
Abstract
Background:
Caregivers are deeply concerned about children achieving independent walking, and evidence-based rehabilitation support is beneficial. However, current research is confined to a single study on spina bifida aperta, leaving a gap in understanding the timing of independent walking for lumbosacral lipomas.
Objectives:
This study aimed to examine the factors influencing independent walking in children with lumbosacral lipomas.
Design:
Retrospective cohort study.
Methods:
This retrospective cohort study included 124 children who underwent untethering surgery for lumbosacral lipomas. The age (in months) at which the children walked independently was used as the primary endpoint, and potential influencing factors, including the type of spinal lipoma, extent of lipoma removal, magnetic resonance imaging features, congenital anomaly complications, urinary/defecation management requirements, foot/toe symptoms, and orthotic device fabrications were analyzed.
Results:
Multiple logistic regression analysis showed that the most significant influencing factor for delayed independent walking was the presence of systemic combined anomalies (adjusted odds ratio = 15.5, P < .001), while non-systemic malformations, such as suburethral cleft, had limited effects. A subgroup analysis of 94 patients without systemic combined anomalies showed that the presence of a malformed conus medullaris was significantly associated with delayed independent walking (P = .014). The median age of independent walking in children with Morota’s classification type 2 was 14 months, which is 1 month later compared to other types, although this difference was not significant (P = .055).
Conclusion:
Our findings suggest that complications arising from systemic combined anomalies and the presence of malformed conus medullaris are influencing factors in delays in independent walking in children with untethered lumbosacral lipomas.
Keywords
Introduction
Spina bifida aperta has long been studied, with the site of origin and the degree of neurological impairment determining future function.1 -3 Recently, postoperative motor function in lumbosacral lipomas and spina bifida occulta has been widely reported, with most children achieving ambulation in early childhood. 4 de Vloo et al 5 reported that 56% of 91 patients with lumbosacral lipomas who underwent radical resections had normal motor function, 32% had slight muscle weakness or delayed milestones but did not require walking aids, and the remaining 12% required walking aids. Thuy et al 6 reported that 11 of 63 patients who underwent untethering had motor weakness or gait disturbances. Koyanagi et al 7 found motor deficits in 9 of 34 patients who underwent detethering, of whom 7 had lipomas that extended beyond the L5 level of the spine and were of the transitional type, which was more likely to result in severe motor deficits. Other lumbosacral lipomas have been reported to have different neurological prognoses depending on their location and size; however, none of these studies clearly state whether independent walking can be achieved.8 -15
Acquiring independent walking is a major concern of caregivers, and presenting evidence-based rehabilitation support is useful for affected children. However, recent studies on the timing of independent walking are limited to only 1 report on spina bifida apertam, 16 and there is a lack of studies investigating this in lumbosacral lipomas. Therefore, we conducted a retrospective cohort study of children with untethered lumbosacral lipomas at the Aichi Children’s Health and Medical Center (ACHMC) to identify factors influencing delays in acquiring independent walking.
Methods
Recruitment of participants
This was a retrospective cohort study. The study population consisted of all children who underwent untethering surgery for lumbosacral lipomas between February 2016 and February 2021 at the ACHMC.
Exclusion criteria were (1) different pathology, (2) additional operations, (3) moved away (relocation), (4) died in infancy, and (5) lack of walking data.
Primary endpoints
The primary outcome was the age at which independent walking was achieved. The age in months was extracted from the medical records, which were transferred from the records of the maternal and child health handbook. 17 The ages of preterm infants were expressed as corrected ages in months. 18 Cohort entry was set at birth, and the primary follow-up concluded 1-month post-independence. Requirement of orthotic devices was not a condition for acquiring independent walking. Children unable to achieve independent walking by 60 months of age were classified as unconfirmed cases.
Based on the World Health Organization’s motor development milestones 19 and recent studies on normal development in Japanese children, 20 we divided the subjects into normal (independent walking acquired before 15 months of age), borderline (independent walking acquired between 15 and 18 months of age), and delayed (independent walking acquired after 18 months or older, including unconfirmed cases) groups.
Examination of influencing factors
Data on sex, gestational age, birthweight, small for gestational age (SGA), 21 age at untethering (in months), timing of untethering (before or after independent walking), type of spinal lipoma, extent of lipoma removal, magnetic resonance imaging (MRI) findings (syrinx, low-set conus medullaris, and malformed conus medullaris), congenital anomaly complications, urinary and defecation management requirements, foot and toe symptoms, and orthotic device fabrications were extracted from the medical records.
The classification of spinal lipoma types followed the Morota’s classification by Morota et al. 22 This classification delineates types 1 to 4 based on the conus medullaris and lipoma’s location using MRI features, and these types were established by 2 or more expert neurosurgeons and were confirmed through intraoperative findings. The extent of lipoma removal was categorized as “total removal,” “partial removal,” or “conservative untethering” (which involves untethering without lipoma removal), based on details from surgical records. For congenital anomaly complications, patients with 1 or 2 of the 4 categories of malformations—(1) anorectal anomalies such as anal atresia, (2) urogenital anomalies such as hypospadias, (3) sacral anomalies, or (4) minor anomalies such as congenital hydronephrosis and some congenital malformations around the pelvic/perineal region—were classified as having “associated/minor malformations.” Those with 3 or more malformations, including associated/minor malformations, anomaly syndromes such as VACTERL (vertebral defects, anal atresia, cardiac defects, trachea-esophageal fistula, renal abnormalities, and limb abnormalities), congenital heart diseases, congenital strabismus/amblyopia and other non-secondary syndromes with potential implications for delays in motor development, were classified as having “systemic combined anomalies.”22 -24
For urinary and defecation management, the designation “yes” applied to patients requiring drug intervention for incontinence or urinary retention, daily urinary drainage, routine hostile stool management (enema or swab stimulation), or treatment involving bisacodyl or magnesium oxide. These classifications and definitions were obtained and recorded by expert urologists after untethering. Regarding foot and toe symptoms, the label “yes” was assigned if patients exhibited any of the following descriptions: talipes valgus, varus, planus, equinus, cavus, or calcaneus, mallet toes, or an inability to spread toes. Data on foot and toe symptoms were collected after 12 months of independent walking.
Statistical analysis
Multiple logistic regression analyses were performed, with both “the normal versus borderline and delayed groups” and “normal and borderline versus delayed groups” as objective variables (binary variables) and sex, gestational age, SGA, and congenital anomaly complications (associated/minor malformations and systemic combined anomalies) as explanatory variables.
For the subgroup analysis in those without systemic combined anomalies, multiple regression analysis was performed with age of independent walking (in months) as the objective variable (continuous variable) and 6 items—sex, extent of lipoma removal, congenital anomaly complications (associated/minor malformations), and 3 MRI findings (syrinx, low-set conus medullaris, and malformed conus medullaris) that were used as criteria for determining the Morota’s classification type—as explanatory variables.
In the subgroups, comparisons based on the Morota’s classification types were conducted using Fisher’s exact or Kruskal-Wallis tests for each examination factor and log-rank tests for the cumulative incidence of achievement of independent walking.
All statistical analyses were performed using R ver. 4.3.0, R Commander ver. 2.8-0, and the plug-in EZR ver. 1.61 for Windows. 25
Post hoc power analyses for predictor analysis were conducted to verify the sample size using G*Power 3.1.9.7. 26 The alpha level used for this study was P < .05.
Ethics
The study was approved by the Ethics Committee of the ACHMC (approval number 2021093) and the Bioethics Committee of Nagoya University (approval number 22-501). As this was a study involving the secondary use of existing data, the requirement for individual consent was waived.
Results
Intraspinal operations for neural tube defects were performed in 165 children during the study period. Among these children, 26 had myelomeningoceles, 5 had a different pathological diagnosis of spinal lipoma, 8 had no information on when they achieved ambulation due to unrecorded data, and 2 had additional operations performed; thus, 124 children—73 in the normal, 26 in the borderline, and 25 in the delayed groups—were included (Figure 1). The patients’ backgrounds and clinical characteristics are listed in Table 1. The median age at untethering was 9.9 months, and 65% of patients were untethered before independent walking. The median age of independent walking was 14 months. The acquisition status of independent walking in the included patients is shown in a histogram in Figure 2.
Characteristics of the study population (n = 124).
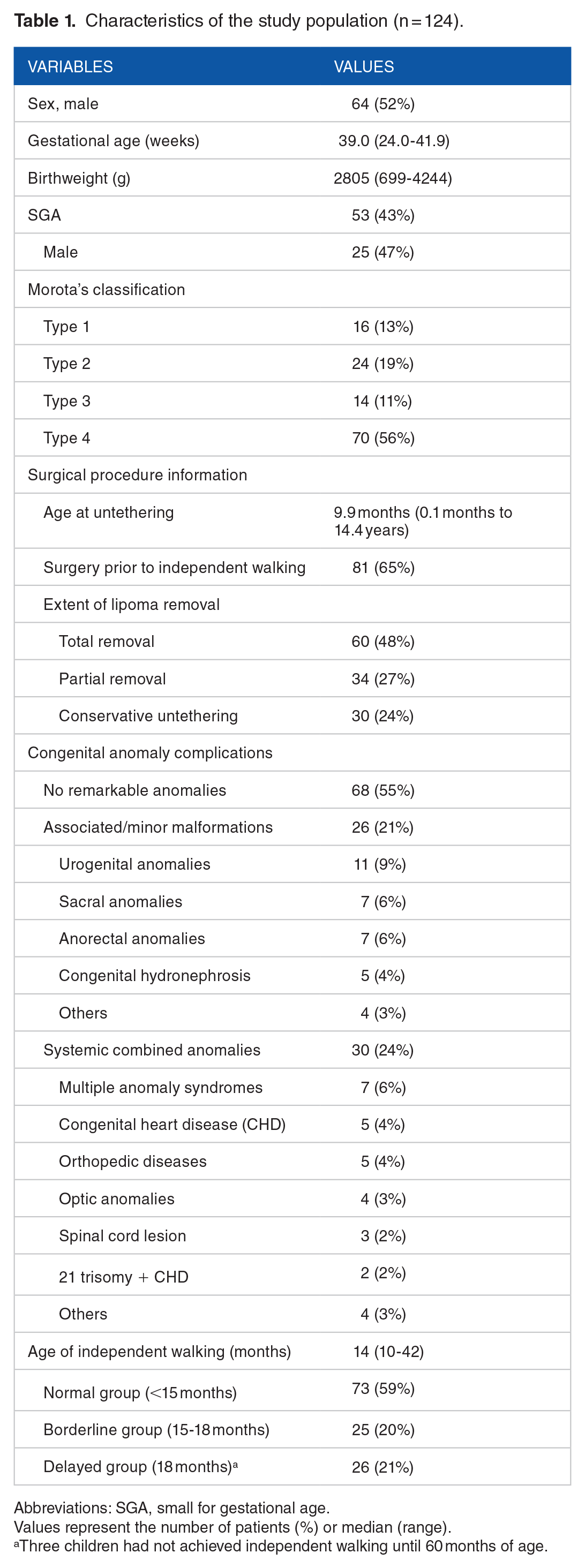
Abbreviations: SGA, small for gestational age.
Values represent the number of patients (%) or median (range).
Three children had not achieved independent walking until 60 months of age.
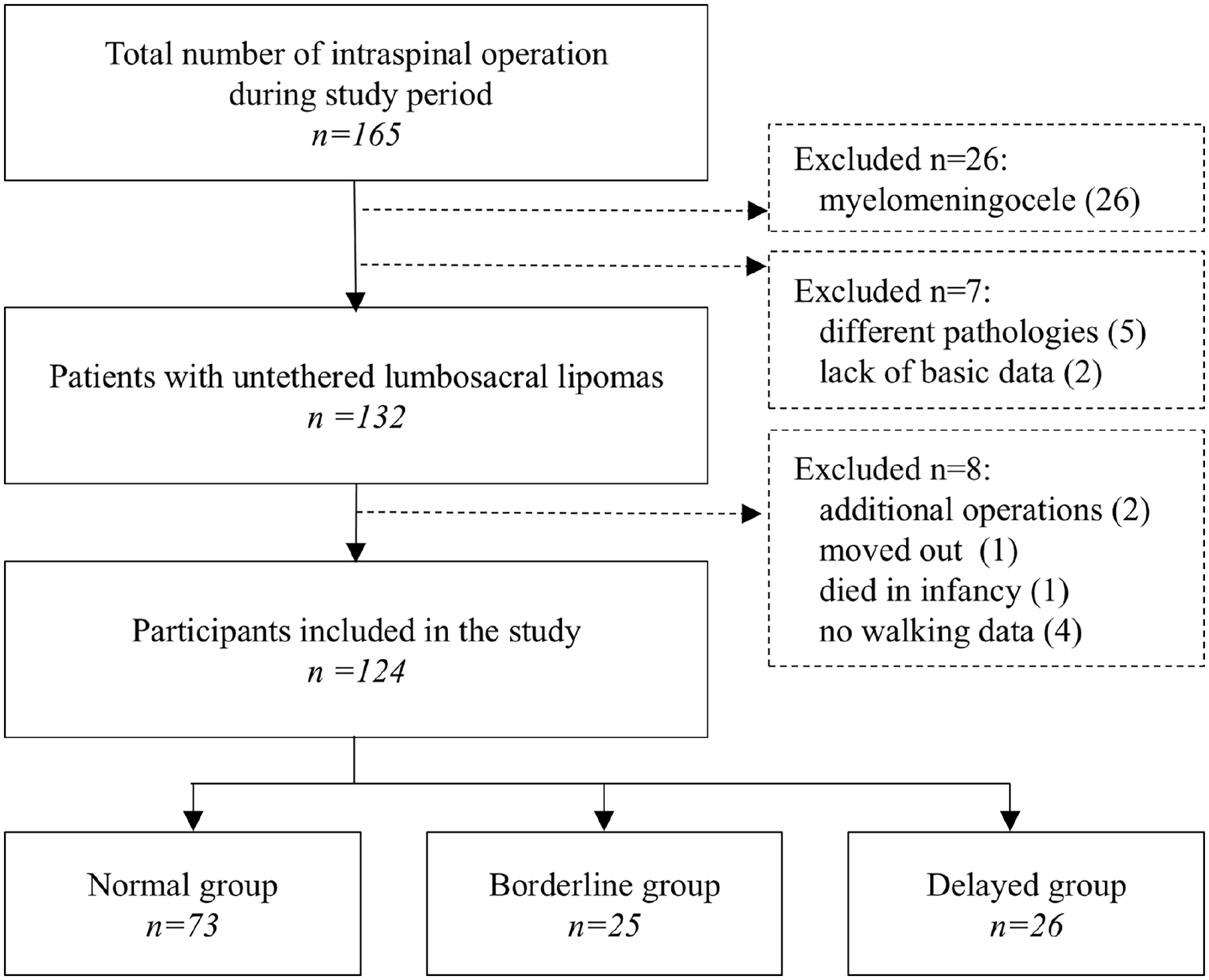
Participant recruitment and inclusion criteria.

Histogram of achieved independent walking ages in months. The histogram is segmented into 3 distinct groups: normal, borderline, and delayed, each demarcated by dotted lines. Unconfirmed cases were included in the delayed group.
Factors influencing the timing of independent walking
Multiple logistic regression analyses showed that systemic combined anomaly complications were significantly associated with the age of independent walking in the delayed group, with adjusted odds ratios (OR) of 15.5 (normal vs borderline/delayed) and 43.2 (normal/borderline vs delayed) (Table 2). Sensitivity analyses were performed excluding 3 unconfirmed cases, with similar results (ORs of 13.7 and 36.7, respectively). No other items were significantly associated with the age of independent walking. The cumulative incidence of achievement of independent walking in those with congenital anomaly complications is shown in Figure 3.
Significant variables between normal group versus delayed/borderline group and normal/borderline group versus delayed group.
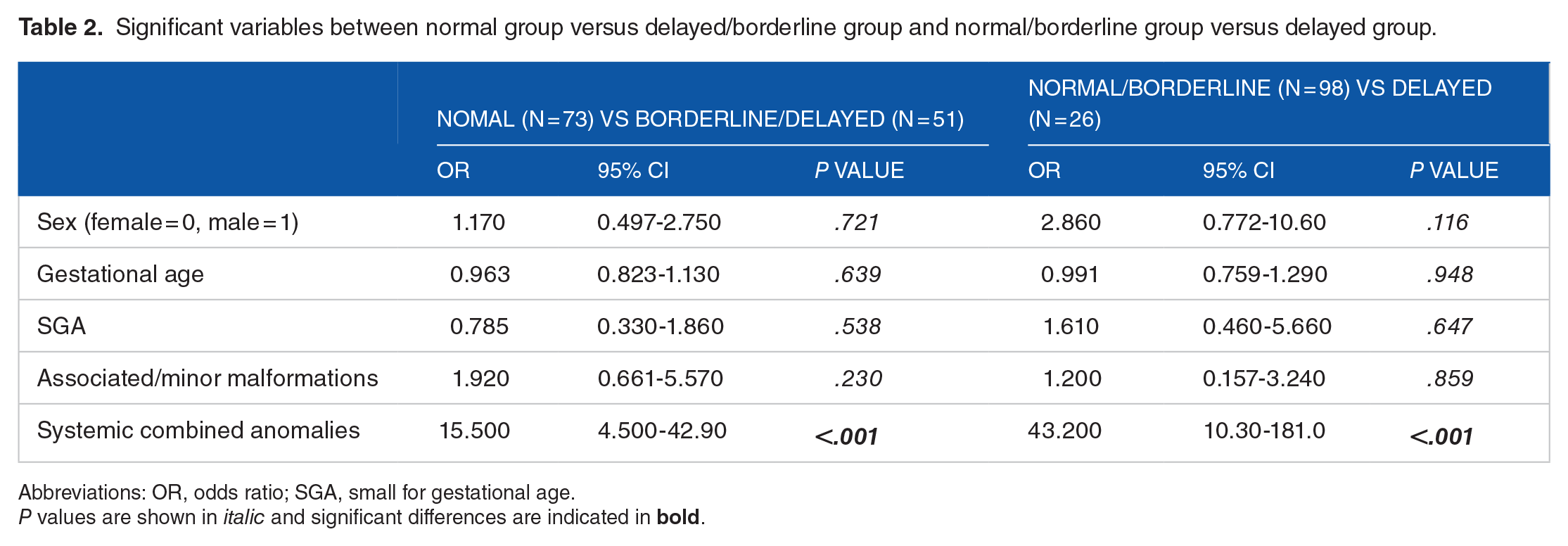
Abbreviations: OR, odds ratio; SGA, small for gestational age.
P values are shown in italic and significant differences are indicated in bold.

Cumulative incidence of independent walking achievement according to congenital anomaly complications. Ninety percent of children in the groups with no remarkable anomalies and associated/minor malformations achieved independent walking by 15 months of age. However, in the systemic combined anomalies group, this achievement was observed in less than 25% of children by the same age milestone. The 90th percentile for the achievement of independent walking in the systemic combined anomalies group was more than 40 months (P < 0.001).
The post hoc power values of the total sample size of 124 were 98%, 84%, and 71% for effect sizes assumed to be OR = 2.6, 2.0, and 1.8, respectively. Thus, ORs of 2.6 and over for logistic regression analysis in this study were valid to detect statistically significant differences.
Subgroup analyses were performed on 94 cases with no remarkable anomalies or associated/minor malformations. In the single regression analysis, malformed conus medullaris, urinary management, and toe symptoms were associated with delayed achievement of independent walking, whereas other factors were not associated. In the multiple regression analysis, which included 6 indicators (sex, associated/minor malformations, extent of lipoma removal, and the 3 MRI findings of syrinx, low-set conus medullaris, and malformed conus medullaris), only the presence of a malformed conus medullaris was significantly associated with the delayed achievement of independent walking (Table 3).
Univariate and multivariate analyses of factors influencing the achievement of independent walking (excluding children with systemic combined anomalies).

Abbreviations: CI, confidence interval; SGA, small for gestational age.
The values of these items were assigned binary scales of 0 or 1.
The binary scale employs “1” to represent total removal and “0” to signify partial removal and conservative untethering.
P values are shown in italic and significant differences are indicated in bold.
The post hoc power values of a sample size of a subgroup of 94 with 6 predictors (independent variables) for multiple regression analysis were 99% and 78% for effect sizes assumed to be large (f 2 = 0.35) and medium (f 2 = 0.15), respectively. The number of subjects used for subgroup analysis was therefore sufficiently large to detect statistically significant differences.
Comparison according to Morota’s classification types
The comparison based on Morota’s classification types in the subgroups without systemic combined anomalies is presented in Table 4. Type 2 cases tended to have an earlier age at untethering surgery (significantly or marginal significantly), with all procedures conducted before the achievement of independent walking. In addition, 62% of type 2 cases presented with lipomyelomeningoceles, and this subgroup exhibited the lowest rate of total removal of lipoma at 33%.
Comparison of lumbosacral lipoma patient characteristics based on Morota’s classification types (excluding children with systemic combined anomalies).

Abbreviations: MRI, magnetic resonance imaging; SGA, small for gestational age.
Values represent the number of patients (%) or the median (range).
Categorical variables were compared using Fisher’s exact test.
Continuous variables were compared using the Kruskal-Wallis test.
Multiple comparisons were made using the Bonferroni method for categorical variables and Mann-Whitney test for continuous variables. Those significantly different from type 1 are indicated by “a,” type 2 by “b,” type 3 by “c,” and type 4 by “d,” respectively.
P values are shown in italic and significant differences are indicated in bold.
MRI findings indicated an increased prevalence of syrinx and low-set conus medullaris in most cases compared to type 4 cases. Moreover, significant variations were observed among types in terms of urinary management, foot/toe symptoms, and orthotic device fabrications.
Comparisons were conducted among the Morota’s classification types regarding the age in months for independent walking. Out of the cases, 14 belonged to type 1, 12 to type 3, and 47 to type 4, with a median age of independent walking of 13 months (ranges, 10-17, 11-15, and 10-18, respectively). Meanwhile, the 21 cases classified as type 2 achieved independent walking at a median age of 14 months (range, 11-20), which was slight later. Additionally, a delay in cumulative incidence was also observed in these cases, but this difference was not statistically significant (P = .055, Figure 4).

Cumulative incidence of achievement of independent walking stratified by Morota’s classification types. Morota type 2 exhibited a delayed cumulative incidence in comparison to the other 3 types. However, the log-rank test did not reveal a significant difference (P = 0.055).
Discussion
The retrospective cohort study showed that the presence of systemic combined anomalies was the strongest factor associated with delayed achievement of independent walking in children with untethered lumbosacral lipomas, while the presence of a malformed conus medullaris was a possible factor. This study is the first of its kind to pinpoint potential risk factors associated with the delayed attainment of independent walking. Such findings hold valuable information for the families of patients and contribute to enhancing their understanding of the condition.
The purpose of the first statistical analysis was to exclude children whose delayed independent walking was not due to the pathogenesis of spinal lipoma. Forty-five percent of the subjects in this study exhibited some sort of malformation complication. To avoid the exclusion of all cases with malformation complications, complications were separated according to their severity. The study identified a delay in achieving independent walking in children with systemic combined anomalies, a finding that aligns with several existing reports.27,28 Simultaneously, associated anomalies such as anorectal or urogenital malformations appeared to be limited risk factors for delayed independent walking. This observation cannot be definitively confirmed due to the lack of relevant perspective reports. Given that congenital anomaly complications within spinal lipoma, stemming from neural tube defects, are relatively prevalent, the results of this study may be relevant to clinical practice.
Our subgroup analysis aimed to investigate factors within the pathogenesis of spinal lipomas associated with delayed independent walking. The findings indicated that a possible factor contributing to the delay was the presence of a malformed conus medullaris. This specific malformation is inherent in Morota types 2 and 3 according to their definitions.22,29 Notably, type 2 exhibited a delay in independent walking of approximately 1 month, while type 3 did not display such a delay. These observations were comparable to the patterns seen in types 1 and 4. However, the analysis of cumulative incidence did not identify any significant delays (Figure 4). If the majority of cases had been operated on before independent walking achievement, there might have been a significant difference. The primary focus of consideration lies in determining whether the delayed independent walking in the screened children stemmed from a neurogenic motor deficit or not.
Most previous studies assessing neurogenic motor deficits have not focused on independent walking in infancy.5,12,13,30,31 In 1 study, Klain and Thompson 32 reported that a patient who presented with mild neurological signs in infancy, without dysuria, achieved ambulation at 28 months without worsening neurological symptoms. In a different study, Vora et al 33 reported that neurological function was preserved in >90% of radical resections and that early surgical intervention prevented neurological deficits. In addition, Thompson et al 34 emphasized the need for cautious consideration of surgical treatment for Morota’s classification type 1 and cases classified under the dorsal type of the Chapman and Arai classification without informed conus morphology. Collectively, these reports indicate that spinal lipomas over the conus medullaris represent significant risk factors and that appropriate untethering in infancy prevents and improves neurogenic motor deficits, contributing to the achievement of independent walking.
The potential impact of early untethering combined with partial lipoma removal might have been substantial in our Morota type 2 cases, where concerns about neurogenic motor deficits were prominent. This suggests that Morota type 2 cases inherently harbor pathogenic spinal lipoma malformations that contribute to neurogenic symptoms and pose a potential risk for unambiguous total removal. Interestingly, 81% of patients with type 2 also exhibited foot symptoms and motor deficit changes that warrant vigilant long-term observation. Meanwhile, in Morota type 3 cases, defined as the early phase of secondary neurulation failure, there existed a malformed conus medullaris located caudal to the spinal cord, accompanied by neurogenic lower limb deficits that occurred exclusively at the level of the sacral medullary nerve. Thus, it is reasonable to conclude that the presence of symptoms in the toes of 67% of patients with type 3 had minimal impact on the delay in achieving independent walking.
In this study, voiding management was associated with the achievement of independent walking (Table 3). Comparison according to Morota’s classification demonstrated that more than 62% of type 2 patients required urinary management and up to 50% required defecation management in the mid-term period after untethering (Table 4). This incidence aligns with the reported outcomes in children with lipomyelomeningoceles by Vora et al 32 and the surgical outcomes in children with lumbosacral lipomas by Vloo et al. 5 Additionally, foot symptoms were present in three-fourths of Morota type 2 cases, and toe symptoms were present in two-thirds of type 2 and 3 cases. These symptoms are likely related to the involvement of the lumbosacral medullary nerve in the lipoma, supported by MRI findings showing malformed conus medullaris, lipomyelomeningoceles, 35 or frequently, chaotic lipomas. 12 The delay in independent walking in Morota type 2 could be attributed to a neurogenic cause, potentially necessitating urinary management as well. Further research is needed to investigate the relationship between delays in independent walking and other clinical features of lumbosacral lipomas.
Notably, our study also found that associated malformations, such as anorectal and/or urogenital malformations, did not strongly influence the delayed achievement of independent walking, whereas the presence of conus malformations did. Moreover, our findings underscore that the children with systemic combined anomalies experienced developmental delays in motor milestones, highlighting the importance of comprehensive rehabilitation.
Study limitations
The main limitation of the study is that it was retrospective: there were no descriptions of a unified assessment of neurogenic motor deficits, and it is uncertain whether the delay in independent walking was truly due to lower-limb dysfunction. Cognitive components may also be related to motor developmental delays. The timing of untethering surgery may also be a confounding factor in the study population, as there was a mix of patients who underwent surgery before or after independent walking. It is also worth mentioning that a considerable number of children with congenital anomaly complications underwent hospitalization for treatments during infancy. This could potentially contribute to delays in achieving motor developmental milestones. In addition, as this was a cross-sectional study, it was not feasible to explore the impact of the extent of lipoma removal and the symptomatic changes experienced before and after surgery. This underscores the need for future research in this area.
Conclusion
In 94 lumbosacral lipoma cases, excluding children with delayed independent walking due to systemic combined anomalies, it was suggested that the presence of malformed conus medullaris was associated with delayed achievement of independent walking.
This finding will contribute to the development of theoretical implications for these children and their guardians, and will encourage further research to explore the neural pathways linking malformations to motor deficits and assessing the impact of surgical interventions on motor outcomes.
This study thus lays the foundation for targeted interventions and refined rehabilitation approaches, enhancing both clinical practice and patient care.