
Abstract
In pediatric patients, the antibiotic use is affected by parental beliefs and practices; especially in countries where it is possible to acquire them without prescription. This study aims to describe the knowledge, attitudes, and practices on antibiotic use among parents of children from urban and peri-urban health care centers in Lima. A cross-sectional study was performed at 1 urban and 2 peri-urban health care centers selected in Lima, Perú. Parents of children below the age of 3 years answered a knowledge-attitudes-practices-validated questionnaire about antibiotic use and were categorized as high, moderate, and low knowledge regarding antibiotics. We analyzed potential determinants for low knowledge and having medicated their children with unprescribed antibiotics using bivariate and multivariate analyses. A total of 224 parents were enrolled, and 8% were categorized as low knowledge. Half of the parents could not recognize that antibiotics cannot cure viral infections, 59.4% disagreed with “antibiotics speed up recovery from a cold,” and 53.2% stored antibiotics at home. Remarkably 23.5% of parents reported having medicated their children with antibiotics without prescription, which was associated with belonging to the peri-urban health care center, use of antibiotics by their children in the last 12 months, and having purchased antibiotics without physicians’ prescription. An alarming overuse of antibiotics without prescription was described among children below the age of 3 years. Educational interventions, addressing parental attitudes and practices, and health policies should be developed to limit inappropriate antibiotic use especially in peri-urban communities.
Background
The control of infectious diseases is nowadays threatened by the increase in antibiotic-resistant organisms. Resistant pathogens have affected mortality, treatments costs, and the spread of infectious diseases. 1 In the United States, these organisms are responsible of 2 million infections and 23 000 deaths yearly, with an economic impact of an additional US$35 million in health expenditures. 2 In Latin America, the information about antibiotic resistance is obtained mainly from the epidemiological analysis of nosocomial infections, highlighting the emergence of broad spectrum resistance to β-lactamases. 3 Peru has shown to have significant high levels of antibiotic resistance, being the country with the highest percentage of methicillin-resistant Staphylococcus aureus (MRSA) in South America and the second with extended spectrum β-lactamases Escherichia coli. 4
The appearance of these organisms is related to the antibiotic use primarily in hospitals, the inadequate selection of them, the wrong dosage, and the low adherence of patients to treatment regimens, which culminates being a perfect environment for the development of antibiotic resistance. 3 In developing countries, the unnecessary use of antibiotics is very common due to the high prevalence of infectious diseases and the possibility of acquiring antibiotics without prescription, which makes self-medication possible. 5
The management of pediatric diseases depends on the parental perception and practices on medication; parents have limited knowledge about the use of antibiotics, a suggested factor to explain the misuse of these in children.6,7 It has been proven that 77% of children who received antibiotics for upper respiratory tract infections have a viral cause and the use of antibiotics does not change the duration and severity of symptoms; however, practitioners have recognized parents’ expectations as a factor influencing antibiotic prescription.8,9
There are few studies that address education of parents about the correct use of antibiotics despite the importance of this factor in preventing the development of antibiotic resistance in countries where antibiotics can be purchased without a prescription. Besides the possible differences between the antibiotic use in urban and peri-urban locations remains poorly understood. Therefore, the aim of this study is to describe the knowledge, attitudes, and practices about antibiotic use among parents of children below the age of 3 years from urban and peri-urban health care centers in Lima, Peru and to analyze potential determinants of having medicated their children with antibiotics without prescription.
Materials and Methods
Study design, setting, and population
We conducted a cross-sectional study that involved parents of children below the age of 3 years who attended 2 peri-urban primary health care centers and 1 urban clinic. The primary public health care centers selected for the study are located in the districts of San Juan de Lurigancho and Independencia, both in peri-urban communities. San Juan de Lurigancho represents 12% of the population of Lima (1 069 703 inhabitants), and it is estimated that 22% of its population live in poverty. Independencia is a smaller district with 207 647 inhabitants; however, 16.9% of its population is considered to be in poverty. The urban private clinic selected for the study is located in Miraflores a smaller district with 85 065 inhabitants and less than 1% of poverty. 10 The principal investigators invited parents of children below the age of 3 years to participate during the waiting rooms for the medical and nurse appointments and the vaccination area from the health care centers. We included parents of children below the age of 3 years, who were older than 18 years, and who were able to read and understand the questionnaire. We excluded participants who filled less than 50% of the questionnaire.
Study procedures
The main outcomes of this project were to describe the knowledge, attitudes, and practices about the use of antibiotics and to correlate low knowledge and self-medication with demographic characteristics. The study used a multiple-choice questionnaire to assess knowledge and attitudes, previously validated by Alili-Idrizi et al 11 For the practices toward antibiotic usage, we used a previously validated questionnaire by Yu et al. 12 Participants answered a 35-item survey of multiple-choice questions. The survey consisted of 3 parts: the first contains 9 claims about knowledge covering aspects including the role of antibiotics, the dangers of using them (allergic reaction), and the effectiveness of antibiotics. The participants could answer “Yes,” “No,” or “I do not know.” The second part contained 10 questions about attitudes regarding the use of antibiotics. Participants could respond “Agree,” “Disagree,” or “I’m not sure.” One question (question 3) was changed from “It would be good to be able to buy antibiotics directly in pharmacies” to “I think it is good to be able to buy antibiotics directly in pharmacies” as in Peru it is possible to buy antibiotics in drug stores without a prescription. The question “Antibiotics should be administered in all cases when a child has a fever” was extracted from the study by Yu, M. et al in 2014 and added to the survey. The third part consists of 5 questions about the practices regarding the use of antibiotics. Participants could respond “Agree” or “Disagree.” In addition, we obtained demographic information on age, sex, education, number of children, age of older children, and previous use of antibiotics by parents and their children.
Data management and analysis
Data were entered in an Access database developed for the study. To describe the main outcomes of the project, we used descriptive measures of central tendency such as mean and standard deviation for continuous variables and for categorical variables percentages and descriptive measures using STATA 11. Each question was described separately and the statistical difference between parents from the peri-urban and urban health care centers for each question was analyzed through chi-squared test.
We categorized knowledge as low, moderate, and high using the number of questions correctly answered as in the study of Alili-Idrizi et al 11 ; being 1 to 3 correct questions a low knowledge, 4 to 6 moderate, and 7 or more high knowledge. We categorized adequate and inadequate attitudes using the median as cutoff. We used bivariate models with logistic regression to study the association of knowledge and having self-medicated their children with antibiotics with the potential individual predisposing factors separately. Variables were included in the multivariate analysis to determine the factors that are independently associated with each dependent variable. The results were reported as odds ratios (ORs) with a 95% confidence interval.
Ethical considerations
The protocol was approved by the Institutional Review Boards of our institutions. The researchers explained the informed consent procedure and that this survey was not from the health system and that their willingness to participate or not would not affect their care. Informed consent was obtained from each participant.
Results
Sociodemographic characteristics
We invited 252 parents to participate, 230 accepted and signed the informed consent, and 6 of them were excluded because they filled less than 50% of the survey. The study analyzed a total of 224 parents: 111 (49.5%) from the urban health care center and 113 (50.5%) from the peri-urban health care centers. Parents from both type of centers had different sociodemographic backgrounds (Table 1). In general, 83.5% of participants were female, the median age was 32 years (interquartile range [IQR]: 27-37 years), and most of the parents enrolled had superior education (55.9%). More than half of their children (61.2%) had received antibiotics in the last 12 months and 10.7% had never received antibiotics.
Sociodemographic characteristics of the participants.

Abbreviations: IQR, interquartile range.
Knowledge about antibiotics
The answers to the 9 questions related to knowledge about antibiotics are presented in Table 2. Most of the parents were categorized as high knowledge (48.2%), 43.8% as moderate knowledge, and 8.0% as low knowledge. In the peri-urban health care centers, 14.2% of the parents were categorized as having low knowledge versus 1.8% in parents from the urban health care center. Half of the parents were not able to recognize that antibiotics cannot cure viral infections and 22.3% did not disagree with the statement “Antibiotics must be taken once a child has a cold.” Almost every statement showed a significant difference between answers from parents from the peri-urban and urban health care centers (P < .05), except the statement “children can be allergic to antibiotics” and “penicillin is an antibiotic.”
Correct answers about the knowledge, attitudes, and practices about antibiotics.

Attitudes toward antibiotics
The answers to the 11 questions related to attitudes toward antibiotics are presented in Table 2. The median score was 5 (IQR: 5-7). Most parents (65.2%) were categorized as having inadequate attitudes toward antibiotics. More than half (59.4%) of parents disagreed with “antibiotics speed up recovery from a cold” and almost one-third of parents (32.1%) did not disagree with “It is good to be able to buy antibiotics over the counter at the pharmacy.”
Practices toward antibiotics
The answers to the questions related to practices of parents among the correct use of antibiotics are presented in Table 2. More than half of parents reported having purchased antibiotics without a prescription and having stored antibiotics at home. We found that 23.5% of parents had medicated their children with antibiotics without prescription, which was recognized by 38.2% of parents from the peri-urban health care centers and 9.1% of parents from the urban health care center.
Bivariate and multivariate analyses of determinants of knowledge about antibiotic use
In the bivariate analysis, we found that parents from the peri-urban health care centers, with inadequate attitudes toward antibiotics, with more than 3 children, who had below superior education and whose eldest child had more than 5 years were more likely to have low knowledge. However, on the multivariate analysis, none of them was associated with low knowledge about antibiotic use (Table 3).
Bivariate and multivariate analyses of determinants of low knowledge about antibiotic use in parents of children below the age of 3 years from Lima, Peru.

Abbreviations: CI, confidence interval; OR, odds ratio.
Bivariate and multivariate analyses of determinants of having self-medicated their children without prescription
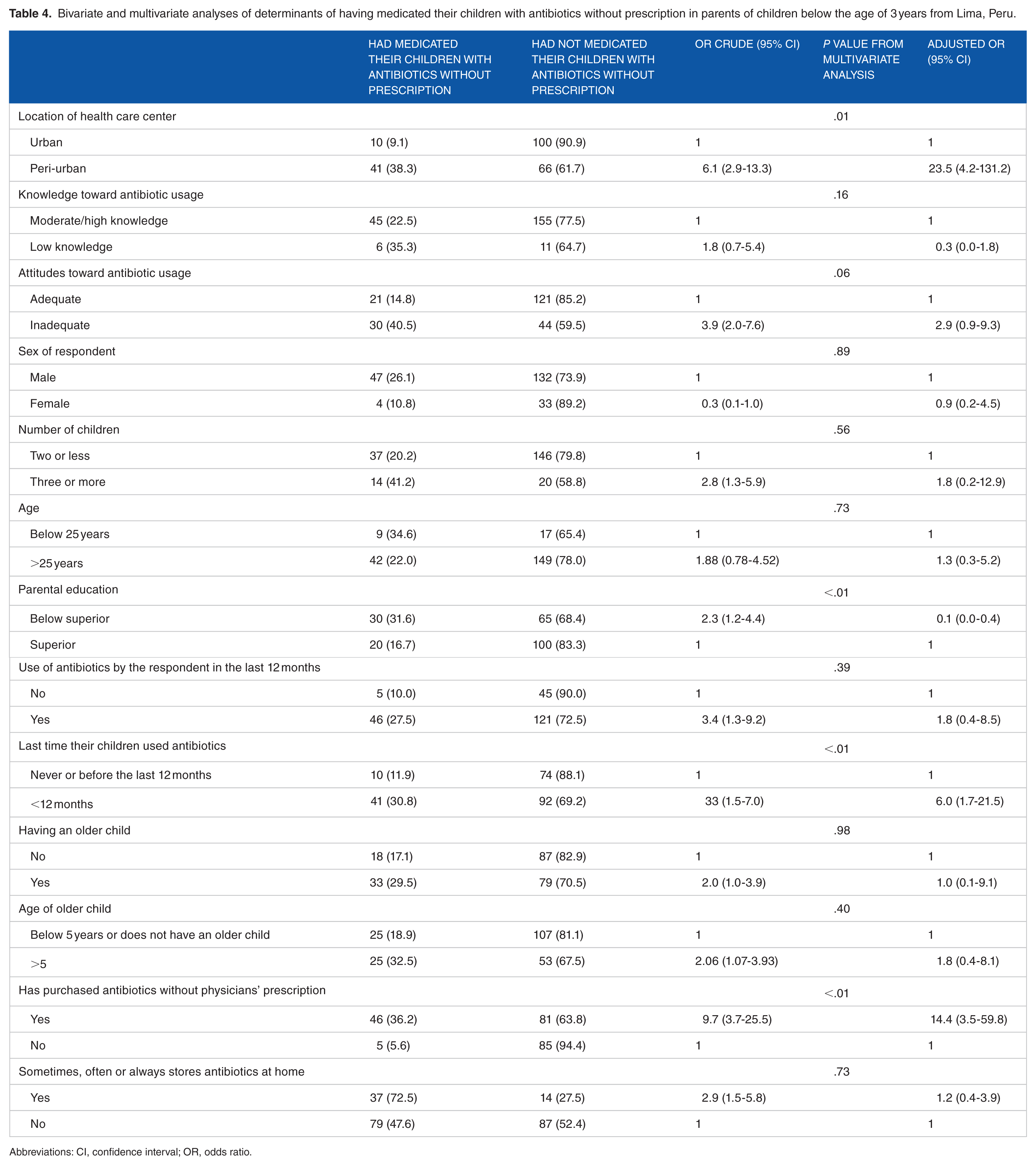
Factors associated significantly with having medicated their children with antibiotics without prescription after bivariate and multivariate analyses were belonging to the peri-urban health care center, use of antibiotics by their children in the last 12 months, and having purchased antibiotics without physicians’ prescription (Table 4). Interestingly after multivariate analysis, parents who had superior education were more likely to self-medicated their children with antibiotics without prescription. Inadequate attitudes toward antibiotics were associated with this practice in the bivariate analysis, but this association was lost in the multivariate analysis (P = .06).
Bivariate and multivariate analyses of determinants of having medicated their children with antibiotics without prescription in parents of children below the age of 3 years from Lima, Peru.
Abbreviations: CI, confidence interval; OR, odds ratio.
Discussion
This study revealed important findings about inadequate knowledge, attitudes, and practices toward antibiotics. We found that 23.5% of parents reported having medicated their children with antibiotics without prescription and 8% of parents from our population showed a low knowledge regarding antibiotic usage.
Our population was composed of younger parents with a lower educational level and scored a higher knowledge of antibiotics compared with previous studies.11-14 Studies from America, Asia, and Europe report that between 22% and 70% of parents have misconceptions about the right use and efficacy of antibiotics. 15 In our study, half of the respondents (50.2%) answered incorrectly the statement that antibiotics can cure viral infections, which is similar than the results from a study in Lithuania where 47.7% incorrectly identified antibiotics as being effective either against viral or mixed infections and lower than the results from a study in India where 72% of parents could not recognize that antibiotics are used to treat only bacterial infections.13,14 Among attitudes more than half of respondents from the peri-urban health care center responded incorrectly to the statements “It is appropriate to use antibiotics when my child has a sore throat because otherwise he or she might catch something more serious” and “antibiotics speed up the recovery from a cold.” Moreover, almost half of the participants (47.6%) did not disagree on the statement that “antibiotics should be use every time a child has fever.” Compared with a study done in Macedonia that used the same survey, we found higher rates of correct answers regarding attitudes, 11 and comparing the statement “antibiotics should be administered in all cases once a child has fever” with the results from a study that enrolled parents in rural China, the percentage of respondents from urban settings was comparable in both studies (74.8% in ours and 72% in their study) but not in the peri-urban settings where 66% of their population responded correctly and only 30% of ours. 12 Even though the association between attitudes and the use of unprescribed antibiotics was lost after multivariate analysis, it trended toward significance (P = .06). Addressing attitudes might be a way to limit the incorrect use of antibiotics in our population.
In our study, the percentage of children who had previously received antibiotics was 89.3%, which is similar to the data from other study in different districts in Lima, but lower than percentages in rural areas of Peru such as Loreto and other low- and middle-income countries.16,17 Regarding practices, we found that more than half of participants (58.4%) had purchased antibiotics without prescription and 58.3% reported that had stored antibiotics at home.
Almost 1 out of 4 parents (23.5%) reported having medicated their children with antibiotics without prescription. Our results are comparable with other local studies such as 1 systematic review about antibiotic use that reported a frequency of nonprescription use of antimicrobials among general population in Perú of 25% and 1 study done in Loreto where parents reported that 71% of antibiotics received by their children were obtained from health professionals.18,19 However we found a higher percentage of self-medication compared with a study that enrolled adults who bought antibiotics for children in private pharmacies in peri-urban areas of Lima, where a prevalence of 13% of purchase of antibiotics without a prescription was reported in 2016. 17 The percentage of self-medication found in this study was higher compared with studies in Athens and Brasil but lower compared with a study in rural China.12,20,21
Factors associated with self-medication were belonging to the peri-urban health care center, use of antibiotics by their children in the last 12 months, and having purchased antibiotics without physicians’ prescription. Interestingly, parents with an education below superior were less likely to self-medicate their children after multivariate analysis, which might be because parents with lower education tend to have a lower economic status and therefore depend on the “Seguro Integral de Salud”, which subsidizes the provision of services to the population living in conditions of poverty and extreme poverty in Peru, to obtain medications for their children. 22 The relationship of peri-urban locations and high antibiotic self-medication has been previously described and has been associated mainly with economic reasons. 23 The fact that the peri-urban health care centers belonged to the public health system could be associated with this finding, as in Peru health services are recognized to have a pro-rich distribution. 24 Besides the population who attend the public health system have described low quality of attention and low accessibility and both money and time have been recognized by parents as reasons to self-medicate their children in other settings.12,22,25
Developing countries have higher levels of antimicrobial resistance and less resources to develop strategies to address this topic compared with developed countries. 26 Peru has shown the largest relative increase of antibiotic usage in South America, 27 and even though physicians are responsible for most antibiotics in the pediatric population, the misuse of antibiotics is common for pathologies such as common cold and diarrhea, where antibiotics are mostly not required. 28
Lima is facing alarming percentages of antibiotic resistance in multiple pathogenic and nonpathogenic bacteria, 50% of S aureus from blood cultures are methicillin resistant, 76.8% of E coli and 75.1% of Klebsiella are producers of extended spectrum β-lactamases, 59% of Pseudomonas aeruginosa isolates are multidrug resistant, 26 and commensal stains of E coli have shown high resistance to quinolones. 29
Despite the existence of laws that limit the acquisition of antibiotics without prescription, this practice is still common in our population. One study done in Chile showed that even though regulatory measures against the use of unprescribed antibiotics had an initial positive impact, there was no reinforcement in the time and there was no further control to this laws. 30
Strengths and limitations of the study
The results of this study should be interpreted in light of its limitations. First, it was composed of self-reported information and recall and omission bias may have influenced results, especially by parents from the urban health care center as they showed a higher educational status in this study and they might be not reporting their self-medication real practices. Besides, parental intentional or nonintentional misunderstanding of questions may also have a role in the findings, and the sample of this survey included only parents who attended health care services. This study enrolled only parents who sought care at health care centers and who could be able to read the informed consent and questionnaire, which limits the generalizability of the results, and the patterns of antibiotic knowledge and usage might be different in parents who do not attend any health care service. Besides the districts selected do not reflect the entire population of Lima as we selected 2 of the districts with highest rates of poverty and the district with the lowest rate of poverty in Lima.
Conclusions and recommendations
This study is relevant as it highlights an alarming overuse of antibiotics without prescription by parents of children below the age of 3 years, especially in peri-urban areas from Lima, Peru. Clinicians should encourage parents not to use antibiotics without prescription in their children and warn them about potential side-effects and the emergence of antibiotic resistance. It is indispensable to develop health policies that can limit the acquisition of antibiotics without prescription in our setting. Health education materials should be developed based on the findings from this study to address this important topic.
Footnotes
Acknowledgements
The research team would like to thank all participants who agreed to complete the survey. Furthermore, we would like to thank “Puesto de Salud Daniel Alcides Carrion,” “Centro de Salud Ermitaño alto,” and “Clinica Delgado” for their help and for allowing us perform this study in their settings.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interest:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
JLP designed the study contributed to collection, analysis and interpretation of data and wrote the initial draft of the manuscript. RN and MR contributed to analysis and interpretation of data, and assisted in the preparation of the manuscript. TJO supervised the conception and design of the work and contributed with the interpretation and critical revision of the article. All other authors have contributed to data collection and interpretation, and critically reviewed the manuscript. All authors approved the final version of the manuscript and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.