
Abstract
A 1 year and 7 months old girl presented to the medical genetic clinic as a referral from the pediatrics clinic. Upon examining the patient and assessing past medical history, an autosomal recessive disorder was suspected. The family underwent whole exome sequencing, which resulted in the diagnosis of Kaufman oculocerebrofacial syndrome (OMIM #244450) in the patient due to the fact that both parents were heterozygous carriers of a novel pathogenic variant in the gene UBE3B that lies on 12q24. It has been recommended for the family that preimplantation genetic testing should be considered for future pregnancies. In this case report, we present a novel variant of the gene and highlight the support of whole exome sequencing in the unveiling of genetic disorders.
Keywords
Introduction
Kaufman oculocerebrofacial syndrome was first reported by Kaufman et al 1 as a distinctive syndrome in 4 of 7 siblings of German ancestry. Over the next 2 decades, cases with the same clinical features appeared emphasising that this syndrome was in fact present in different regions of the globe.2 -4 The cases reported noted that both parents were unaffected, however, the children presented with growth delay, preauricular tags, upslanting eyes with different anomalies, and intellectual disability. In 2012, Basel-Vanagaite et al were the first to link the clinical features of Kaufman Oculocerebrofacial Syndrome with the gene UBE3B, which codes for ubiquitin-protein ligase E3B, after its observation in all patients. 5 The data analyzed UBE3B mutations in 4 patients from 3 unrelated families reported through literature, confirming that Kaufman Oculocerebrofacial Syndrome is an autosomal recessive disorder. All 3 UBE3B mutations found on chromosome 12q24 introduced premature termination codons and were expected to result in nonsense-mediated mRNA decay and/or protein truncation. 5 Herein, we report a case of a rare pathogenic UBE3B variant from 1 family.
Case Presentation
Pediatric clinic consultation
The patient was delivered at full term by spontaneous vaginal delivery following an apparently normal pregnancy with a birthweight of 2.8 kg. She was noted from the time of birth to have multiple dysmorphic features which instigated investigations and referral to the medical genetic clinic. Clinical features evident in the patient include growth deficiency evident from the antenatal period, upward slanting eyes, microcephaly, microphthalmus, and sclerocornea with severe visual impairment, bilateral ear canal stenosis with moderate hearing impairment, micrognathia, low-set ears, long shallow philtrum, narrow mouth, and over-riding toes. She has global developmental delay, hypotonia, and an abnormal EEG with seizure activity.
Medical genetics clinic consultation
An autosomal recessive disorder was suspected, as a result, whole exome sequencing (WES) was requested for the daughter as both parents were unaffected but had a consanguineous marriage (first cousins). The report found that the patient was homozygous for the pathogenic variant c.469C>T (p.Arg157*) in the UBE3B gene, which has not been reported previously in databases. This confirmed that the autosomal recessive disorder suspected is Kaufman Oculocerebrofacial Syndrome. The parents underwent WES to further screen for the inheritance of the pathogenic variant. The reports came back with a positive result that both parents were heterozygous (carriers) for the same pathogenic variant in the UBE3B gene found in their daughter.
Whole exome sequencing (WES) methodology and result interpretations
The clinical information provided as part of the WES request followed HPO nomenclature (Figure 1). Previous external genetic testing part of the newborn screening were negative, with a karyotype (46,XX).

Patient clinical information.
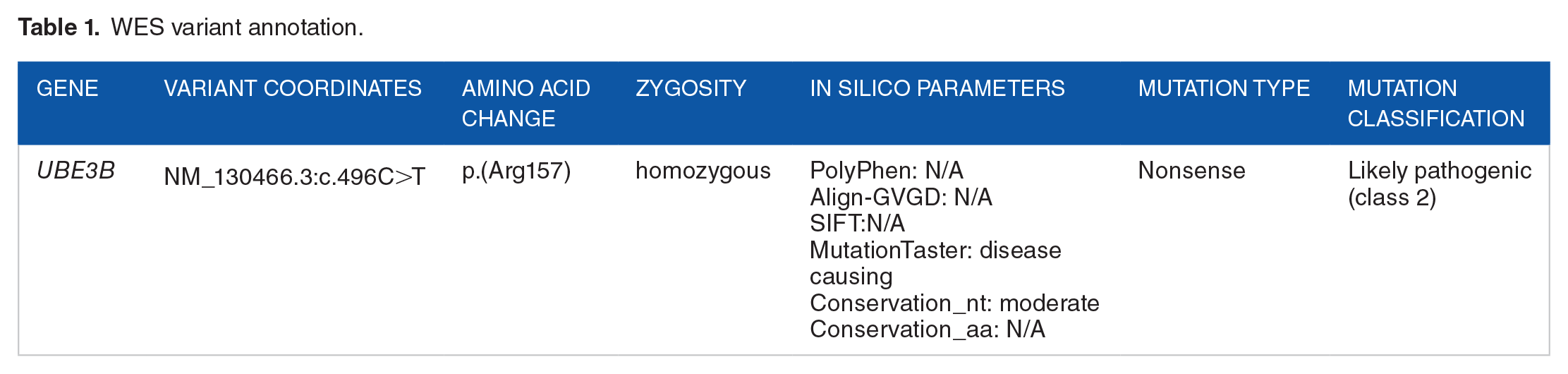
A double-stranded DNA baits against ~36.5 Mb of the human exome are used to enrich target regions from fragmented genomic DNA with the Twist Human Core Exome Plus kit. CentoXome® Solo including NGS-based CNV analysis targeted 98.74% nucleotides for this patient with at least 20× coverage depth. An in-house bioinformatics pipeline, including read alignment to GRCh37/hg19 genome assembly, variant calling, annotation, and comprehensive variant filtering is applied. The investigation for relevant variants is focused on coding exons and flanking patterns are considered, however, only variants in genes potentially related to the proband’s medical condition are reported. CNVs are detected with a sensitivity above 90% for all homozygous deletions and heterozygous deletions/duplications spanning at least 3 consecutive exons. The results found a premature stop codon on UBE3B variant c.469C>T p.(Arg157*; Table 1).
WES variant annotation.
Discussion
Kaufman Oculocerebrofacial Syndrome was first described in 1971, but it was not until 2012 that its genetic cause was discovered by the identification of biallelic mutations in the ubiquitin ligase E3B encoding gene UBE3B. 6 Kaufman Oculocerebrofacial Syndrome is most commonly diagnosed through genetic testing as there is not a consensus on the clinical diagnostic criteria, 7 and it is characterized by developmental delay, intellectual disability, microcephaly, hypotonia, structural eye anomalies, other organ malformations, and distinctive facial dysmorphic features. 8
Basel-Vanagaite et al linked these characterizations with the gene UBE3B, which is a found-on chromosome locus 12q24.11. This gene encodes the protein ubiquitin-protein ligase E3B which is highly expressed in the central nervous system, digestive tract, respiratory system, multiple cell lineages, and other soft tissues. 7 Using mouse models, the UBE3B mouse phenocopies reduced brain size, muscular strength, hearing impairment, and reduced cholesterol levels that is found in human patients. 6
Kaufman Oculocerebrofacial Syndrome is an underdiagnosed disorder in clinical practice due to its over lapping clinical presentations with blepharopgimosis-mental retardation syndromes, and rarity. 9 A case series and literature review identified 31 cases of Kaufman Oculocerebrofacial Syndrome in 2019, summarizing the clinical feature into 11 sections: Neonatal findings, growth, craniofacial feature, respiratory symptoms, cardiovascular findings, genitourinary findings, musculoskeletal findings, neurological findings, ectodermal findings, and laboratory findings. 10 Our patient was reported to have craniofacial features, respiratory symptoms, cardiovascular symptoms, gastric symptoms, as well as neurological findings. These findings were compared to other cases found in literature, where we found similar symptoms were reported in other cases. 11 As a result, physicians can use these lists to assess the clinical characteristics of Kaufman Oculocerebrofacial Syndrome.
Apart from our case in the Middle East and North Africa, ten known cases of Kaufman Oculocerebrofacial Syndrome were reported within the past 5 years. In Egypt, 9 cases were reported as Blepharophimosis-Ptosis-Intellectual Disability (BPID) Syndrome also known as Kaufman Oculocerebrofacial Syndrome, in 6 unrelated families. 12 Meanwhile in the United Arab Emirates, 1 case of a 9-year-old boy was noted as part of a retrospective analysis on neuro-genetic disorders patients, as well as mentioning that his sibling and cousin were affected. 13 Most cases discussed in the literature allude to the disease being more common in females,10,12 -14 but no studies confirm that gender has a significant correlation with the syndrome.
Due to the rarity of Kaufman Oculocerebrofacial Syndrome, there is no clinical guidelines for management. Treatment of clinical manifestations is advised upon diagnosis. Some clinical manifestations include epilepsy, feeding Issues, ophthalmologic involvement, hearing impairment, respiratory problems, cardiac anomalies, renal anomalies, skeletal, endocrine, and cleft palate. 7 Surveillance is recommended for all patient diagnosed with Kaufman Oculocerebrofacial Syndrome to assess for developmental delays, vision, and hearing. Furthermore, in our case, Preimplantation Genetic Testing (PGT) was recommended to the parents for future pregnancies.
Future directions of genetic testing the Middle East have been highlighted in Saudi Arabia after stating that due to the high rate of consanguinity, high birth rate, and burden of genetic diseases it pose a serious challenge to the healthcare providers to implement long term care. 15 Furthermore, accessing genetic services for preventative purposes is a problem for the region. Strategic plans proposed included increasing the general publics’ awareness about the consequences of consanguineous marriage, the burden of managing genetic diseases, and improving access to genetic prevention services. 15
Conclusion
To conclude, the use of next generation sequencing in clinical diagnosis will eventually lead to expanding the knowledge of Kaufman Oculocerebrofacial Syndrome. As such, this case report would like to draw awareness to the use of the WES in cases of unexpected clinical features from a young age to support the treatment and management of incurable diseases especially in the Middle East and Northern Africa region.