdom. This may be partly attributed to a lack of awareness of the condition by National Health Service (NHS) health professionals.
Methods:
We developed an online survey to determine health care professionals’ (midwives, health visitors, obstetricians, paediatricians, and general practitioners) perceived knowledge, attitudes, and clinical practices relating to alcohol in pregnancy and FASD.
Results:
There were a total of 250 responses to the surveys (78 midwives, 60 health visitors, 55 obstetricians, 31 paediatricians, and 26 general practitioners). About 58.1% of paediatricians had diagnosed a patient with foetal alcohol syndrome (FAS) or FASD and 36.7% worried about stigmatisation with diagnosis. Paediatricians reported the highest levels of FASD training (54.8%), with much lower levels in midwives (21.3%). This was reflected in perceived knowledge levels; overall, only 19.8% of respondents knew the estimated UK prevalence of FASD for example.
Conclusions:
We identified a need for training in alcohol screening in pregnancy and FASD to improve awareness and recognition by UK professionals. This could improve patient care from the antenatal period and throughout childhood.
Introduction
Alcohol exposure is one of the leading risk factors for population health worldwide, and as a known toxin and teratogen, it has a direct impact on maternal and child health. 1 There is a body of evidence demonstrating that prenatal alcohol exposure (PAE) can profoundly affect the foetus and result in a myriad of lifelong physical and cognitive disabilities, known internationally as foetal alcohol spectrum disorders (FASDs). 2 Foetal alcohol spectrum disorder is an umbrella term that encompasses several medical diagnoses, from the complete presentation of foetal alcohol syndrome (FAS), to a range of conditions – including partial foetal alcohol syndrome (pFAS), alcohol-related birth defects (ARBDs), alcohol-related neurodevelopmental disorders (ARNDs), and neurobehavioral disorder associated with prenatal alcohol exposure (ND-PAE). These diagnostic terms demonstrate various features of FASD and facilitate appropriate interventions in the patient pathway. For clarity, the term FASD will be used in this article. In the United Kingdom, FASD has recently become increasingly prominent within the public health agenda, as awareness of the condition slowly improves. 3 The Chief Medical Officers for the United Kingdom recommend that pregnant women, or those planning to become pregnant, avoid drinking any alcohol at all to keep risks to a minimum. 4 Screening for alcohol use early in pregnancy will facilitate the identification of those in need of support to discontinue or reduce their alcohol consumption. 5 Furthermore, screening of the mother during pregnancy, and later of the neonate, may enable infants exposed to alcohol to be identified and diagnosed. 6 In the United Kingdom, women of child-bearing age are some of the highest consumers of alcohol. 7 Popova et al 8 recently estimated that 41.3% of women in the United Kingdom consume alcohol during pregnancy, corroborating findings by the UK Infant Feeding Survey, where two in five mothers admitted drinking alcohol during pregnancy. 9 This compares to a global estimated average of 10%, but Western societies which traditionally have a stronger alcohol culture were understandably found to have higher prevalence rates including the United States, estimated at 20% to 30%. 8 The UK National Institute for Heath and Care Excellence (NICE) 10 specifies the importance of screening as part of antenatal care, recommending that women should be given information about all issues including alcohol that may affect their health or the health of their baby. To optimise the health and well-being of women and their children, the World Health Organization (WHO) state that screening is a priority to prevent, reduce, and stop the use of alcohol during pregnancy and the postpartum period. 1
After the child is born, the early diagnosis of FASD facilitates opportunities for early intervention and management for the affected child and reduces rates of secondary disabilities, such as mental health problems and exclusion from school. 11 It also helps reduce the risk of future PAE pregnancies.
As the first point of contact, physicians and other health care professionals are in a position to fulfil a crucial role in the prevention and identification of FASD. Appropriate screening for prenatal alcohol use should be prioritised in clinical practice, as eliminating or decreasing alcohol consumption at any point in pregnancy will reduce the risk of harm to the foetus. 12 The effectiveness of brief interventions are well documented, and even the process of screening has been shown to raise awareness and may reduce alcohol consumption in pregnancy. 2 It is, therefore, important to consider the knowledge and attitudes of health care professionals regarding alcohol because a lack of understanding of the issues will limit opportunities for FASD prevention, diagnosis, and early intervention. 13 Several international studies involving doctors and midwives have demonstrated confusion around the appropriate advice to give to pregnant women on the use of alcohol in pregnancy and the effects of alcohol on the foetus. Payne et al 14 surveyed 166 midwives across Western Australia and reported that 93.2% said that they ask about alcohol consumption in accordance with the national guidelines which advocate that not drinking is the safest option in pregnancy. In addition, 64.2% stated that they informed women of the effects of PAE, 47.5% did not always use the recommended Alcohol Use Disorders Identification Test (AUDIT; a simple screening tool developed by WHO to pick up the early signs of hazardous and harmful drinking and identify mild dependence), and 70.4% admitted to not providing brief interventions. Diekman et al 15 surveyed 600 US obstetrician-gynaecologists and found that although 97% reported asking patients about alcohol consumption, only 20% would advise abstinence as the safest option in pregnancy, 13% were unsure about harmful levels, and 4% believed that eight or more drinks per week would not increase the risk of adverse outcomes. Some studies have identified the provision of vague advice regarding drinking alcohol in pregnancy, recommending ‘cutting down’ rather than ‘giving up’ alcohol.12,16,17 It has been suggested that conflicting official British national health and professional organisations and even international advice has confused the issue for health care professionals and women alike. 18 For example, the lack of conclusive evidence regarding the safety of low levels of PAE has contributed to the varying guidelines and advice on alcohol consumption during pregnancy.
Thousands of families are currently seeking an FASD diagnosis for their children and have voiced their concerns over the lack of services available. 19 The FASD Network United Kingdom has requested this research to raise awareness with health care professionals to help address this important issue. 20
The level of FASD knowledge among professionals is a documented factor that influences the rates of diagnosis.21,22 The literature reports that paediatricians under-report FASD and even misdiagnose the condition as other medical conditions such as attention deficit hyperactivity disorder, due to stigma as well as diagnostic uncertainty. 17
Evidence suggests that biomarkers may have clinical value in detecting alcohol consumption in pregnancy, to highlight women in need of support and later to facilitate diagnosis for children affected with FASD. 23 Consequently, we were interested in finding the views of health care professionals around obtaining blood or meconium samples to supplement self-report, given the complex ethical nature of the issue.
The aim of this study was to explore the current perceived knowledge, practices, and attitudes of the key health professionals in the United Kingdom regarding alcohol consumption in pregnancy and FASD in childhood. For the purpose of this study, we adopted the Oxford Dictionary definition of Knowledge ‘Facts, information and skills acquired through experience or education; the theoretical or practical understanding of a subject’.
It was intended that these findings would help address an apparent gap in knowledge when the UK prevalence rate for alcohol consumption in pregnancy is the fourth highest in the world, and yet most children with FASD-related disabilities remain undiagnosed and therefore, unsupported. We intend to use the results from this study to highlight the training needs of each professional group to provide evidence based recommendations to improve clinical practice.
Ethics
The study received a favourable ethical opinion from the Tyne & Wear South National Research Ethics Committee (Ref: 15/NE/0216). The survey data presented here were provided on a voluntary basis and were collected anonymously using an online survey.
Methods
This was a cross-sectional online survey conducted between October 2015 and July 2016.
Key professional groups were sent a web-link to the survey via email. We used a pragmatic cascade method of distribution to maximise the number of potential respondents, making the exact figures approached unknown. An introductory summary contained information about the study aims and how the data would be used. The contact details of the lead midwife (H.H.) were also given in case respondents required more information before completing the form. Given the nature of data collection, written consent was not obtained from those who completed the survey. Names and addresses, or any other personal identifiable data, were not collected.
Participants
We targeted key health professionals involved in screening for alcohol and FASD during antenatal, postnatal, and paediatric care. Surveys were sent to midwives, obstetricians, general practitioners (GPs), health visitors, and paediatricians. In the United Kingdom, the role of the midwife is to provide care and support to women during pregnancy, throughout labour, and the early postnatal period. The midwife enables women to make informed choices about their care and is usually the first and main contact. Whereas, health visitors are nurses or midwives who have completed extra training to work with families to give pre-school-age children the best possible start in life by promoting healthy lifestyles and preventing illness. Contact with the family usually begins antenatally with an introductory visit at around 32 week’s gestation. An email cascade approach was used for distribution using colleagues and contacts at local, regional, and national levels. These included the local National Health Service (NHS) Trust distribution network and research and professional organisations such as the National Institute for Health Research Local Clinical Research Network and the Institute for Health Visiting. We asked recipients to forward the survey links to other colleagues to maximise the number of respondents.
Survey questionnaire
The online survey was piloted by representatives from each professional group before general circulation and took under 10 minutes to complete. After feedback, some questions were adapted to aid clarification and ensure that the profession-specific part of the surveys were appropriate. No data from the pilot phase were included in the final results because we did not want to compromise the accuracy and consistency of the results. Health care professionals were asked general questions around alcohol in pregnancy and FASD in the first part of the questionnaire, and the later questions were adapted to the specific role of each profession. For example, obstetricians and midwives were asked about alcohol during pregnancy and referring mothers while paediatricians and health visitors focussed more on the presentation of the children with FASD and retrospective PAE issues. We wanted to gain a greater insight into perceived knowledge and confidence levels in all professions and learn about a general range of issues around alcohol and FASD screening, referral practices, and finally, diagnostic experience. The intention was then to identify the gaps in perceived knowledge to inform future training provision. Feedback regarding professional practice in the United Kingdom is of particular interest, as the current documented lack of service provision poses many challenges to NHS staff. 19 We were guided by the questions asked by the existing international body of knowledge so that we could augment existing data and compare this to our UK sample of respondents. The questions were multiple-choice type with additional free text to complete where appropriate. The questions can be categorised into three broad areas of clinical practice, knowledge, and attitudes, which we acknowledge can overlap. The questions are listed in Table 1.
Survey questions.

Abbreviations: AUDIT, Alcohol Use Disorders Identification Test;
TACE,
Data analysis
Data analysis was supported by the software package SPSS (version 23, IBM Corp, Armonk, NY, USA). Data were summarised using standard summary statistics (eg mean, median, and frequency) depending on the type of data collected. We employed descriptive statistics to gain in-depth information from our respondents. Only valid responses are included. In this study, invalid answers referred to unanswered questions, or the field was left blank. For three questions, an answer was given which did not appear to answer the question. In these cases, the answer was deemed invalid. Three researchers reviewed the data and came to a consensus regarding valid answers. All responses were also verified by the co-authors to reduce bias.
Results
There were a total of 250 responses to the surveys: 78 midwives, 60 health visitors, 55 obstetricians, 31 paediatricians, and 26 GPs responded during the data collection period (10 months).
Clinical practice-related results
Alcohol screening practices in pregnancy
Rates of reported screening for alcohol use were generally high (midwives
68/75 [90.7%], health visitors 51/55 [92.7%], obstetricians 41/55 [74.5%],
although rates were lower in GPs 14/26 [53.8%]). However, there was little
consistency in the choice of alcohol screening tools. The most common
approach used by 113 respondents was simply detailed questioning with no
specific tool. Five clinicians used AUDIT. Alcohol Use Disorders
Identification Test – C, a shortened version of the AUDIT tool, was used by
32 professionals. A total of 18 staff utilised a local NHS Trust-specific
assessment. Four respondents used TACE (a measurement tool of four
questions:
Referral for alcohol use in pregnancy
Reported levels of drinking at which midwives would refer varied considerably: 32/75 (43.2%) specified they would refer for any reported alcohol consumption, 10 (13.5%) stated they would refer if drinking more than 14 units of alcohol per week and 8 (10.8%) if more than 21 units per week. A further 11 (14.9%) indicated they would only refer if the patient was visibly drunk at an appointment. Responses from health visitors were similar: 26/53 (49.1%) indicated they would refer if any drinking was reported, 6 (11.3%) if greater than 14 units per week and 4 (7.5%) is greater than 21 units per week, 3 (5.7%) said they would only refer if the patient was visibly drunk when seen.
Of 51 midwives who answered that they had referred someone for alcohol use in pregnancy, 36 (70.6%) had referred to an alcohol specialist nurse and 42 (82.4%) to an obstetrician, 16 (31.4%) to addiction services and 18 (35.3%) to a social worker or child protection officer. Of 32 health visitors who had referred someone for alcohol use in pregnancy, 28 (87.5%) had referred to an alcohol specialist nurse, 4 (12.5%) to an obstetrician, 11 (34.4%) to addiction services, and 12 (37.5%) to a social worker.
Only 5/25 GPs responded that they would refer for any alcohol consumption in pregnancy, 8 if consumption was greater than 14 units per week, and 5 if greater than 21 units per week: 8 specified they would refer if the patient was visibly drunk when seen.
Referral for FASD
The numbers of known children with FASD were very low, with five or fewer was the most common response even among paediatricians. Of the 31 paediatricians in the study, 18 (58.1%) had diagnosed a patient with FASD. However, 11/30 (36.7%) said they worried about stigmatisation with diagnosis and, of these, 2 said they had been convinced of a diagnosis but did not refer to more specialist services.
51/55 (92.7%) health visitors said they would refer an infant with FASD to a paediatrician or neurodevelopmental paediatrician, and 36 (65.5%) would refer to the GP and 12 (21.8%) to a social worker. All 24 GPs respondents said they would refer to a paediatrician or neurodevelopmental paediatrician, and 3 said they would refer to a social worker.
Knowledge-related results
Training in screening for alcohol use in pregnancy and identifying FASD in infants
Rates of previous training in FAS and FASD (Figure 1) were generally low, with midwives and GPs having the lowest rates of previous training and health visitors the highest rates. This was corroborated with a high level of requests for further training across the specialities, ranging from 98% of health visitors to two-thirds of GPs. Online training packages were requested by some respondents because they can be easily accessed at a time and place to suit.

Previous training and need for further training.
Perceived knowledge of FASD
The lack of training was reflected in low levels of knowledge about the prevalence of FAS and FASD in the general population. Overall, only 22.1% of respondents knew the estimated prevalence of FAS and only 19.8% the estimated prevalence of FASD (Figure 2).
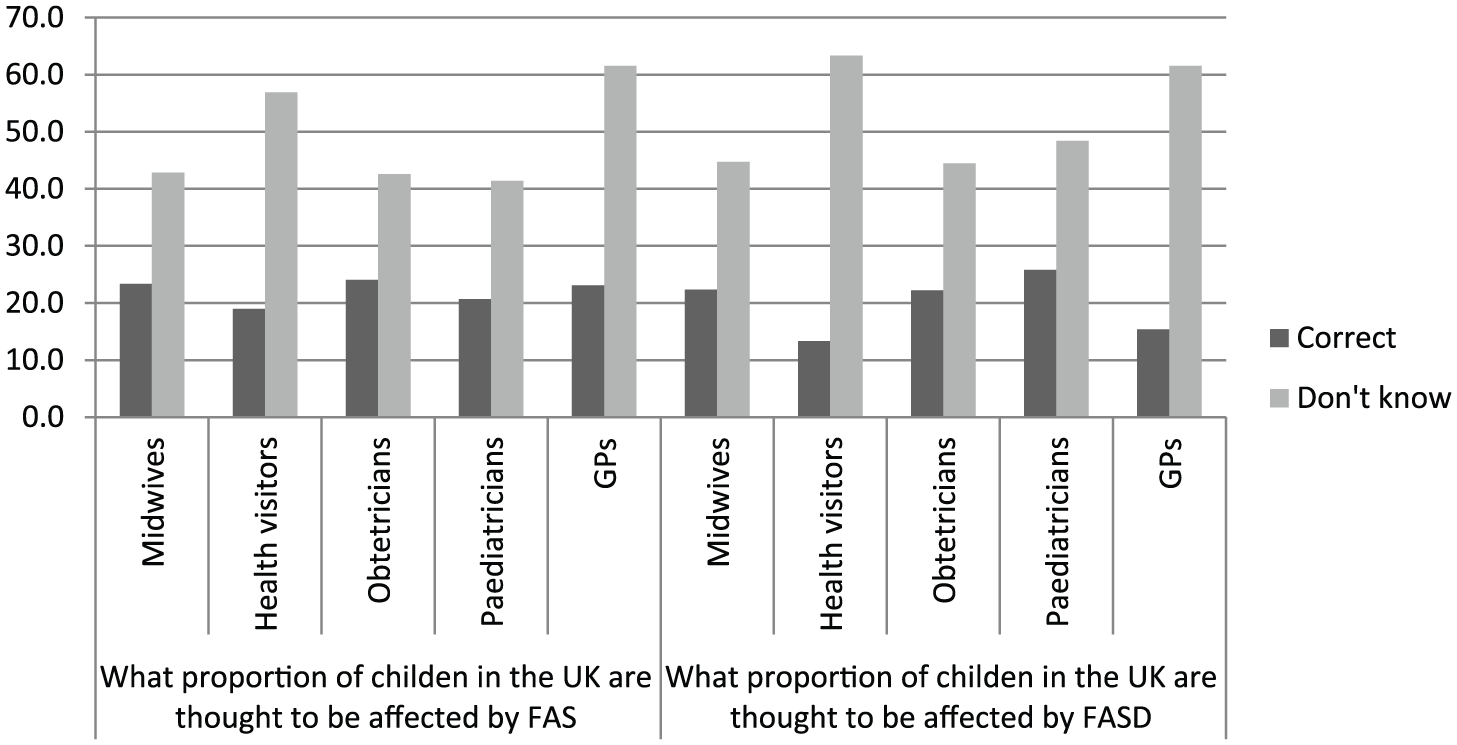
Knowledge of the prevalence of FAS and FASD.
Discussing FASD with parents
Health visitors, paediatricians, and GPs were asked how comfortable they would feel discussing FASD with a parent; 38/60 (63.3%) of health visitors, 24/30 (80.0%) paediatricians, and 23/25 (92.0%) GPs said they would feel comfortable.
Signs, symptoms, and diagnosis
A total of 17 from 74 (23.0%) midwives said they would feel confident (1 very confident and 16 fairly confident) in identifying the signs and symptoms of FASD, whereas 11/55 (20.0%) health visitors and only 1 (3.8%) GP said they would feel confident (all fairly confident). Confidence was higher in paediatricians (64.5%, 15 fairly confident and 5 very confident) and obstetricians (34.5%, 18 fairly confident and 1 very confident).
A total of 18 (58.1%) paediatricians had previously diagnosed FASD, although only 3 (9.7%) claimed to be very confident and 14 (45.2%) fairly confident about diagnosing FASD. In contrast, only one (3.8%) GP disclosed they had ever diagnosed FASD before, two (7.7%) said they would be fairly confident about diagnosing; none stated they would be very confident.
Attitude-related results
Attitudes to blood and meconium screening
As blood and meconium screening has the potential to detect alcohol consumption in pregnancy and supplement self-report, professionals opinions were sought on the feasibility of both in practice. General practitioners (64.0% and 70.8%, respectively) and health visitors (74.6% and 63.8%, respectively) were much stronger advocates than midwives (56.4% and 41.6%, respectively), obstetricians (45.5% and 43.6%, respectively), or paediatricians (40.0% and 35.7%, respectively).
Discussion
The results of this study gives us a greater understanding of the perceived knowledge, attitudes, and clinical practices of the key health care professionals delivering care throughout the patient journey from the antenatal period and throughout childhood. This included the identification and referral of women who drink alcohol in pregnancy and the identification and diagnosis of children with FASD. Furthermore, the results of our survey support findings from other settings, suggesting that these issues are not unique to the UK health system. 14 Indeed, many of the underlying reasons for this lack of consistency (eg lack of confidence in discussing a sensitive issue, rights of the individual, and lack of a clear ‘gold standard’ to screen for alcohol use) are common globally. 17
Clinical practices
Awareness and practices around alcohol screening were generally very encouraging. Most professions indicated that they proactively ask about alcohol consumption, and very few from each professional group had never referred a mother for alcohol or a child with FASD. A diverse range of alcohol screening tools were used, and the levels of alcohol consumption which triggered a referral varied considerably. This trend was observed across all professional groups. Further research into developing a standardised alcohol referral protocol specifically for pregnant women may support health professionals to provide a more consistent service.
An important indicator of the success, or otherwise, of current clinical practice is the reported experiences of the women themselves. The Infant Feeding Survey 2010 9 asked women about the information they received in pregnancy regarding alcohol. Of the women who drank before pregnancy, 71% received information about drinking during pregnancy, and 62% said they had been given general information about the effects of drinking alcohol on the baby. Only 36% stated they had been given information on how to cut down or limit the amount they drank during pregnancy, while just 29% said they had been given information on stopping drinking alcohol completely. When analysing the figures for those who received information about drinking, the most common source was a midwife (81%); 14% stated a health visitor, and 13% cited a doctor. In an Australian study, Crawford-Williams et al, 24 highlighted the barriers identified by health professionals in discussing alcohol with women. They include the concepts that many professionals have a perception that most women do not drink in pregnancy; that women know not to drink; that alcohol is not a priority in a time-limited antenatal visit; and that discussing alcohol might cause anxiety, frighten, or anger the woman. 24 These perceptions can be classified into determinants such as self-efficacy, risk perception, and personal identity. The identification of specific barriers by the health professional increases self-awareness and is an important part of understanding what needs to be changed. Therefore, self-reflection and awareness of differing and potentially conflicting beliefs should be included in future training.
Referral pathways for patients with FASD varied widely, as there are no current NHS-coordinated FASD services established in the United Kingdom to date. 2 The lack of diagnostic clinics, interventions, and care pathways were reported as barriers to referrals by GPs, paediatricians, and health visitors in particular. Until very recently, only one official diagnostic clinic in the United Kingdom was available and most FASD management resources are derived from Canadian or Australian practices. 25 A lack of patient access to diagnostic services is well documented and will inevitably inhibit best practices of early intervention.17,26,27 To maintain the momentum of the informed and proactive health professionals, there is a clear need for the United Kingdom to launch standardised, high-quality FASD services.
Knowledge
FASD training was a substantial need identified across all the professional groups surveyed. In particular, screening for FASD, alcohol use, and the onward referral processes were acknowledged as learning requirements. These findings corroborate empirical evidence and previous research which concluded that if FASD-related disorders (including secondary co-morbidities) are to be effectively prevented, identified, and treated, improvements to referral systems, professional education, and screening are essential for pregnant women and children with PAE.14,21 General practitioner responses especially reflected a desire for additional training. The relatively low levels of current FASD training in the United Kingdom are reflected in the low level of knowledge pertaining to FAS and FASD prevalence. In addition, the signs, symptoms, and diagnosis confidence levels were similarly low, with the exception of paediatricians. This identified knowledge gap may compromise the provision of care for mothers and children throughout the patient journey. Interestingly, health visitors, paediatricians, and GPs demonstrated relatively high levels of confidence in discussing FASD with patients. This is an interesting finding for a group of professionals who otherwise report a lack of training in FASD and a limited knowledge base. This may be explained by the interpretation of the question in terms of professional competency rather than from an FASD-specific perspective.
Identified gaps in FASD knowledge and awareness would support a link to the considerable under-diagnosis in the United Kingdom.21,22 Popova et al 28 estimated an FASD prevalence rate of 5% based on an FAS prevalence rate in excess of 50 per 10 000 of the general population. The latest figures from a large cohort prevalence study found that up to 17% of children screened positive for FASD but had not received a formal diagnosis. 29
In the United States, Gahagan et al 27 surveyed 879 paediatricians and found that 62% could identify children with FASD, 50% would diagnose a child who presented with FASD but only 34% would manage and coordinate treatment. Similarly, Nevin et al 26 surveyed 75 family physicians in Toronto and found that 8% had diagnosed a child with FAS and 17.9% had had suspicions but had not diagnosed. Confidence levels in FAS diagnosis were found to be low with 49% feeling that they had little confidence. Furthermore, only 60.8% reported advising pregnant women on alcohol consumption.
A little over half of the paediatricians had actually diagnosed FASD and over a third expressed concerns around stigmatisation of diagnosis. This suggests that the issue of stigma needs to be explored further in training packages to facilitate the diagnosis and management of children and adults with FASD. Stigma around alcohol use in pregnancy is an international issue. In Australia, Elliott et al 30 surveyed 132 paediatricians; 76.5% reported suspecting but not diagnosing FAS, 12.1% had been convinced but not diagnosed. The authors also report that of the same paediatricians, 79.6% agreed that early diagnosis may be beneficial, but 69.6% believed that diagnosis may be stigmatising, and furthermore, 36.4% presumed that parents might resist referral for assessment and intervention. Mukherjee et al 13 also attributed the reluctance to diagnose FASD to professional lack of knowledge and stigma. Stigma is a serious concern for health professions. Corrigan et al 31 confirmed that mothers of children with FASD are significantly stigmatised for their past behaviour and often experience public discrimination. To address this, Corrigan et al 31 recommend contact-based strategies in preference to educational strategies when implementing stigma reduction interventions.
Attitudes
Interestingly, professionals did not necessarily agree to routine blood or meconium screening even though they may facilitate the detection of foetal alcohol exposure. This may arise from an ethical and legal perspective as patient consent was not specified in the question. General practitioners and health visitors were the strongest supporters of screening initiatives. One possible explanation may be that children’s advocacy is a key role of the health visitor, but this is also true of the paediatricians who were more circumspect. To contextualise this matter, the NHS currently recommends offering routine antenatal screening of hepatitis B, HIV, and syphilis in every pregnancy. 10 These tests arguably share similar issues of stigma and sensitivity as alcohol in pregnancy, but through training and a changing culture of practice, all have now become an accepted screening routine by women and health care professionals alike. Similarly, biomarker screening may benefit both the mother and child, and could be undertaken in a supportive manner which could direct valuable resources to those most in need.
Recommendations for practice
This study has identified a noteworthy gap in knowledge around risks of PAE and the management of children with FASD across the professions (Figure 3). This deficit will undoubtedly influence clinical practice and may partly explain the United Kingdom’s estimated high alcohol prevalence rates in pregnancy. It has also recognised clear FASD-related training needs which corroborate the conclusions of Mukherjee et al. 13 While, acknowledging that some literature may not necessarily correlate increasing knowledge with behaviour change, we feel that education is the key facilitator available in this instance. 32 Training will increase knowledge and understanding, thus providing a rationale and catalyst for health care professionals to change attitudes to prevention, diagnosis, and early intervention. To support these initiatives and behaviour changes, the United Kingdom urgently requires clear, consistent, and mandated FASD referral pathways, guidelines, early interventions, and support services for children and their families. This strategy should also include education around the risks of harm from alcohol in pregnancy. Screening for alcohol should be routine in all primary-care settings, with an emphasis on preconception health advice and contraceptive counselling. Referrals to established alcohol or substance misuse services for women identified to have an alcohol use disorder should also become the norm so that women receive the specialist support required. These initiatives could help to prevent further cases of FASD, and would minimise co-morbidities and maximise the potential of individuals with FASD. A high-profile public health promotion to alert both health professionals and the general public to the risks of foetal alcohol exposure is overdue. Future research should seek to better understand FASD prevalence and characteristics of at-risk groups so that effective services and interventions can be developed. A cost-benefit analysis of the impact of awareness raising, training, screening, and referral on downstream costs to health and social care budgets should also be conducted to support the engagement of stakeholders at Government level. A Canadian study has referred to children with FASD as $1 million babies, but the prevention and management costs are likely to be a fraction of this. 33
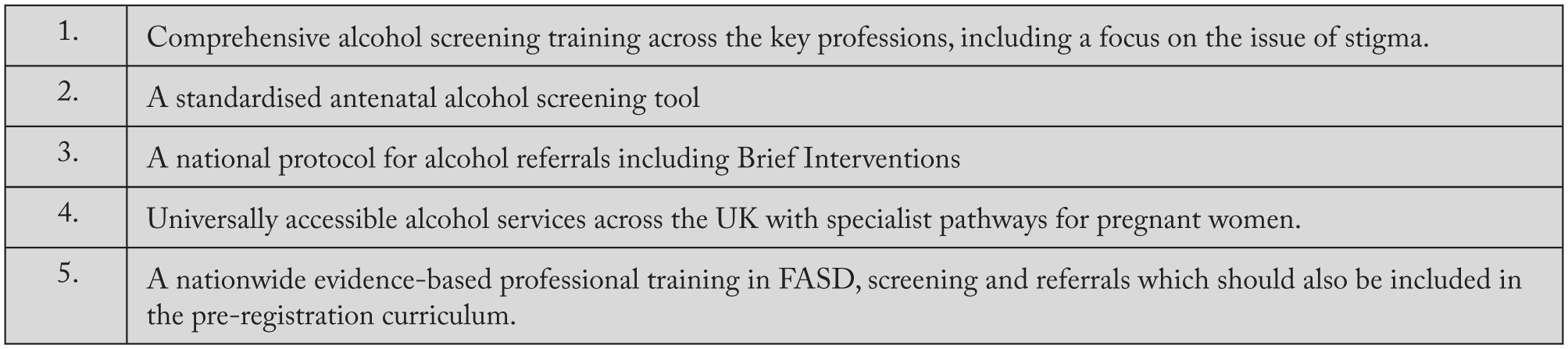
Recommendations for practice.
Strengths and limitations
We had originally planned to send our surveys to each relevant professional body for distribution across the United Kingdom. However, this approach was denied by all but the Institute of Health Visitors. We, therefore, asked local professional networks such as the North East and North Cumbria Clinical Research Network to circulate the questionnaires among all eligible health professionals locally and nationally. We requested all recipients to forward our survey link to other appropriate colleagues. This pragmatic approach increased the potential number of health professionals who received a questionnaire, but unfortunately left no clear audit trail. Consequently, we do not know the total number of health professionals who were invited to participate in the survey to calculate the response rate. Ideally in future studies, we would have profession-specific questionnaires distributed from the corresponding professional governing bodies for maximum distribution.
Some health visitors responded to the paediatrician’s questionnaire, but we were able to identify them from the first question which asked about their speciality area. The data were then reassigned to the health visitor statistics. We are unable to comment on the generalisibility of our responders. Our results may be influenced by the inherent response bias of any survey questionnaire. The professionals who have an interest in alcohol consumption in pregnancy and FASD may have been more likely to participate. This could have led to an overestimation of knowledge, attitudes, and practices in this sample. Social desirability bias may also confound self-reported opinions and practices. This may influence responses to sensitive questions around as assessment and management, but the anonymity of this research should mitigate this bias. This exploratory study gives insight into the perceived knowledge, attitudes, and practices of five strategic NHS professions in relation to alcohol in pregnancy and FASD throughout childhood.
The generic limitations of questionnaires could also be applied to this study and include factors such as the truthfulness of responses, individual’s agendas, a lack of conscientious response and differences in understanding and interpretation. We also recognise that our findings are based on self-report and not a formal assessment of knowledge but still provide a useful insight.
Finally, due to the scope of this study, we were unable to examine individual’s detailed personal beliefs and perceptions, as many aspects of clinical practice that we asked about such as screening tools and referrals are guided by local protocols and resources. However, this topic would be worthy of future investigation and could include more qualitative methodologies such as interviews and focus groups.
Conclusions
This study highlights a need for training and education regarding the risks of alcohol in pregnancy and FASD in children for health professionals in the United Kingdom. The health care infrastructure around FASD across the life course in the United Kingdom lags behind many Western countries such as USA, Canada, and Australia. However, we can learn from their experience and share the best practices already established on an international scale. If we are to prevent or minimise the risk of harm from PAE and make a significant difference to the outcomes of individuals with FASD, we need to work collaboratively to expedite the establishment of world class FASD services throughout the United Kingdom.
Footnotes
Acknowledgements
The authors wish to acknowledge the help of their colleagues at the Northumbria Healthcare NHS Foundation Trust. The authors also like to express their sincere thanks to everyone who completed the survey and made this research possible.
Funding:
This study was funded and sponsored by the Northumbria Healthcare NHS Foundation Trust.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
H.H., S.M., E.-M.S. and J.R. conceived and designed the study. H.H. and W.K.G. were involved in data acquisition and H.H. and W.K.G. contributed to data analysis. H.H. wrote the paper and all authors commented on the paper and gave final approval for submission.
Ethics
The study received a favourable ethical opinion from the Tyne & Wear South National Research Ethics Committee (Ref: 15/NE/0216). The survey data presented here were provided on a voluntary basis and were collected anonymously using an online survey.
Funder’s Role
The sponsor of this study had no role in the study design, in collecting the data, in data analysis or interpretation, in writing this manuscript, or in the decision to submit to this journal for publication.