
Abstract
Background:
Voiding dysfunction (VD) is a frequent reason for primary care referrals to urologists and pediatric urologists. VD symptoms include urine incontinence (UI), urinary tract infection (UTI), hyperactive bladder, and constipation. Early detection of Nocturnal enuresis is critical due to its high frequency and the consequences for families and children regarding psychological and behavioral aspects.
Objectives:
This study aims to determine the prevalence of voiding disorder in Palestine and its relationship to demographic, family, and behavioral risk factors.
Design:
A cross-sectional study.
Methods:
This study administered a 2-part validated questionnaire to the mothers of primary school-age children who had no history of urological disease between December 2022 and March 2023.
Results:
Out of 169 children; daytime incontinence was found in 39 (23.2%) of the sample, whereas nocturnal enuresis was found in 49 (28.4%). Age was significantly correlated with voiding dysfunction, in which 25 (55.6%) were under the age of 7 years (P = .025).
Conclusion:
According to our data, VD is a widespread health issue in primary school. Expanding our understanding of voiding dysfunction is important to eliminate the social stigma associated with voiding disorder and encourage parents and children to seek treatments and therapies. Furthermore, raising awareness will aid in early diagnosis, resulting in fewer long-term problems and earlier treatments. Raising awareness can be accomplished through educational programs focusing on primary care screening.
Introduction
Voiding dysfunction (VD) is a common problem in primary care in which children need to be referred to the urologist pediatricians, and urologist for treatment. 1 Nocturnal enuresis (NE) hurts the affected child and their family’s social, psychological, and emotional health. 2 In some cases, the psychological and developmental damage may be more significant and devastating to the child than the symptom of enuresis itself. 3
Dysfunctional Voiding is habitually contracting the urethral sphincter or pelvic floor during voiding. It demonstrates a staccato pattern with or without an interrupted flow on repeat uroflow when EMG activity is concomitantly recorded in a neurologically intact patient. 4 It can present a variety of symptoms like urinary incontinence (UI), urinary tract infection (UTI), overactive bladder, or constipation. 1 Urinary incontinence is defined as involuntary leakage of urine and can be continuous or intermittent. Intermittent incontinence is the leakage of urine in discrete amounts, if that occurs while awake, it is termed daytime incontinence. 4 Nocturnal enuresis is a prevalent condition among young children, characterized by an inability to control urination and involuntary urination during sleep. The child must be Five years of age or older, have at least 1 episode of nocturnal enuresis, experience daytime urinary incontinence once a month, and were having the enuresis problem for a minimum of 3 months in order to meet the criteria of the International Classification of Disease (ICD-10) for a symptom.4,5
Enuresis is differentiated according to the presence or absence of lower urinary tract symptoms which are non-monosymptomatic and monosymptomatic, respectively. It is also classified according to the most expanded period of dryness: primary (less than 6 months dryness) or secondary (more than 6 months dryness). 4 The pathophysiology behind nocturnal enuresis is complex and multifactorial with causes including genetics, environmental, and psychological stressors. In addition to delayed and immature nerve development, bladder immaturity and disturbances in antidiuretic hormone secretion and reception play roles.6 -8 Studies have shown multiple risk factors for NE including prolonged use of disposable diapers, 9 male gender, difficulty in awakening at night, 10 mental stress, poverty, 11 and family environment. 2
Differences in the prevalence of NE and DUI across countries and areas within countries. 1 The frequency of VD and NE in Anatolia was 6.1% and 6.6%, respectively, while Joinson 2 recorded 8% DUI in Denzili city, 18% in Ankara 5 and west Iran has 8% NE prevalence, 7 Egypt 18%. 6 In Palestine, no studies have been reported on the epidemiology of NE. We aimed to investigate the prevalence of NE in primary-school-aged children in Nablus, Palestine, using a validated tool to assess potential risk factors of NE. This provides baseline data for prevention and treatment.
Methodology
Study design and settings
This is a cross-sectional study involving primary school-aged children, grades 1 through 6. Convenient sampling was employed and data were collected between December 2022 and March 2023.
Study Population, inclusion, and exclusion criteria
The study population included primary school aged children in Nablus, Palestine. We invited the mother through the children’s school committee, where they completed the required information independently. After that we distribute an online questionnaire to mothers who are unable to attend school due to their hectic schedules through an online group of mothers that the administrative schools in order to establish a connection with the mothers.
Primary school children aged 5 years or older who were not diagnosed with any sort of urological problem or disease were included in the study. Children with a history of any urological disease were excluded.
Sample size and sampling techniques
The sample size was calculated using an online Rao soft sample size calculator, which showed a convenient sample of 165. A confidence level of 95% error and a 5% margin were used.
Study tool, validity, and reliability
A 2-part questionnaire was used. The first part collected demographic data, and the second part was the Dysfunctional Voiding and Incontinence Score validated score by Serel 12
Family demographics and child behaviors included: Age, gender, type of school, amount of time spent watching TV and gaming, parents’ educational levels, family income, number of family members, amount of fluid intake per day, and history of any urological disease.
The dysfunctional voiding scoring system questionnaire for children assesses daytime symptoms, night-time symptoms, voiding habits, bowel habits, and quality of life. It consists of 14 questions with yes/no or nominal. The total score ranges from 0 to 35. A score greater than or equal to 9 indicated the presence of voiding dysfunction.
Statistical analysis
Data were entered and analyzed using the Social Sciences Statistical Package (SPSS) version 26. Categorical variables were described as absolute frequency (percentage), and continuous variables were presented as medians and interquartile ranges. The chi-square was used to test the significance between categorical variables, and the Mann-Whitney test was used to test for differences in the means between categories. The significance level was established at the P-value <.05.
Results
Children’s demographics
A total of 189 parents agreed to participate, 20 were excluded due to incomplete questionnaire, and data of the 169 children who met our criteria were included, 98 (58%) were male, and 70 (41.4%) were under the age of 7 years. The median of children’s daily fluid intake in liters was 1 [1-1.5]. Almost-two thirds, 103 (60.9%), spend 1 to 2 hours on TV watching. Most spend 1 to 2 hours on mobile phones and games 114 (67.5%; Table 1).
Children’s demographics.

Responses to the DDV9 score
Diurnal enuresis (daytime wetting) was found in 39 (23.2%) of the sample, whereas nocturnal enuresis was present in 49 (28.4%). The majority of parents reported that their children did not strain or experience pain when urinating (160 (49.7%) and 162 (95.6%), respectively). Nearly two-thirds, 111 (65.7%), reported that their child “holds their pee.” When the parents were asked about the impact of symptoms on their child’s family or social life, 128 (75.7%) reported varying degrees of impact. (Table 2)
Responses to DDV9 score.

n = 40.
n = 49.
The correlation between DVSS and children’s demographics
The dysfunctional voiding was found among 45 (26.6%) participants. Age was significantly correlated with voiding dysfunction, in which 25 (55.6%) were under the age of 7 years (P = .025). All other demographic variables, including gender, student’s school type, fluid intake, time of TV watching, and games, had no significant correlations with the dysfunctional voiding. (Table 3)
The correlation between DVSS and children’s demographics.

The bold values indicate P < .05.
Statistical significance values calculated using Pearson chi-square test.
Statistical significance values calculated using Mann-Whitney U test.
The correlation between DVSS and Family demographics for voiding dysfunction
Familial risk factors, including mother’s and father’s educational level, number of family members, and family income, were not associated with the presence of voiding dysfunction. (Table 4)
The correlation between DVSS and familial risk factors for voiding dysfunction.

The bold values indicate P < .05.
Statistical significance values calculated using Pearson chi-square test.
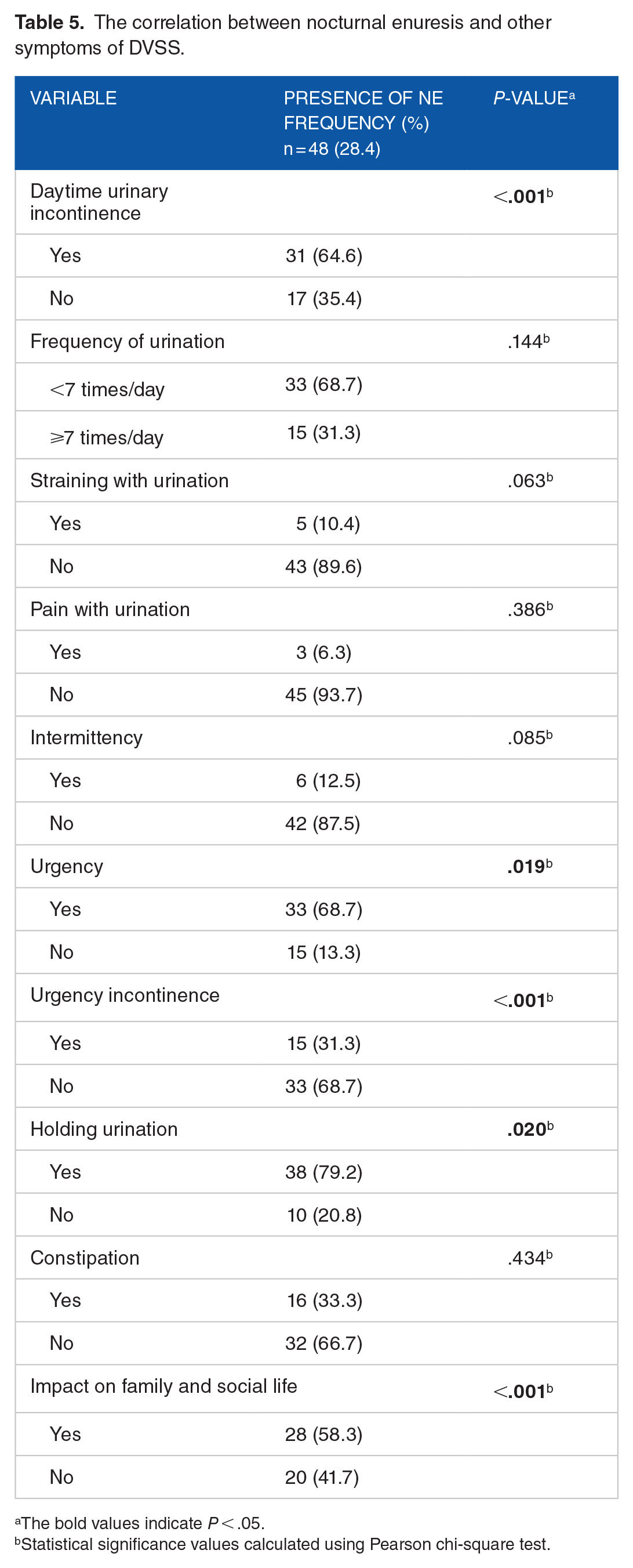
The correlation between nocturnal enuresis and other symptoms of DVSS
The nocturnal enuresis (NE) was found among 48 (28.4%) participants. Daytime urinary incontinence was significantly correlated with the presence of NE, in which 31 (64.6%) had daytime urinary incontinence (P < .001). Holding urination was significantly associated with NE 38 (79.2%; P = .020).
Furthermore, NE was significantly correlated with Urgency and urgency incontinence in which 33 (68.7%; P = .019) had urgency, On the contrary, children with urgency incontinence were less likely to have NE in which 15 (31.3%; P < .001) had urgency incontinence. Moreover, presence of NE was significantly correlated with the impact on family and social life 15 (31.3%; P <.001). Constipation, frequency of urination, pain with urination, intermittency, and straining with urination haven’t reach any statistical significance with NE (Table 5).
The correlation between nocturnal enuresis and other symptoms of DVSS.
The bold values indicate P < .05.
Statistical significance values calculated using Pearson chi-square test.
Discussion
Our study revealed an overall prevalence of daytime urinary incontinence among children of 23.2%, which is noticeably higher than the results of other studies. The prevalence rates recorded by several European countries ranged from 4.4% to 19.2%, whereas numerous Asian countries reported rates ranging from 2.1% to 6.3%.13 -17 Another study conducted in Denizli province, Turkey, revealed a prevalence of 8%. 18 In our study, 3% of the children were wetting themselves once or twice per day, and 8.9% of them were dampening their underwear. Bakker et al 13 demonstrated that the higher the frequency of daytime urinary incontinence, the more likely the degree of wetting increases.
Our study found a prevalence of 28.4% nocturnal enuresis, which is high compared to the 2 published prevalence studies performed in Turkey, which have shown that 9.8% to 12.9% of children have NE.12,19
However, these studies used wider age groups in their samples we found significantly higher rates of VD in children less than 7 years old which is consistent with the findings of a previously conducted study in Turkey which used the same validated questionnaire by Akbal et al 20 and showed a decreasing frequency of VD with age. 21
We studied the relationship between voiding dysfunction and parents’ educational levels and found no significance. Supportive results were observed in Iranian, 8 Turkish, 22 and Chinese studies. 9 Conversely, the lower the fathers’ and mothers’ level of education was significantly related to the increased prevalence of voiding dysfunction in other studies’.7,10 A possible explanation for the discrepancy with our results is secondary education access for genders of all socioeconomic statuses may vary to other countries. Interestingly, an inverse relationship was observed in another study, 23 which demonstrated increased risk of voiding dysfunction with parents of higher educational levels. They speculated that well -educated parents put increased stress on their children.
When asked how often their child used the toilet to void daily, 40 out of 169 participants (23.7%) answered “7 or more times/day.” Studies have shown that children with enuresis tend to void more often than normal children, and 20% to 30% of children with DUI have increased daytime urinary frequency. Kajiwara et al 16 demonstrated that 26.8% of children with DUI have frequent voiding. Although, a study conducted by Hansen et al 24 found no correlation between urinary frequency and daytime/night-time wetting. When asked if the child strains to void or experiences any pain while voiding, 5.3% and 4.1% answered yes to these questions, 24 respectively. Our study demonstrated that 111 (65.7%) have holding postures, and 92 (54.4%) void urgently. Multiple studies have proved that holding postures, frequency, and urgency impacted on daytime urinary frequency.15,25 Hansen et al 24 also revealed that micturition symptoms such as: straining, running to the toilet, revisiting the toilet soon after voiding and intermittency were significantly associated with daytime urinary incontinence in comparison to those without those symptoms.
Studies have shown that urinary incontinence significantly impacts on the affected children’s quality of life and a tremendous effect on their families’ dynamics and function. Therefore, early recognition and intervention are critical to curtail these impacts. 26 In our study, 75.7% were not at all affected by the condition and only 7.1% were seriously affected. These findings may be due to our cultural background, a lack of awareness on how to deal with such conditions, and possibly the fear of stigma.
Lastly, the discussion turns to a new study 27 examining innovative technologies for addressing nocturnal enuresis (NE), with a particular emphasis on an advanced autonomous system in the field of Advanced Mechatronics Systems (AMS). This technology implements a sophisticated method to tackle bedwetting by proactively indicating the need to urinate, taking into account specific the biological traits of each individual. The AMS gadget, which is compactly housed, combines measurements of bladder fullness, expansion, and emptiness. It also includes user-friendly interfaces specifically designed for children to use without adult supervision. This revolutionary technology represents a notable breakthrough in the early identification of bladder voiding, employing advanced bladder volume monitoring to notify users and avert accidents. An improved early warning system holds the potential to assist children in acquiring bladder control and decreasing occurrences of nocturnal enuresis (NE). The inclusion of single-element MEMS sensors amplifies the simplicity, safety, cost-effectiveness, and user-friendliness of the approach, underscoring its potential efficacy in clinical applications.
Limitations and strengths of the study
Our study had some limitations. Some questionnaires were completed online and some face to face. Mothers may have been more honest online. However, face-to-face questioners may have been better able to clarify questions about the items. Our sample size was small due to restrictions on in-person school attendance due to conflict in Palestine at the time of the study. We did not enquire about parents’ voiding habits during their childhood, so we could not investigate the association between VD in children and that of their parents. In addition, VD was the parental report from the questionnaire and not validated by medical records or clinical evaluation. Despite these limitations, this study is the first on this topic in Palestine and is a starting point for the preventing and treating VD. It provides a baseline for educating primary care physicians about screening families to help patients and their children deal with the issue.
Conclusion
Our study estimates the prevalence of VD and NE among primary-school aged children in Nablus Palestine. VD is a common health problem among children with dysfunctional voiding occurring in over a quarter of all participants (26.6%) and more than half of those under the age of 7 years (55.6%). In order to effectively resolve these findings, we suggest the implementation of educational programs that are designed to increase awareness of the risk factors associated with children’s voiding issues. Furthermore, the implementation of more extensive screenings at schools can facilitate early detection and intervention. Physicians are crucial in this initiative by providing parents with critical information regarding the management of these conditions and by implementing the requisite therapeutic measures to address VD and NE. Additionally, our research has the potential to inform the development of comparable studies by delineating effective methodologies and emphasizing critical findings that are pertinent to public health strategies. Finally, Health care Policymakers can optimize health outcomes for children affected by VD and NE by reallocating resources toward preventative healthcare measures and targeted interventions, as a result of these insights.