
Abstract
Background:
Muslim Arab immigrants are a fast-growing, under-studied, and underserved minority population in the United States. Little is known about breastfeeding practices in this population.
objectives:
The objective of this study was to describe infant feeding practices and factors associated with these practices among immigrant Muslim Arab women.
design:
A nonexperimental-one group, cross-sectional, descriptive, prospective design was used to identify infant feeding practices among immigrant Muslim Arab women.
methods:
A convenience sample of one hundred sixteen immigrant Muslim Arab women with at least one child five years or younger was recruited from a large metropolitan area in the Southwestern region. Participants completed the social ecological model of health promotion self-reported questionnaire. Descriptive statistics were performed to identify infant feeding practices and logistic regression was used to identify factors associated with these practices.
results:
Immigrant Muslim Arab mothers demonstrate high breastfeeding initiation rates (99.2%) and lengthy breastfeeding duration (M = 11.86, SD = 8.04), but low rates of exclusive breastfeeding at six months (21.6%). The most frequent reasons for early termination of breastfeeding were perceived insufficient milk (44.4%), child was still hungry after breastfeeding (37.5%), and the belief that the child was old enough to stop breastfeeding (32.9%).
conclusion:
Development of educational interventions are needed to improve breastfeeding exclusivity and raise women’s awareness of the importance of exclusive breastfeeding. Healthcare providers should help women gain confidence in their ability to produce enough milk to successfully continue breastfeeding.
Background
Arab immigrants are a fast-growing, under-studied, and underserved minority population.1,2 The number of immigrant Arabs in the United States (US) increased from 1.1 million in 2000 to 1.9 million in 201. 3 Although immigrant Muslim Arabs represent the fastest growing segment of the Arab American community, little is known about breastfeeding practices of these women and challenges they face to establish successful breastfeeding. In particular, breastfeeding research within the immigrant Muslim Arab population has been misclassified in US national data in the white, non-Hispanic category.4,5 No specific data is known about breastfeeding practices and challenges faced by immigrant Muslim Arab women.
Breastfeeding has a religious context in Arab culture. The Islamic values of Muslim Arab women can play a role in these breastfeeding practices. Islamic laws recommend that a mother breastfeed her child, if possible, for two years and state that newborn infants have a right to be breastfed. Religious teachings are reported as valuable sources of motivation that promote breastfeeding in this group of women.6 -10 Although Muslim Arab mothers are motivated to breastfeed from religious teaching, they often lack the knowledge of exclusive breastfeeding practices or hold cultural myths that hinder successful breastfeeding.11 -13 For example, prelacteal feeding (eg, water, sugar water, salt solution, crushed dates, artificial milk, animal milk, yogurt, gripe water, herbal tea, and black tea) is given for the first three days after delivery based on the belief that it cleanses the bowels of the newborn until the mother produces “white” milk.12,14,15 Prelacteal feeding interferes with exclusive breastfeeding and makes breastfeeding more difficult to establish.
Assessing women’s breastfeeding practices is essential to effectively promoting and supporting successful breastfeeding among this population. The purpose of this study is to describe infant feeding practice among immigrant Muslim Arab women who reside in a metropolitan area of the Southwestern US. The following research questions were posed: (1) What are immigrant Muslim Arab mothers’ infant feeding practices in terms of breastfeeding initiation, duration, and exclusivity at six months? (2) What are the reasons for stopping breastfeeding? And (3) What are the sociodemographic factors (age, income, education, employment, length of stay in US, and religion) associated with exclusive breastfeeding up to six months and breastfeeding duration for more than one year?
Methods
Setting
This study was conducted within a metropolitan area in a state within the southwestern US. According to the Arab American Institute Foundation, 3 the Southwest region of the US has one of the rapidly growing Arab populations in the country with an estimated statewide population of 31,809.
Design
A nonexperimental-one group, cross-sectional, descriptive, prospective design was used to identify infant feeding practices among immigrant Muslim Arab women.
Sample
A convenience sample of Muslim Arab women were invited to participate in this study if they met the following inclusion criteria: (a) Muslim; (b) first-generation immigrant mother from an Arab country; (c) greater than or equal to eighteen years old; (d) living in the Southwest region of the US; (e) have given birth to at least one child in the US within the past five years; and (f) able to read and write in English. If the woman had more than one child, she was asked to give information on her youngest child who was born in the US. Mothers were excluded from participation in this study if they did not meet the inclusion criteria, or if the mother’s youngest baby was a multiple birth, as these mothers are less likely to breastfeed exclusively and more likely to stop breastfeeding early. Data was collected from September 28 to November 4, 2016.
To estimate the proportion of mothers with exclusive breastfeeding at six months, proportions with a 95% confidence interval (CI) were calculated and reported. Assuming a proportion of 0.16 as reported by Saaty et al 16 and setting the width of CI at 0.15, the required sample size was 92. 17
Measurement
This study used a self-reported questionnaire to collect data adapted from Dunn et al, 18 which was reviewed by experts in breastfeeding to establish content validity and by participants from the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) to determine face validity. Dunn et al 18 did not report any reliability for their instrument. Permission to use their questionnaire for this study was granted from the principal researcher, who was contacted through email.
The questionnaire was administrated to Muslim Arab immigrant women in English as it is the dominant language of communication in healthcare and the lack of educational materials in Arabic. The questionnaire was pilot tested to check clarity and the sequence and time needed for completion of questions. The survey was pilot tested using a convenience sample of five Muslim Arab immigrant mothers from the target population and excluded from the findings. No adjustments to the survey were suggested.
The survey questions were composed of two parts: demographic information and infant feeding practices. Sixteen demographic questions were assessed for social and economic characteristics of the sample. Included in the demographic questions are maternal characteristics, such as age in years, marital status, employment status, income, and education. Country of origin was assessed using an open-ended item. Mothers were also asked about their parity, number of years living in the US, the city where they live, whether the child was born at full-term “37+ weeks” (yes or no), and whether their pregnancy was planned or not.
The World Health Organization (WHO) definition for breastfeeding practices was adopted for this study. Infant feeding practices were defined as initiation of breastfeeding after delivery, exclusive breastfeeding until the age of six months, months of exclusivity (if not exclusively breastfeeding for six months as recommended by WHO), and duration of breastfeeding. 19
The infant feeding practice portion of the questionnaire consisted of eleven items related to breastfeeding initiation, exclusivity, duration, and reasons not to breastfeed or terminate breastfeeding. The breastfeeding initiation question asked how soon after delivery the mother breastfed or tried to breastfeed for the first time (within one hour, one to six hours, more than six hours, next day, or can’t remember).
Exclusivity and duration of infant feeding were measured through answers to two questions: “Did you ever supplement with substances other than breast milk like formula, juice, cow’s milk, sugar water, herbal tea, or anything else, even water?” and “How old was your baby the first time he or she had any other liquids or solids, not counting vitamins, minerals or medicines?” Breastfeeding duration was assessed by asking: “How old was your baby when you stopped breastfeeding?” One question included reasons not to breastfeed or for terminating breastfeeding: “Did any of the following reasons influence your decision to not breastfeed or to stop breastfeeding?” Mothers chose from a checklist with seventeen possible reasons, such as “It was easier to give my baby formula,” “I felt more comfortable giving my baby formula,” and “I got free formula from WIC,” “I didn’t want to have to watch what I ate and drank,” and “I don’t have enough milk.”
Religious influence. Two questions addressing the influence of religion on breastfeeding decision were added to the survey by the researcher. Mothers were asked if their religion encouraged them to breastfeed with a response range “yes or no.” An open-ended question “please specify how your religion influenced your breastfeeding decision” was available for participants to describe how their religion influenced their breastfeeding, purely for informational purposes. Content analysis of the written responses was examined to identify patterns and trends in their responses.
Data collection
Participants were recruited from four Muslim community-based organizations, and two Islamic schools. Flyers advertising the study’s objectives, the researcher’s contact information, the study’s online link, and the survey access code were posted in Muslim community centers and schools. In addition, research staff were available in mosques during special community events and during Muslim Friday prayer to administer questionnaires to participants between September and November 2016.
Additional recruitment was done through advertising on the social networking sites (ie, Facebook, WhatsApp). An event page was created on Facebook where interested participants could read about the research and click on a link to take the online survey using the Research Electronic Data Capture (REDCap) system. The online survey allowed participants who do not attend Muslim community organization events to join the study.
Data from online surveys were directly imported into the Statistical Package for the Social Sciences (SPSS) version 23 software program. Written data was transferred into electronic format using a double entry system to reduce rates of error. The principal investigator entered all raw data into REDCap. The principal investigator and one researcher from the team reviewed the data again to identify inconsistencies in data entry.
Data analysis
Descriptive statistics were performed to summarize the demographic data and infant feeding practices, including measures of central tendency (means and standard deviations) and measures of variability (ranges for continuous variables and counts with frequencies for categorical variables). Frequency distribution and percentages were calculated to answer question 2.
To answer research question 3, logistic regression was used to examine relationships between the sociodemographic factors and exclusive breastfeeding of six months and breastfeeding duration (statistical significance set at P < .05 was used to examine the effect of each factor). The dependent variable was classified as either mothers exclusively breastfeeding their infants for six months or not (exclusive breastfeeding = 1 or not = 0). Duration of breastfeeding as the dependent variable was classified breastfeeding for either less than 12 months or 12 months and more (less than 12 months = 0 and ≥12 months = 1). Results are presented as odds ratios and their respective confidence intervals at 95%.
Results
Characteristics of sample
The total number of participants included in the study was one hundred sixteen, sixty-nine (59.5%) participants completed the paper survey, while forty-seven (40.5%) respondents were enrolled online. Table 1 describes the demographic characteristics of participants. The mean age of respondents was 33.1 years (SD = 5.36). Table 2 describes the demographic characteristics of children included in the study. The mean age of children was 28.77 months (SD = 17.60).
Demographic characteristics of the sample (N = 116).
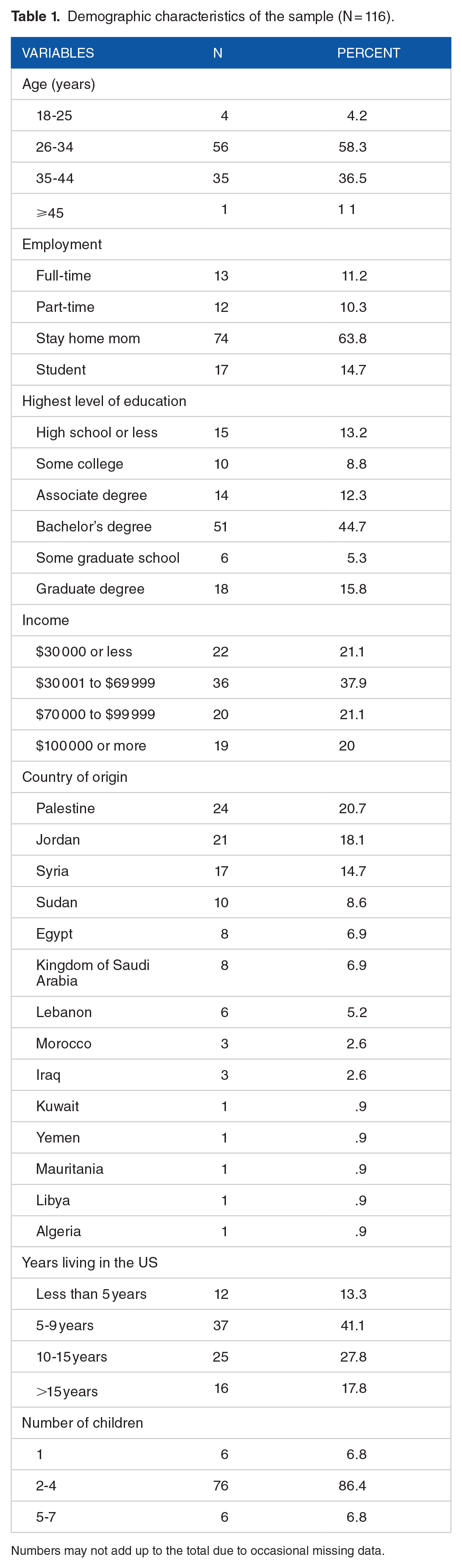
Numbers may not add up to the total due to occasional missing data.
Demographic characteristics of the children included in the study (N = 116).

Numbers may not add up to the total due to occasional missing data.
Infant feeding practices
Findings related to infant feeding practices are grouped into breastfeeding practices (eg, initiation rate and time, exclusivity, and duration) and feeding practices (eg, predominant breastfeeding and mixed feedings). Of the mothers who tried to breastfeed in the hospital (n = 115), 57.5% breastfed their babies within the first hour of birth; whereas, 34% breastfeed their babies within one to six hours. The rest breastfed their babies within the first day after delivery. Breastfeeding practices of the mothers in this study are described in Table 3. The median duration of any breastfeeding was 11.86 months (SD = 8.04) with a wide range varying from one month to thirty-six months.
Breastfeeding practices of the mothers.

Figure 1 illustrates the percentages of feeding practices. For predominant breastfeeding, forty (38.5%) mothers reported use of ritual fluids. The most common used supplemental fluids were herbs (61.30%) and water (22.6%). Almost half (n = 17, 47.2%) of the mothers introduced these fluids during the first month. Sixty-nine mothers reported use of mixed feeding. Of those mothers, 64.4% (n = 38) reported starting supplementary feeding for their babies in the first month. The mean age of formula supplementation was 2.57 months (SD = 3.28). Table 4 summarizes the reasons mothers stopped breastfeeding. The most frequent reasons for early termination of breastfeeding were perceived insufficient milk (44.4%), child was still hungry after breastfeeding (37.5%), and the belief that the child was old enough to stop breastfeeding (32.9%).
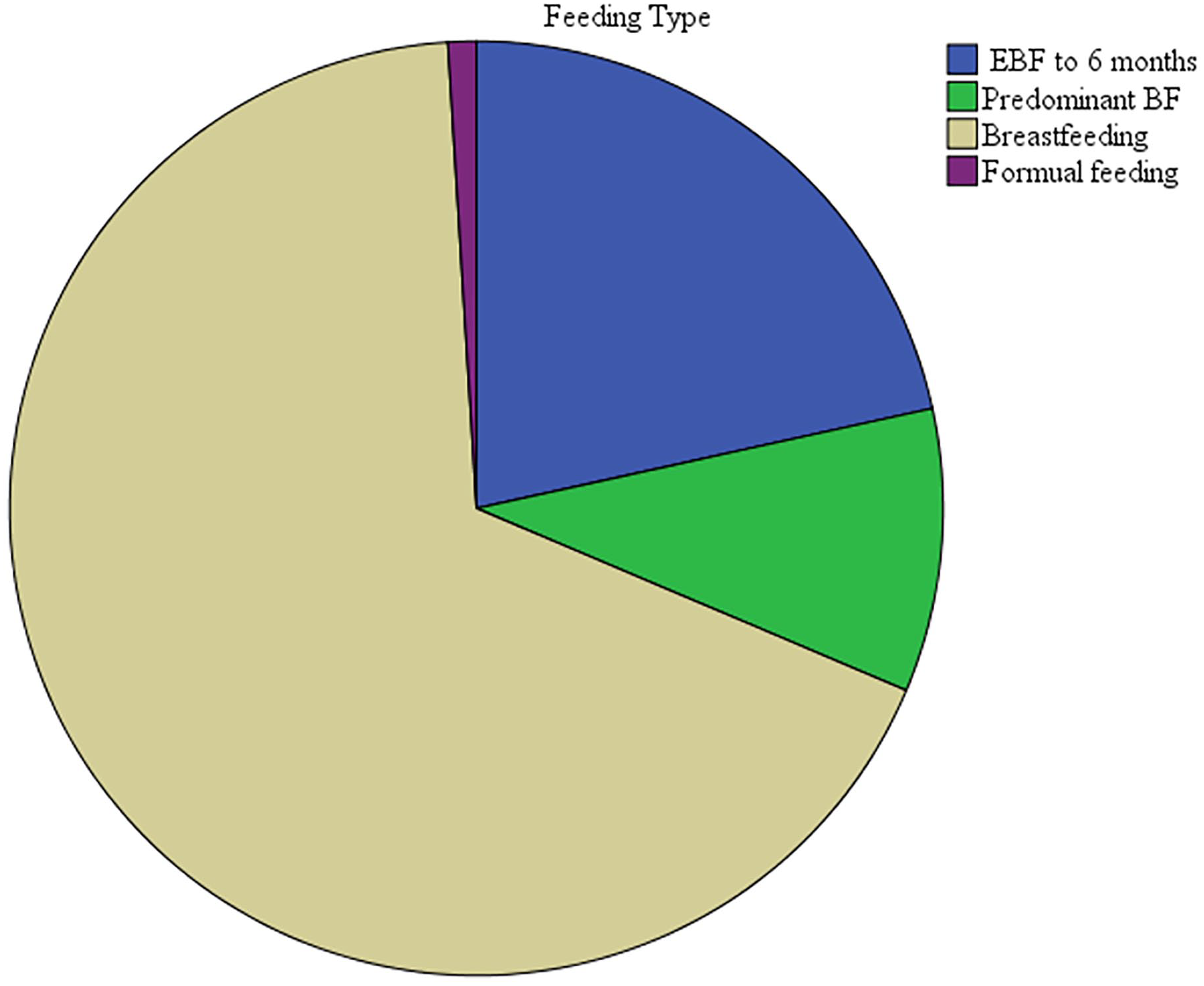
Feeding types of the sample.
Reasons for stopping breastfeeding.

The results of simple logistic regression models indicated that age, education, employment, and length of stay in US were not significant related to exclusive breastfeeding at six months. Household income was the only variable that was significantly related to exclusive breastfeeding. The odds of exclusive breastfeeding in mothers with incomes of $70 000 or more was 2.43 (95% CI 1.01-5.86; P = .04) compared to mothers with incomes less than $70 000. Maternal age was the only variable that was statistically significant when associated with breastfeeding duration. Results of this study indicated that older mothers were less likely to stop breastfeeding at twelve months (OR = 0.10; 95% CI 0.83-0.99, P = .04). Religion was significantly related to exclusive breastfeeding. Mothers who reported that their religion influenced their feeding choice were more likely to exclusive breastfeed than mothers who indicated religion did not influence their feeding choice (OR = 0.38; 95% CI 0.16-0.90; P = .02).
Discussion
Almost all participants breastfed their babies (n = 115, 99.1%). The percentages of mothers who began breastfeeding during the first hour in this study are higher than that of the national standards of 81.9%. 20 High breastfeeding initiation rates show that mothers want to breastfeed. Although almost all immigrant Muslim Arab mothers breastfed their babies in this study, exclusive breastfeeding to six months of the baby’s life was practiced by only 21.6% of mothers. Researchers in Arab countries reported similar exclusive breastfeeding rates. The pooled prevalence of exclusive breastfeeding in Middle Eastern countries was calculated as 20.5%.21,22 Rates varied between countries with the most reported rates were under 25%. 22 For example, the prevalence of exclusive breastfeeding for infants at six months was 8% in Kuwait, 23 11% in Lebanon, 24 31.4% in Tabuk, Saudi Arabia, 21 33% occurred in Jordan, 25 16.9% in Abu Dhabi, United Arab Emirate, 26 and 50% in Egypt. 27 The large discrepancy between breastfeeding practices in this population and international recommendations for breastfeeding demonstrates that increased attention should be given to the promotion of exclusive breastfeeding among Muslim Arab immigrants. 7 Given the protective benefits of exclusive breastfeeding, interventions should target practices that encourage and support exclusive breastfeeding among this immigrant group.
Of those that predominantly breastfed, supplementation was mostly from the practice of giving ritual fluids. Supplemental feedings are common in Arab cultures and are given to protect children from real or assumed health hazards. Supplemental feeding (eg, water, sugar water, salt solution, yogurt, gripe water, herbal tea, and black tea) is a common traditional practice among Arab cultures and interferes with exclusive breastfeeding.14,27,28 These practices can be improved by counseling and confidence building. Healthcare providers must provide breastfeeding education and support among these women. 7
In this study, many mothers reported mixed feeding. Researchers from Arab countries have reported mixed feeding as a common feeding practice.6,21,22,24,25 Supplementation with formula often starts around four months The most common reasons for mixed feeding were insufficient milk, return to work/school, the belief that mixed feeding is the ideal method of feeding, and various breastfeeding difficulties.21,22,29 Other studies reported difficulties in managing breastfeeding problems (eg, difficulty in positioning and latching, nipple soreness, pain, infection). Other reasons for mixed feeding were the beliefs that breast milk was not enough to satisfy or nourish their infants as evidenced by hunger or crying after the feeding.21,22,24,29 It is unclear from the present study if the reported mixed feedings were related to these problems. An understanding of the mothers’ beliefs towards mixed feeding will guide the development of effective breastfeeding education and promotion.
Mothers in this sample breastfed for a median duration of 11.86 months. Studies reported longer duration of breastfeeding in Arab countries.13,22,26 The key identified reasons for discontinuing breastfeeding were not enough breast milk and that the child was still hungry after breastfeeding. Perceived insufficient milk supply is the most common reason for women to stop breastfeeding.30,31 These results suggest that women’s perceptions of having a low milk supply might, in many cases, be related to their lack of information and understanding regarding the physiology of lactation. Increasing breastfeeding knowledge is a process that can be improved with increased scientific knowledge and support through input from healthcare providers. The explanation of “insufficient milk” could mask a range of underlying factors that undermine breastfeeding.
Other reasons reported for termination of breastfeeding were that the mother felt more comfortable giving the baby formula and did not have time to breastfeed. The perceived inconvenience of breastfeeding is a barrier to continued breastfeeding. 32 These reasons reflect immigrant Muslim Arab challenges and pressures related to balancing their breastfeeding commitment and household responsibilities. It is a traditional norm that Arab men should not involve themselves with infant feeding because it is believed to be a “woman’s job.” This has an impact on breastfeeding patterns. The importance of the involvement of fathers with breastfeeding has shown to be significantly associated with breastfeeding duration. 33 Issues of inconvenience may be addressed by encouraging the mother to use breast pumps, which allow the father to participate in infant feeding by using breast milk rather than formula.
Only a few women in the study noted that return to work/school was a barrier that prevented breastfeeding. This finding is similar to the findings of a research study conducted by Dagher et al 34 that indicated working mothers who returned to work were less likely to continue breastfeeding.
Healthcare providers should also be trained to understand the religious and cultural context of breastfeeding practices. Clear and open communication should be encouraged between the mother and healthcare providers to allow better understanding of their breastfeeding needs and practices. An example of religious practice that Muslim families practice related to breastfeeding is Tahneek, which is rubbing a small piece of softened date on the newborn’s palate shortly after birth and before the first feeding based on the practice of the Prophet Muhammad (Peace be Upon Him). This practice has been supported by current evidence-based practice as the first line therapy to treat hypoglycemia in late preterm and term babies in the first forty-eight hours after birth. 35
Sociodemographic characteristics including maternal age, income, employment, and education have been reported to influence exclusive breastfeeding practices. However, the results of this study indicated that income is the only variable associated with exclusive breastfeeding. Mothers with high income tend to exclusive breastfeed more than the mothers from low income. These results are congruent with those reported in developed countries.22,36 Religion was a predicted factor for exclusive breastfeeding practice in this sample. Al-Sahab et al 37 ; Dorri et al 38 ; and Jamil 39 stated that religion plays a significant role in predicting breastfeeding among Muslim women at four months.
Successful breastfeeding is dependent multiple factors related to the mother, and socioecological environment. In this study, mother’s age was significantly related to breastfeeding duration. This is in contrast to results reported in US which have shown that older maternal age is associated with longer duration of breastfeeding.40,41 This is congruent with the results of many Arab studies which suggested that breastfeeding is more common among younger mothers.42,43
Limitations
The generalizability of the study is limited by the small convenience sample that was drawn from a population of immigrant Muslim Arab women living in the Southwest region. The conclusions reached may be applicable only to immigrant Muslim Arab mothers sharing the participants’ personal characteristics, such as using similar kinds of health facilities or living in similar geographic areas. One important limitation of this study is recall bias due to the retrospective nature of the approach to data collection and the effect it may have on the results of the study. This might lead to over/under estimation of actual practices and inaccuracy about dates, particularly in the survey. However, an important strength of this study is using a cross-sectional approach, which is relatively cost effective as fewer resources are required and it provides a snapshot of variables at a moment in time.
Conclusions
This study contributes to the limited breastfeeding research in immigrant Muslim Arab women. Despite high rates of initiation and breastfeeding duration, exclusive breastfeeding practices of immigrant Muslim Arab mothers are lower than WHO recommendations. Findings from this research make a number of important contributions to the literature in identifying current breastfeeding practices of Muslim Arab women. It informs the need for the development of educational interventions to raise women’s awareness of the importance of exclusive breastfeeding for the first six months of their infants’ life, the advantages of breastfeeding for the mother and child, and potential hazards of formula feeding. Healthcare providers should help women gain confidence in their ability to produce enough milk and be advised on the physiology of breastfeeding to successfully continue breastfeeding.
This research has laid the foundation for describing and understanding breastfeeding practices of immigrant Arab Muslim immigrant women in the US. To have a better understanding of the immigrant Muslim Arab women sociocultural context of infant feeding, their common concerns, cultural beliefs and practices, and the way these factors work together to shape infant feeding practices, descriptive qualitative studies are needed. Descriptive qualitative research is needed to understand breastfeeding practices from the perspective of these women. Religious teachings are said to be valuable sources of information that help to promote breastfeeding in this group of women. The importance of having qualitative research to explore the significance of Quran teachings on breastfeeding is highlighted. Cultural practices and beliefs were not addressed in this study, and thus future researchers might look at these issues in greater depth. Future researchers may explore the diversity in breastfeeding practices among Muslim Arab women.
Supplemental Material
sj-docx-1-pdi-10.1177_11795565231200798 – Supplemental material for Breastfeeding Practices and Associated Factors among Immigrant Muslim Arab Women Living in a Metropolitan Area of the Southwest of United States
Supplemental material, sj-docx-1-pdi-10.1177_11795565231200798 for Breastfeeding Practices and Associated Factors among Immigrant Muslim Arab Women Living in a Metropolitan Area of the Southwest of United States by Wafa F Khasawneh, Azza H Ahmed, Megan E Petrov, Elizabeth Reifsnider and Pauline Komnenich in Clinical Medicine Insights: Pediatrics
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.