
Abstract
Introduction:
Our study aimed to assess the impact of managed complications of tension-free vaginal tape (TVT) on the patients’ assessment of the results as measured by Patient Global Impression of Improvement (PGI-I).
Materials and methods:
This was a retrospective study, supplemented with a telephone interview, comparing patients who had complications of TVT procedures with those where no complications recorded. The primary outcome was the PGI-I score in the 2 groups.
Results:
A total of 118 invitations were sent. In all, 60 patients returned the signed consent and completed the telephone interview with one of the authors (response rate = 50.8%). Complications were recorded in 21 patients (group 1) and no complications in 39 patients (group 2). There was no statistically significant difference between PGI-I in both groups.
Conclusions:
Managed complications of TVT do not seem to affect patients’ assessment of outcome as measured by PGI-I score.
Introduction
Tension-free vaginal tape (TVT) has become the procedure of choice for treating urinary stress incontinence in women. 1 Many studies have reported the short-term and long-term outcomes of TVT including patients’ assessment of results. Fewer studies have reported the complications of TVT. Recorded complications include bladder perforation (4.9%-24%) excessive bleeding (0.9%-2.5%), pelvic haematoma (1.7%-1.9%), voiding dysfunction (4.9%-29%), with 8% to 10% required surgical intervention, overactive bladder (OAB) symptoms requiring anticholinergics (12%-30%), recurrent urinary tract infection (10%), and mesh erosion (0.4%-0.9%).1 -5 However, there is lack of data regarding the impact of these complications on the patients’ assessment of the outcome of sling. One study reported no impact of bladder injury on patient satisfaction. 3
Our study aimed to assess the impact of managed complications of TVT on the patients’ assessment of the results as measured by Patient Global Impression of Improvement (PGI-I). 6
Materials and Methods
This was a retrospective study, supplemented with a telephone interview, including patients who underwent TVT sling by the senior author in a private hospital between 2009 and 2014. There were no exclusion criteria. Patients were identified from practice management computer records. All patients were invited to participate in the study and asked to sign and return consent. The study was approved by The University of Queensland Medical Research Ethics Committee.
Preoperative assessment included symptom-specific questionnaires (International Consultation on Incontinence Questionnaire Urinary Incontinence – Short Form [ICIQ-UI-SF]), urine microbiology, and urodynamic testing.
All participants were interviewed over the telephone and asked to score their impression of improvement using PGI-I score.
Patient Global Impression of Improvement is a score given by the patients expressing their perception of improvement or worsening of their condition. Patients were asked to select the category which fits most with their perception of improvement (Figure 2). Patient Global Impression of Improvement was selected as a patient-reported outcome measure (PROM) as it has an established construct validity in patients with urinary incontinence. 6
Surgical Procedure
All procedures were performed by the senior author under general anaesthetic through 1.5-cm vaginal incision starting at 0.5 cm from the urethral meatus and two 1-cm skin incisions just above pubic bone. Bladder was deviated away from the trocar pathway using a rigid inserter into Foley catheter. The TVT was inserted and cystoscopy check was performed using 70° cystoscope to exclude bladder perforation. 7 A pair of straight Mayo scissors was placed between the urethra and the sling while the tape is pulled to its final position. Where concurrent procedures were undertaken, TVT sling was inserted first, but the position was adjusted at the conclusion of the concurrent procedures. Antibiotic prophylaxis was used for all patients at the time of induction of anaesthesia. Indwelling urinary catheter was inserted at the end of the procedure and removed next morning. Trial of void was considered successful if the residual urine was less than the 1/3 of total bladder capacity (defined as voided urine volume + residual urine volume). 8
Data Collection
Data were collected retrospectively from records and supplemented by phone calls. Preoperative and postoperative data at 6 weeks, 6, and 12 months were collected. The participants’ charts were reviewed by one of the authors. Data collection included demographic data, concurrent operations performed, preoperative and postoperative scores of ICIQ-UI-SF, intraoperative and postoperative complications, and recorded management of complications as well as the PGI-I score collected by phone interview with the patient. Figure 1 illustrates the flowchart of the study.
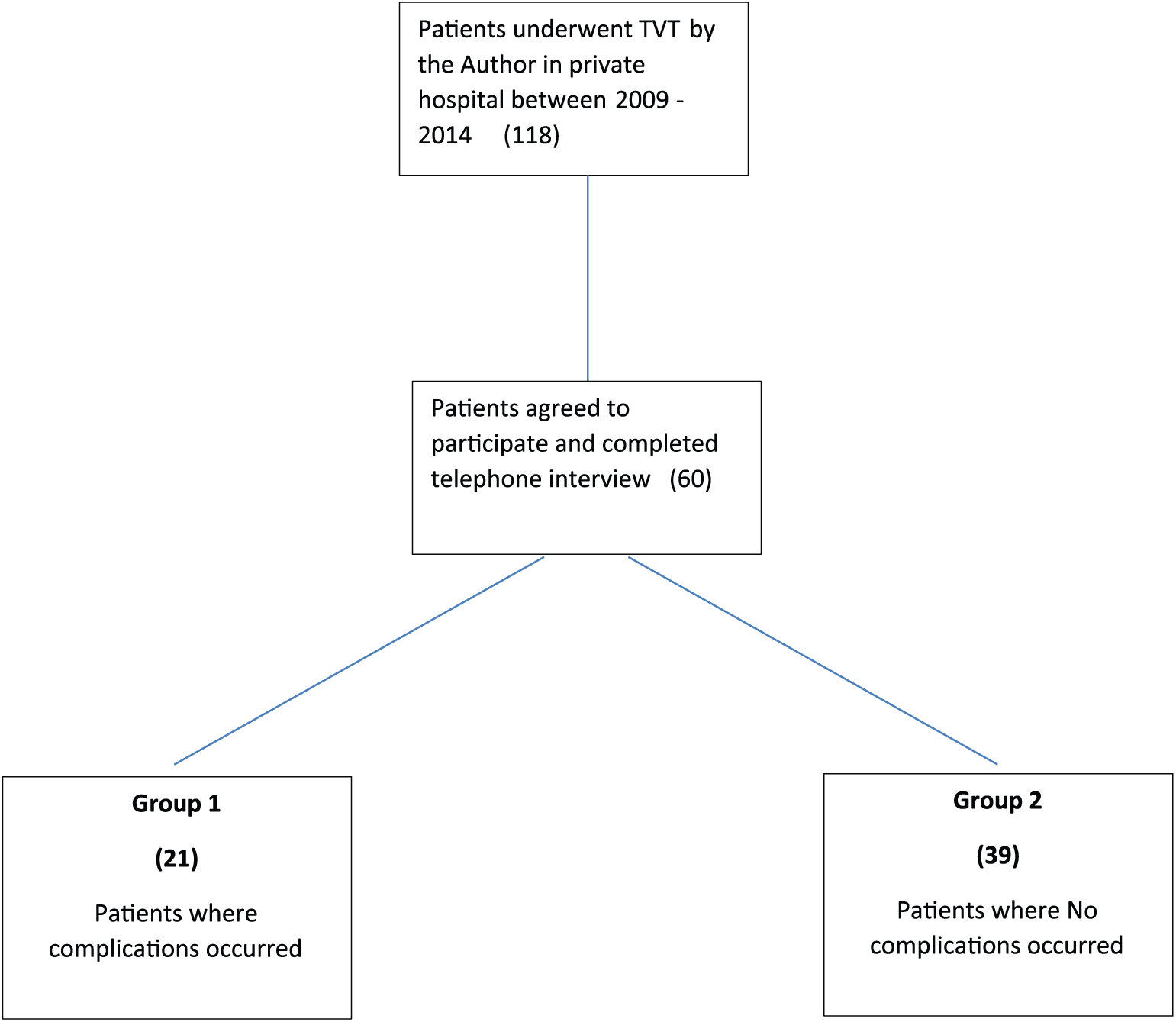
Flowchart of the study.
Statistics
Group 1 included patients where complications were recorded, and group 2 included all other patients. The primary outcome was the PGI-I score in the 2 groups. Secondary outcomes included prevalence of complications in all patients who underwent TVT, postoperative ICIQ-UI-SF score for the 2 groups, and the complications associated with different PGI-I scores. The 2 groups were compared using t test for continuous variables (an alternative of analysis of variance test was tried which gave similar results) and Fisher exact test for nominal variables as the numbers are small and exact test is more accurate. Kruskal-Wallis test was used for nonparametric variables including PGI-I score and ICIQ-UI-SF score as the values in PGI-I and ICIQ-UI-SF are ranking values.
Results
A total of 118 invitations were sent. In all, 60 patients returned the signed consent and completed the telephone interview with one of the authors (response rate = 50.8%).
Table 1 summarises patients’ characteristics, preoperative urinary symptoms, and ICIQ-UI-SF for the 2 groups. There was no statistically significant difference between the 2 groups in age, parity, previous surgical procedures including pelvic floor surgery, interval since surgery at the time of telephone interview or the preoperative ICIQ-UI-SF score. Both groups were comparable also in the number of concomitant procedures performed. Urinary symptoms were not different in the 2 groups.
Patients’ characteristics and preoperative findings for the 2 groups.

Abbreviations: ICIQ-UI-SF, International Consultation on Incontinence Questionnaire Urinary Incontinence – Short Form; IQR, interquartile range.
Patients may have more than one of these concomitant procedures.
Table 2 summarises the postoperative outcome expressed as PGI-I and postoperative ICIQ-UI-SF for the 2 groups, whereas Figure 2 represents chart of PGI-I for the 2 groups. Median PGI-I was slightly worse in the complication group, but the difference was not statistically significant, also there was no statistically significant difference between the 2 groups in terms of number of patients reporting significant improvement, little or no improvement, or being worse off after surgery. On the contrary, postoperative ICIQ-UI-SF score was statistically higher in group 1 (complications group).
Postoperative outcomes for the 2 groups.

Abbreviations: ICIQ-UI-SF, International Consultation on Incontinence Questionnaire Urinary Incontinence – Short Form; IQR, interquartile range; PGI-I, Patient Global Impression of Improvement. Bold value: statistically significant.

Chart of Patient Global Impression of Improvement (PGI-I) for 2 groups.
Table 3 summarises the incidence of different complications. In total, 10 patients had OAB, but only 5 had de novo symptoms. About 7 patients had voiding difficulty, 5 managed conservatively, and 2 cases had the TVT sling mobilised under anaesthesia, but no cases needed the TVT to be cut or excised. Figure 3 represents the complications behind each of PGI-I scores. Although the small numbers limit the ability to interpret these data with confidence, Figure 3 shows that high PGI-I scores signifying patients dissatisfaction were all associated with OAB symptoms either de novo or persistent postoperative OAB.
Complications of tension-free vaginal tape.

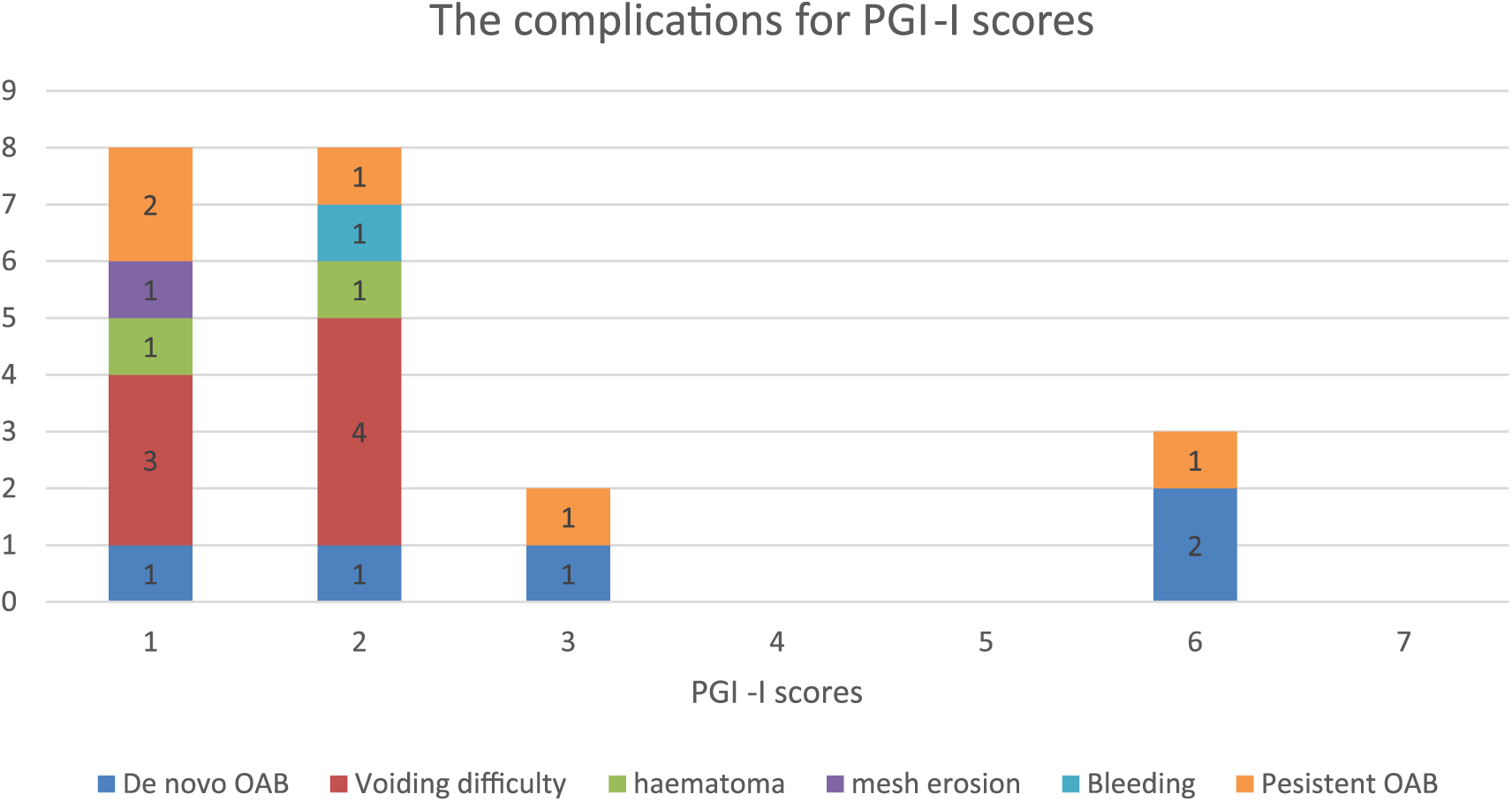
The complications for different PGI-I scores. PGI-I indicates Patient Global Impression of Improvement.
Discussion
Our study compares the patients’ reported outcome after TVT with or without complications. This study shows that considering patients’ assessment of outcome of TVT using PGI-I, there was no significant difference between patients who sustained complications and those who did not.
In our study, despite low incidence of de novo OAB (8.3%), it was the complication associated with highest patients’ dissatisfaction. This was also suggested by Reich et al 1 who reported that urge incontinence was the main reason for dissatisfaction in 90% of discontent patients. De novo OAB was reported by Serati et al 9 to occur in 30.1% of patients after TVT, whereas Reich reported de novo urge incontinence to occur in 14.8% of patients within 10 months increased to 32% after 102 months. Schierlitz et al 10 reported de novo urgency of 21% and de novo urge incontinence of 13% after TVT. As de novo OAB is the main reason for patients’ dissatisfaction, we suggest that its low incidence in this series could explain the lack of significant impact of complications on PGI-I.
Although complications did not change PGI-I significantly, ICIQ-UI-SF score was significantly affected by complications. This difference between PGI-I and ICIQ-UI-SF reflects the difference between patients’ assessment of outcome which is more subjective and the objective assessment of urinary symptoms using validated symptoms scoring methods. Although there is no doubt that objective outcomes are more accurate to measure and compare, in today’s health care generally and urogynecology especially, there is an increasing emphasis on using PROMs.
We did not collect specific data about stress incontinence postoperative as this was not one of the aims of the study. However, we recognise that failed surgery with persistence of stress incontinence may have affected ICIQ-UI-SF scores and contributed to the significant difference between ICIQ-UI-SF scores for the 2 groups.
Voiding difficulty is another common complication after TVT. We reported voiding difficulty to occur in 11.6%; this is considerably less than reports by Shippey et al 11 who reported 40% short-term voiding difficulty. However, Freeman et al 12 reported that only 5.8% required catheterisation, and Schierlitz et al 10 reported that 8.5% had short-term catheterisation. This large difference in the reported incidence of voiding difficulty after TVT reflects different definitions used in assessing voiding difficulty. We considered catheterisation for more than 24 hours as voiding difficulty. In considering who needed further catheterisation after initial catheter removed, we used the limit of residual urine volume less than 1/3 of total bladder volume as suggested by Kleeman et al. 8 All patients who failed to satisfy this criterion after 5 days (2 patients) underwent early mobilisation of the sling. Using this strategy, we had no long-term voiding difficulty, and all patients who sustained voiding difficulty had PGI-I of 1 to 2. Price et al 13 have reported significant success of early mobilisation of TVT sling in patients with voiding difficulty.
The study has limitations including the low participation rate of patients and the retrospective design. However, the use of telephone interview did offer prospective data about PGI-I which is the primary outcome of the study. We recognise that face-to-face interview would have given more insight than the telephone; however, we felt that more patients would have declined participation in the study if they were to attend in person. The study represents the first to assess impact of complications on patients’ assessment of outcome of TVT.
Conclusions
Within its limitations, the study shows that managed complications of TVT do not seem to affect patients’ assessment of outcome as measured by PGI-I score. De novo OAB symptoms are associated with the worst patients’ satisfaction.
Footnotes
Acknowledgements
The authors would like to thank Mrs Emma Buttler for helping in retrieval of patients’ clinical notes.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by The University of Queensland, Faculty of Medicine Summer Scholarship Program.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
DS conceived and designed the study and wrote the first draft of the manuscript. AJL and GC contributed to data collection. DS and GC contributed to data analysis. All three authors contributed to writing of the manuscript.
Disclosures and Ethics
As a requirement of publication, authors confirm compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality, and protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. The study was approved by Human Research Ethics Committee, University of Queensland. Approval number 2014001183.