
Abstract
Introduction
Nocturnal enuresis is involuntary urination while sleeping after a certain age, usually five years, when children should have established bladder control. The prevalence has been found to be up to 20% in five year old children, and it is considered the most common urological childhood complication.
Material and Methods
This study was conducted on Makassed School children aged 5–18 years. This was a two-step study, the first step was a questionnaire distributed to the children to be answered by their parents. The second step included individually meeting with every child who met the inclusion criteria and his/her parents and physically examining the child.
Results
11,440 questionnaires were distributed to school children aged 5–18 years, to be answered by their parents. Of the 7270 parents who responded back, 6620 reported no enuresis, 90 (1.25%) reported only diurnal enuresis, 107 (1.5%) reported diurnal and nocturnal enuresis, and 453 parents reported their child having nocturnal enuresis only. The data collected was analyzed according to age, sex, area, body mass index (BMI), and the PMQOL-SF score. The prevalence of mono-symptomatic nocturnal enuresis (MNE) in Lebanon was found to be 5.3%. The results showed that the prevalence of MNE is inversely proportional to age. The prevalence of male to female ratio was 1.4:1. As for the prevalence according to different geographic areas, the results have shown that the North had the majority of cases with 7.6% prevalence. Results showed that 82.4% of children had a score more than 50, and only 28% of parents had a score above 50.
Discussion
The prevalence of nocturnal enuresis in Lebanon is lower than that in neighboring countries such as Turkey 8 and Saudi Arabia, 9 but higher than that in Italy 10 and Hong Kong. Our study has managed to show the same results, with a peak in incidence at seven years then dropping back to 0% at the age of 16. Our study has shown a male to female predominance but the male to female ratio was 1.4:1, a value lower than that described in earlier studies. Our study has shown that more than 80% of children were psychologically affected whereas only less than 30% of parents were affected.
Conclusion
To our knowledge, this was the first study in Lebanon conducted to determine the prevalence of MNE. The relatively low prevalence rate found may be because of differences in genetic predisposition, psychosocial or environmental conditions, and traditional and cultural backgrounds. No relation was found between obesity and nocturnal enuresis. The psychological impact on children is significant but that on the parents is minimal.
Introduction
Nocturnal enuresis is included as a disease in ICD-10 under the code of F98.0. It is involuntary urination while sleeping after a certain age, usually five years, when children should have established bladder control. The prevalence has been found to be up to 20% in five year old children, 1 this number decreases as children become older, and it is considered the most common urological childhood complication. 2
Previous studies were conducted on children between 6 and 12 years of age, and showed a prevalence of 0.2–9.0% (daytime incontinence), 1.5–2.8% (combined daytime and nighttime incontinence), and 1.5–8.9% [mono-symptomatic nocturnal enuresis (MNE)], respectively. 3
The prevalence of MNE has been studied in multiple regions and countries, and values have varied according to what is thought to be a difference in attitude and expectations towards this problem. The MNE prevalence was reported as following: 18.6% in India, 3.8% in Italy, 9.2% in Korea, 8% in Malaysia, 5.5% in Taiwan, 4.2% in Thailand, 12.4% in Turkey, 18.9% in Australia, 15% in Saudi Arabia, 3.5% in Hong Kong, 6% in The Netherlands, 7.4% in New Zealand, 13.7% in Sudan, and 6.8% in Iran. 4
The values varied significantly between two neighboring countries such as Turkey (18.9%) and Iran (6.8%), which shows that every country has an individual prevalence.
Nocturnal enuresis has been found to be related to obesity, with around 31% of children with nocturnal enuresis being obese. 5
It is an important public health problem that has been linked with considerable distress to children and their parents, also nocturnal enuresis has been found to cause psychological side effects, especially low self esteem. 6
Aim
The aim of this study is to determine the prevalence of nocturnal enuresis, asses its relation with obesity, and evaluate its psychological effects on Lebanese children and their families.
Material and Methods
This study was conducted on children of Makassed School aged 5–18 years. A total of 32 schools spread across Lebanon were included and divided into four regions: Beirut (the capital), North, South, and Bekaa.
This was a two-step study; after IRB approval was obtained, the first step was a questionnaire distributed to the children to be answered by their parents. This questionnaire asked about the presence of enuresis, and if present, whether it occurs during the day only, at night only, or day and night. Also, the parents were asked to specify the weight and height of their children, and whether either parent had nocturnal enuresis while growing up. These questioners were analyzed and only the individuals with enuresis at night were included in the second part of the study.
The second step included individually meeting with every child who met the inclusion criteria and his/her parents and physically examining the child for any anatomical cause of enuresis. His weight and height were measured, and a urine analysis using a urine dipstick (Compur 10™) was done. The presence of leukocyte esterase or nitrites in urine would render it an abnormal urine analysis and that child was excluded from the study. 7
The rest had their parents fill out another questionnaire, the Short Form of the Pediatric Enuresis Module on Quality of Life™ (PEMQOL-SF), which is a certified questionnaire made up of 16 questions, 7 questions concerning the effect of enuresis on the child and 9 questions concerning its effect on the parents. 3 Data from this questionnaire, concerning the psychological impact on the child and parents, were analyzed and compared with results of the same module from other studies.
Results
A total of 11,440 questionnaires were distributed to school children aged 5–18 years, to be answered by their parents. Each questionnaire had questions concerning the child's age, sex, weight, height, and whether the child has enuresis of any type. The questionnaire also served as a written consent form, by which the parents were informed about the study and were asked for their signature of consent. Out of the 7270 parents who responded back, 6620 reported no enuresis, 90 (1.25%) reported only diurnal enuresis, 107 (1.5%) reported diurnal and nocturnal enuresis, and 453 parents reported their child as having nocturnal enuresis only.
Parents of children with MNE were then contacted and a meeting was arranged with them and their children. These children were examined for any obvious anatomical anomaly, and if present, were excluded from the study, also their weight and height were measured accurately and the body mass index (BMI) was calculated. A urine analysis was performed on every one of these children using a urine dipstick (COMPUR 10™). Children whose urine analysis was leukocyte esterase positive or nitrites positive were excluded from the study to eliminate the possibility of a urinary tract infection as the cause of their enuresis. Out of the 453 children, 74 were excluded, 68 had abnormal urine analysis, 1 had hypospadias, and 5 stated that they misunderstood the questionnaire and that their child had no problem.
The remaining 379 (5.3%) patients met all inclusion criteria and were included in the study. Their parents had to fill out the PEMQOL-SF, a 16-question tool used to assess the psychological impact of enuresis on children and their families.
The data collected were analyzed according to age, sex, area, BMI, and the PMQOL-SF score. The prevalence of MNE in Lebanon was found to be 5.3%. The results showed that the prevalence of MNE is inversely proportional to age with an exception of a rise in the incidence to 10.6% at age of seven years compared to 7.8% at age of five years; after seven years the incidence decreases gradually and becomes almost 0% at the age of 16 years (Fig. 1). The prevalence of male to female ratio was 1.4:1. As for the prevalence according to different geographic areas, the results have shown that the North had the majority of cases with 7.6% prevalence, Bekaa had 4.7%, Beirut 3.7%, and the South 3.2% (Table 1).

Prevalence of MNE vs. age.
Epidemiology of nocturnal enuresis.

Regarding the effect of obesity on nocturnal enuresis, BMI was calculated on subjects with and without nocturnal enuresis (as control), BMI was plotted on the CDC BMI curves for sex and age and obese children were considered the ones above the 95%. Comparison was done and showed that 8% of normal population had obesity, and 10.2% of children with nocturnal enuresis had obesity, which is higher but not significant (
Prevalence of MNE by BMI category.

The results from the PEMQOL-SF were divided to seven questions for the children's score and nine questions for the family's score, a score more than 50 was considered as a significant effect on psychological well being. Results showed that 82.4% of children had a score more than 50, and only 28% of parents had a score above 50 (Table 3).
PEMQOL-SF score for child and parents.
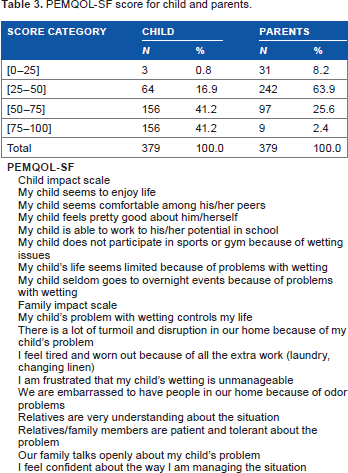
Child impact scale My child seems to enjoy life My child seems comfortable among his/her peers My child feels pretty good about him/herself My child is able to work to his/her potential in school My child does not participate in sports or gym because of wetting issues My child's life seems limited because of problems with wetting My child seldom goes to overnight events because of problems with wetting Family impact scale My child's problem with wetting controls my life There is a lot of turmoil and disruption in our home because of my child's problem I feel tired and worn out because of all the extra work (laundry, changing linen) I am frustrated that my child's wetting is unmanageable We are embarrassed to have people in our home because of odor problems Relatives are very understanding about the situation Relatives/family members are patient and tolerant about the problem Our family talks openly about my child's problem I feel confident about the way I am managing the situation
Discussion
Nocturnal enuresis is known to be a worldwide problem, but still there is some controversy about its prevalence. Several studies have been conducted worldwide, and large differences have been noticed even among countries in the same geographic region. Its correlation to obesity has been discussed in some studies, and its psychological impact on the children and their families have been considered a burden on the community. The problem lies within the norms and culture of certain populations such as ours, where such a problem is sometimes dealt with as a taboo and thereby is not addressed to, or is dealt with as something very minor and not requiring any kind of intervention. This leads to more psychological burden on the child who is either pressured by being scorned and hit by his parents, who are unwilling to admit that he has a problem or verbally abused by his siblings and peers.
In this study a questionnaire was made that contained simple and straight forward questions. The questionnaire was distributed to 15 random mothers at first to assess the clarity of its questions. The questionnaire required the parents to provide information about the age, weight, height, enuresis status, and several other factors regarding the wellbeing of the child. A consent clause was included at the bottom of the questionnaire and was signed by the parents. The sample size was adequate to estimate the prevalence with acceptable accuracy. The country was divided to four regions, having more or less different norms and values, to avoid any selection bias.
The prevalence of MNE was found to be 5.3%, where as those with diurnal enuresis was 1.25%, and both (diurnal and nocturnal enuresis) was 1.5%. The prevalence of nocturnal enuresis in Lebanon is lower than that in nearby countries such as Turkey, 8 and Saudi Arabia, 9 but higher than that in Italy 10 and Hong Kong. 11 The difference in the prevalence may be because of the different definitions used in different studies; some studies defined nocturnal enuresis as occurring once in a three month period, which cannot be used in Lebanon where once a month is not considered an issue. Moreover, the fact that some people consider this as a taboo and thus deny it in their children would lower the prevalence compared to countries that are more open to such a problem.
Several studies have shown that nocturnal enuresis decreases with age,12,13 and our study has managed to show the same results, with a peak in incidence at seven years and then dropping back to 0% at the age of 16 (Fig. 1), which might be an accidental finding. Studies suggested that boys are three times more likely to wet their beds than girls, 14 our study has shown a male to female predominance but in a ratio lower than that described, the male to female ratio was 1.4:1. There was a difference in prevalence from one region to another with the North having 7.6% prevalence compared to 4.7%, 3.7%, and 3.2% in Bekaa, Beirut, and South, respectively. This difference was explained by Safarinejad et al., 4 who found a direct relation between low socioeconomic status and increased number of family members and increased prevalence of MNE. These criteria fit that of the North and Bekaa that have lower socioeconomic status and more children compared to Beirut and the South. As for the correlation between obesity and nocturnal enuresis, studies have shown that obesity increases the incidence of nocturnal enuresis. 15 Our study, however, failed to establish such a relation, obesity was found in 8% of normal population and 10.2% of patients with nocturnal enuresis; although there is a higher incidence, it is not significant. The two studies compared5,15 reported a direct correlation between obesity and nocturnal enuresis; such a correlation could not be established in our study. Further studies should be done with comparison to the normal population to either confirm or refute such a relation.
The psychological effect of nocturnal enuresis has been established in several studies. Landgarf et al in 2004 created the Pediatric Enuresis Module on Quality of Life™ (PEMQOL to assess the effect of enuresis on the children and their families. 16 From this original instrument, the PEMQOL Short Form or PEMQOL-SF was formed and was tested and validated by Landgarf in 2007. 17 We used the PEMQOL-SF on the parents of the included children. Results were split according to the questions into two groups, one was the effect on children and the other was the effect on the family. The previously conducted studies addressing these issues have always shown a significant effect, and that the children and their families alike were affected. 18–21 Our study has shown that more than 80% of children were psychologically affected whereas only less than 30% of parents were affected. This can be explained by two hypotheses; one is the fact that a large number of parents do not consider it as a major problem and tend to deal with it by simply letting their child wear diapers, the second hypothesis is that some parents consider it as a normal phase of development, and something that is common in the family and they will grow out of. This is a major concern, as the parents will not try to address this issue as a problem and thereby not try to solve it, causing the child to deal with it alone without any help or support. This has been reported by Scholmer Bet et al but to a lesser extent, with 45% of parents not considering treatment for their enuretic children. 22
The Makassed Health Care Bureau received the collected data, and promised to start immediate awareness campaigns with the possibility of providing treatment modalities if needed.
Limitations
The number of enuretic children could have been greater, had all parents replied to the questionnaire distributed to them. The second limitation was that teenage students were embarrassed by the questionnaire and failed to deliver it to their parents. The last limitation was that urine culture would have been more specific for accurately detecting the cases of urinary tract infection.
Conclusion
To our knowledge, this was the first study in Lebanon conducted to determine the prevalence of MNE. The relatively low prevalence rate found compared to those reported from other countries may be because of differences in genetic predisposition, psychosocial or environmental conditions, and traditional and cultural backgrounds. No relation was found between obesity and nocturnal enuresis. The psychological impact on children is significant but has minimal impact on the parents, and thus the parents do not consider it as a problem. Governmental and non-governmental organizations should put efforts into seminars and awareness campaigns, to educate the community and inform the parents about MNE as a treatable disease, and its psychological impact on their children's life.
Author Contributions
Conceived and designed the experiments: BAM, AH, FZ, RK, MR. Analyzed the data: BAM, AH, FZ, RK, MR. Wrote the first draft of the manuscript: MAM. Contributed to the writing of the manuscript: BAM, AH, FZ, RK, MR. Agree with manuscript results and conclusions: BAM, AH, FZ, RK, MR. Made critical revisions and approved final version: BAM, AH, FZ, RK, MR. All authors reviewed and approved of the final manuscript.