
Abstract
Objective:
New parents need education about infant sleep but is not universally available especially not in regional and rural areas. We delivered sleep education both face-to-face and online to test sleep knowledge acquisition for parents wherever they reside. Best practice delivery of accessible sleep health information for new families needs to be investigated more carefully in order for specialist services to be universally available.
Methods:
Pre- and post-information session questionnaires (n = 32) assessed levels of knowledge acquisition and comparisons tested differences between face-to-face seminars compared with an online webinar.
Results:
Sleep knowledge across participants was low (69% scoring < 50%). Sleep knowledge significantly increased for both the webinar delivery group (P = .002) and face-to-face delivery group (P = .001). No significant differences in knowledge acquisition were found between face-to-face vs online delivery (P = .170), suggesting both modes of delivery were sufficient to improve parental sleep knowledge.
Conclusions:
Parental sleep knowledge, while low, increased with education. Online delivery was similar to face-to-face delivery suggesting ease of access for rural and remote communities needing specialist sleep information.
Implications for public health:
Information delivered online is effective and offers a health delivery solution to regional and remote parents unable to access sleep services and rendering sleep service accessibility more equitable.
Introduction
Sleep health is the foundation of all areas of mental and physical health, yet 40% of families report sleep disturbance in their new child. 1 Dissemination of sleep education and information are imperative if we are to ensure optimal health. Best practice for information delivery and acquisition needs to be available for all families irrespective of where they live and what services are physically available.
Background
Among the most common concerns raised by caregivers are those where parents experience difficulties managing their children’s sleep and settling behaviours at the beginning of the night and overnight. 2 Some young children need parental assistance to re-settle, often up to 5 times per night. These sleep problems, when left unresolved, can result in significant and serious consequences for the child, including sleep problems in later childhood, 3 increased behaviour problems, learning difficulties, 4 and elevated risk of injury. 5 In addition, subsequent parental sleep disturbance can cause parental postnatal depression, 6 marital conflict, 7 performance and well-being problems, 8 and even child abuse. 7 Importantly, sleep problems costs the health care system up to US $1.5 billion per year. 9
Awareness of what is good sleep health and information to prevent or manage sleep problems is low in the community 10 and as a first point of call, parents seek assistance for sleep disturbance from their general practitioner (GP) or more commonly their community nurse. However, neither primary health professionals in Australia nor parents receive sufficient, systematic training or information in sleep health. 11 As a result, primary health care professionals may be ill-equipped to deliver evidence-based sleep education information to parents. Consequently, management techniques offered to families or accessed by families are very indiscriminate, non-systematic, and inconsistent. New parents deserve to be provided with the latest evidence and with information that they deem important to be empowered with knowledge. 12 Delivering sleep education to parents as a first point of call may be a primary solution.
In previous studies, face-to-face sleep education has increased knowledge in school-aged children13,14 and parents of school-aged children, 15 but literature for parents of young children is sparse.
Providing formal information to parents on childhood sleep behaviours increases their sleep knowledge and enables them to better manage these difficulties. 16 This has been shown in the general health literature when the dissemination of generalisable health information is encompassed within the stepped care model, 17 where information and preventive treatment delivered at a primary health care level (at the first tier of the model) can provide a degree of assistance to ameliorate health problems, avoiding the need for more specialised services and significantly reduce costs. The stepped care model has been used to deliver preventive sleep information to adult insomniacs 18 to avoid ongoing problems, so it may be that sleep information can be similarly preventive for infant sleep behaviours despite the complexities associated with early parenthood and the parent-child relationship. 6 Previous investigations of what information parents want have confirmed parental desires for preventive sleep education. 12
Knowledge delivery can occur either online or face-to-face. For example, delivery of health educational information on smoking 19 and AIDS/HIV 20 through face-to-face seminars significantly increased knowledge. Similarly, formal face-to-face sleep education in school-aged children 14 and university students 21 has been shown to increase knowledge acquisition.
Although face-to-face delivery is effective, it is restricted to those who can attend specialty services. Families residing in rural and remote locations or where services are not available are at a disadvantage. Therefore, the first step is assessing the value of technological advances for dissemination of sleep knowledge. Online delivery of sleep education would seem a plausible strategy for improving parental understanding of sleep patterns and their remedies especially if the delivery is an online model closely resembling that of the face-to-face model, such as an interactive webinar. The delivery of childhood sleep information using an online delivery platform (eg, webinar) has the capability to reach a wider audience than face-to-face delivery and could potentially provide a greater level of support to parents experiencing childhood sleep management problems, particularly those in rural and remote regions. 3
While health information delivery face-to-face and online have been found to be comparable for physical therapy, 22 how effective webinar delivery could be for the delivery of sleep education to new families is not known. Furthermore, to the authors’ knowledge, to date, there has been no systematic comparison of knowledge acquisition of sleep education through webinar vs face-to-face delivery.
The aim of this study was to determine whether knowledge acquisition is equivalent across delivery modes by comparing the formal acquisition of sleep knowledge between participants attending a face-to-face seminar and participants viewing an online webinar of childhood sleep information. Specifically, it was hypothesised that parent sleep knowledge acquisition would increase both through webinar information delivery and face-to-face delivery and, furthermore, knowledge acquisition will not differ between face-to-face seminar delivery and webinar delivery.
Method
Participants
Participants were recruited via convenience sampling for both sites. Site 1 (face-to-face delivery) was a regional centre in South Australia of approximately 4000 inhabitants where parents of children under 4 years of age were invited to attend a sleep education information session. Site 2 was an early childhood and parenting community centre 35 km south of Adelaide, South Australia. Sessions were advertised through community health care and Child Youth Health nurses’ networks and centres, parenting groups, radio, and through SA government networks. For both sites, the duration of the one sleep information session was 60 minutes with an additional 30 minutes for questions with the presenter, who is an experienced sleep clinician and paediatric sleep researcher (S.B.). Parents completed pre- and post-questionnaires which were collected on-site by the presenter (Site 1) or research assistant (Site 2). All Site 1 participants received face-to-face training and all Site 2 participants attended the webinar. Because the webinar was not recorded, and in an attempt to control as many variables as possible within this pilot study, both the face-to-face group and the webinar group had equal opportunity to gain knowledge about sleep within the same time frame (90 minutes) with only the medium of delivery and venue being different between the groups.
Any parent could attend, regardless of whether or not their child presented with sleep disturbance. Participants were predominantly (97%) women, with only 1 male participant (in the face-to-face group). In all, 8 parents failed to complete both pre- and post-questionnaires and 1 parent failed to complete a consent form. As the study measured knowledge acquisition generally rather than specific to that of parents, data from child care workers who attended the seminars (n = 3) were retained for analysis. Participant age was divided into 3 categories (25-30, 31-36, and ⩾37 years) based on percentiles. Participant’s socio-economic status (SES) was measured using the SEIFA Index of Relative Socio-economic Advantage and Disadvantage. 23 The SES decile, based on participants’ postcode, was collapsed into quintiles (eg, first and second decile collapsed to form first quintile, third and fourth deciles collapsed to form second quintile, where the first quintile represents the highest SES and the fifth quintile the lowest SES).
Ethics and informed consent
Ethics approval was obtained from Central Queensland University Ethics Committee (Approval# H15/04-070). Attendees were provided with a consent form detailing study purpose and confidentiality at the commencement of the sleep education information sessions. Participants provided informed consent by completion of the consent forms and research questionnaires.
Design
Measures
Parent Sleep Knowledge Inventory
Childhood sleep knowledge was measured pre- and post-information seminar using an adaptation of the Parent Sleep Knowledge Inventory (PSKI). 24 Questions from the original questionnaire that were relevant to children <4 years of age were extracted from the PSKI. Some questions were changed to increase ease of understanding (eg, PSKI Item 15 ‘One-year-olds sleep approximately 13-16hrs within a 24hr period’ changed to ‘One-year-olds sleep approximately 13-16hrs across the whole 24hr day and night period’). The final adapted questionnaire consisted of 26 items, including demographic questions (6 items) and 20 statements about childhood sleep behaviours where participants used a 4-point Likert scale, ranging from 0 (not at all true) to 2 (very true) or 3 (don’t know), to respond to each statement. To increase sensitivity of detecting change in knowledge, responses were recoded to align with correct answers (ie, most correct answer = 2, somewhat correct answer = 1) or definitely NOT correct (incorrect/don’t know answer = 0). ‘Pre-Scores’ and ‘Post-Scores’ were calculated for each participant by summing the score of each question, respectively. A ‘Score Difference’ was calculated by subtracting the Pre-Score from the Post-Score for each participant, where a higher Score Difference represented higher knowledge acquisition.
In addition, the post-webinar questionnaire included statements on the importance of sleep education and the value of online delivery, eg, ‘Delivering sleep education through online technology is better than no sleep education at all’, with a 4-point Likert scale ranging from 0 (not at all true) to 2 (very true), or Don’t know, reported as 3, for each statement. A final open-ended question allowed participants to ask for any further information on children’s sleep. Answers were independently thematically analysed.
Procedure
Following consent form completion, the sessions were presented and included information about child sleep patterns, age-appropriate sleep duration recommendations, sleep hygiene, and sleep behaviour modification methods. Table 1 presents the specific contents of the sleep education sessions in chronological order. All the information contained within the sessions was based on the latest information about sleep health in young children extracted from various evidence-based resources such as the American Academy of Medicine (https://aasm.org/) and the Australasian Sleep Association (https://www.sleep.org.au/). The same PowerPoint presentation was delivered to both the face-to-face parents and the webinar group parents.
Contents of sleep education programmes.

Information presented to parents about the development of problematic behavioural sleep associations (which are common in the age groups targeted for this study) was based on behaviour theory’s principle of extinction. 25 Extinction-based sleep interventions are those that `extinguish’ a behaviour by ignoring it or replacing it. In child sleep problems, the parent’s attention for re-settling is considered the reinforcer of protesting behaviour at night-time, so by ignoring or replacing the behaviour, it will decrease or go away. Explanations about these learned behaviours and how to improve and/or avoid them were discussed during the sleep education sessions. Following seminar completion, participants completed the post-questionnaire, which was collected on-site by the presenter (Site 1) or research assistant (Site 2).
Results
Demographics
In total, 32 participants attended the sessions. Participant age did not differ significantly between the face-to-face parents (n = 14, RangeAge 25-57 years, M = 34.39, SD = 7.83) and the webinar group parents (n = 18, RangeAge 28-46 years, M = 34.39, SD = 5.59), χ2(2, N = 32) = 0.42, P = .812. Over half of the participants (59.4%) were in the lowest quintile of SES 23 based on postcode, and although there was no significant difference in SES between groups, χ2(4, N = 32) = 8.62, P = .071, this trend may reflect the fact that all participants from Site 1 (face-to-face delivery) were all of medium to low SES. Most of the participants (90%) had at least 1 child under 3 years of age. Participants in the webinar group were significantly more likely to have a child under 12 months of age (n = 18, RangeAge: 4 months to 6 years, M = 1.89, SD = 1.65) compared with those in the face-to-face group (n = 11, RangeAge: 11 months to 2 years, M = 1.56, SD = 0.35), χ2(3, N = 29) = 10.65, P = .014. Participants in the face-to-face group (50%) were more likely to have more than 1 child compared with the webinar group (22%); however, the participants’ number of children did not significantly differ between the groups χ2(4, N = 32) = 7.314, P = .120.
Baseline sleep knowledge
Prior sleep knowledge among participants was low, with 69% of participants (22/32) scoring below 50% on the Pre-Score questionnaire (RangePreScore: 15%-65% correct, M = 41.3%, SD = 14.7%). Prior sleep knowledge was higher in the face-to-face group, with 51.1% scoring over 50% in the Pre-Score questionnaire compared with only 11.1% in the webinar group. The percentage of Pre-Score questions that were correct significantly differed between the groups, χ2(3, N = 32) = 7.777, P = .020. Participant demographics and sleep questions scores are presented in Table 1.
Changes in sleep knowledge
A paired-samples t test with an α level of .05 was used to investigate the effects of sleep information delivery method on knowledge acquisition. Sleep knowledge was measured pre- and post-information session and a Score Difference (Post-Score minus Pre-Score) measured change in knowledge scores, with higher scores indicating higher knowledge acquisition. Shapiro-Wilk statistics indicated that the assumption of normality was supported for all measures (P > .05).
Results showed an increase in sleep knowledge acquisition between the Pre-Scores (M = 15.06, SD = 4.80) and Post-Scores (M = 18.55, SD = 4.36) for the webinar delivery group, which was statistically significant t(17) = 3.71, P = .002, 2-tailed, d = 0.88, with a large effect size. Results also showed an increase in sleep knowledge acquisition between the Pre-Scores (M = 18.43, SD = 6.74) and Post-Scores (M = 24.21, SD = 3.87) for the face-to-face delivery group, which was also statistically significant, t(13) = 4.16, P = .001, 2-tailed, d = 1.11, with a large effect size (Figure 1).
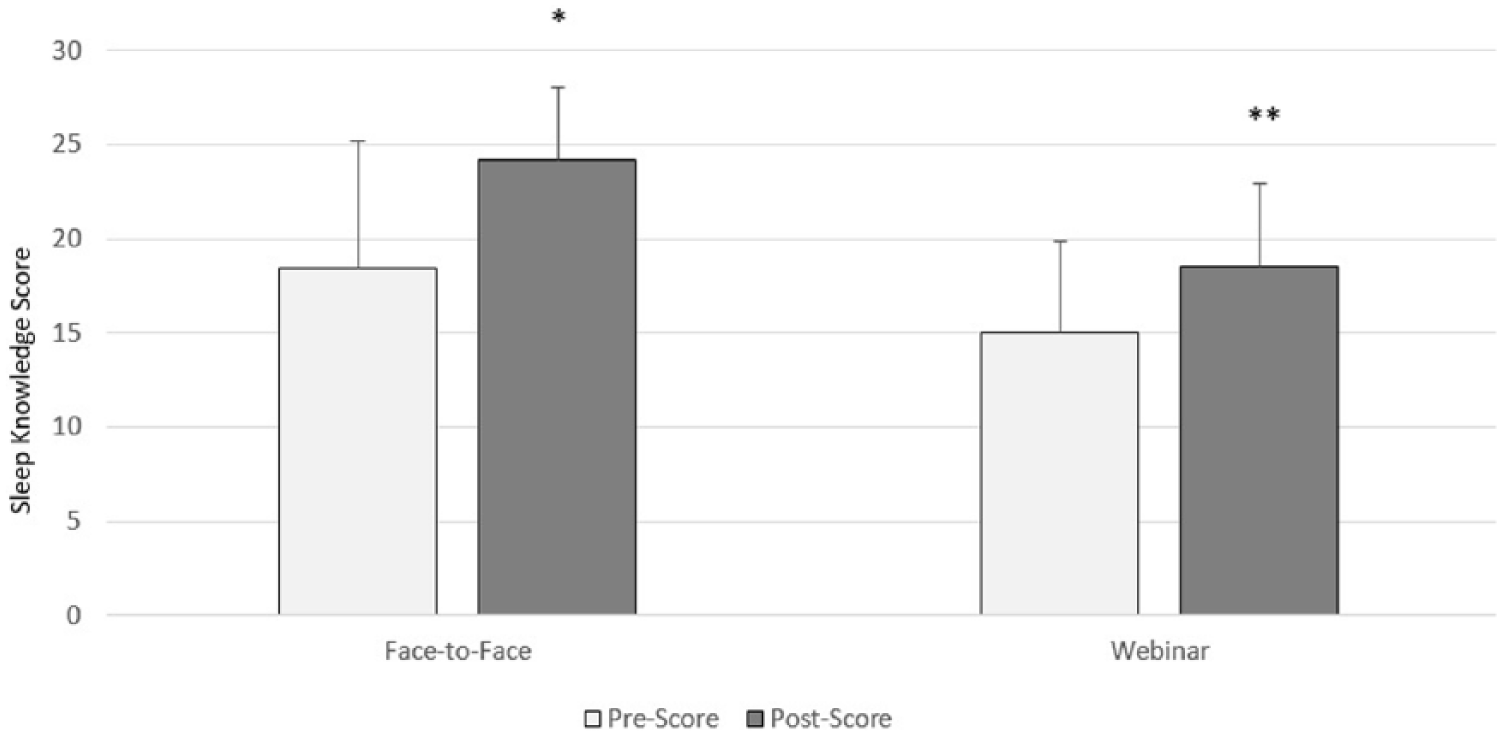
Parental Sleep Knowledge Acquisition. *P ⩽ .01; **P ⩽ .001.
An independent samples t test with an α level of .05 was used to compare the level of sleep knowledge acquisition in participants receiving face-to-face information delivery and participants receiving webinar information delivery. Levene test was non-significant, thus equal variances were assumed. The t test revealed that the Score Difference in the face-to-face group (M = 5.79, SD = 5.21) was on average 2.29 marks higher, 95% confidence interval [−1.04 to 5.61], than the webinar group (M = 3.50, SD = 4.00); however, this difference was not statistically significant, t(30) = 1.41, P = .170, 2-tailed, r2 = .06, and the effect size was small.
Participant characteristics.

Abbreviation: SES, socio-economic status.
Qualitative analysis
Webinar participant feedback emphasised the importance of sleep education, with 100% of participants believing that online delivery of sleep education was preferable to no sleep education at all and online sleep education was sufficient to increase their sleep knowledge, whereas 89% believed sleep education should be delivered to every new parent (see Table 3).
Sleep education webinar participant feedback.

Qualitative sleep knowledge
Qualitative results on the participant questions relating to the value and importance of receiving sleep knowledge suggest that parents want systematic sleep education and also that they see sleep education as acceptable either face-to-face or online. Overall, these data suggest that sleep education is efficacious in improving sleep knowledge, and generally both face-to-face and online methods are acceptable (see Table 3).
The final open-ended question was also analysed to ascertain what type of information parents required. At the completion of the webinar, 15 participants asked the speaker additional questions via online submission of their questions via the webinar portal. Thematic analysis of these post-seminar questions found that these parents wanted greater detail about topics already covered in the webinar such as sleep routines, duration, intervention strategies, sleep patterns/architecture, sleep aides, and individual differences (Table 1).
Discussion
This study was the first, to our knowledge, to test the efficacy and acceptability of sleep education delivery via webinar delivery compared with face-to-face delivery in parents of young children. Findings suggest that both methods of delivery are equally effective in improving knowledge and that there was no difference in knowledge acquisition between delivery modes. Parents reported needing and wanting sleep education and reported both modes of delivery to be acceptable. These findings strengthen the argument for sleep education for all new parents and specifically for those in regional or remote locations so that they need not be disadvantaged, if online delivery can be made accessible. 27 This supports evidence of the potential benefits of using a stepped care model in mental health care 26 and suggests that informal dissemination of information (ie, the first tier of the stepped care model) would help to satisfy the needs of parents at a primary level.
The hypothesis that there would be a significant increase in sleep knowledge between the ‘Pre-Score’ and the ‘Post-Score’ for both the face-to-face and webinar group was supported with all parents increasing their sleep knowledge. Interestingly, face-to-face group participants had a higher (non-significant) baseline level of sleep knowledge. This may be attributable to the fact that they had older children and a greater number of children, both of which may have enhanced their level of sleep knowledge (ie, through experience).
Both delivery modes are effective methods in enhancing sleep knowledge among parents/caregivers. It is noteworthy that while this study used a webinar portal, online delivery can be undertaken via varied and diverse systems and availability of compatible technologies is necessary for effective delivery.3,28 This is particularly important for parents residing in rural and remote areas, where limited access to specialised paediatric sleep specialists means these parents are less likely to receive adequate support3,28 and where a diverse range of technologies would likely be available. 27
The third hypothesis that there would be no significant difference between the mean ‘Score Difference’ across the webinar and face-to-face groups was also supported. This suggests sleep knowledge can be acquired as effectively through webinar delivery as it can through face-to-face delivery. These findings support Jones et al, 22 who found comparable knowledge acquisition of physical therapy educational information across delivery platforms (ie, classroom vs video link vs Web-based tutorials).
In addition, the use of an online delivery platform for dissemination of infant sleep behaviour education provides an opportunity to deliver this information through a cost-effective method and would fall within the stepped care model. Using a stepped care model reduces health care costs by allowing formal knowledge to be disseminated, either online or face-to-face, to wider communities, thus reducing the need for parents to access more specialised services. Although the sleep behaviour change literature suggests that the dissemination of knowledge alone does not necessarily elicit behaviour change,29,30 and so would not necessarily reduce actual sleep disturbance, knowledge is a basic requirement for progression into a sleep behavioural change process. 31 A plausible next step would be the systematic training of primary health care workers (eg, GPs and community nurses) in sleep education to deliver health care at the second tier of the stepped care model where necessary. Furthermore, in future trials, a methodical process evaluation could look in detail at the impact of parental sleep education on sleep-related decision making and behaviour such as described in Espie’s model. 17
Limitations of this pilot study include the small sample sizes which may reduce the likelihood of detecting significant differences between the groups due to limited statistical power. In addition, a convenience sampling method was used which may limit the generalisability of the findings. Therefore, future studies should investigate whether these findings are replicable in a larger, more diverse populations using a randomised controlled trial. Therefore, without this randomisation, it is possible that the demographic differences at each site in this study may have confounded the results. A final limitation was the use of the PSKI. Although the instrument has previously been used as a tool to measure sleep knowledge, 24 the instrument has not been validated and therefore its validity and sensitivity to change are unclear. Furthermore, ambiguous item wording, such as the word ‘sounder’, are ill-defined and open to individual interpretation on what constitutes ‘sounder’ sleep. Standard sleep knowledge questionnaires do not exist and most studies have had to develop their own. 13 Future scales measuring knowledge acquisition need to have clearly defined items with evidence-based rather than opinion-based answers to improve face validity.
Despite these limitations, this study provides evidence that delivery of sleep information through face-to-face or webinar platforms are both effective means of increasing sleep knowledge in parents/caregivers. Furthermore, the study findings suggest that the efficacy is equivalent across platforms, indicating that using a webinar platform to distribute sleep information has the potential to effectively improve sleep knowledge among parents/caregivers in the wider population, particularly those residing in rural areas where access to sleep specialists is limited. Online delivery is both cost-effective and has the potential to benefit a greater number of parents than face-to-face delivery alone by enabling more parents to access the information necessary to assist their management of infant sleep behaviours. Certainly, parents have reported that sleep education is both helpful and necessary which supports earlier work by this group. 12 Furthermore, it has the capacity to reduce the associated health risks to both parents and infants as well as the health care costs of the downstream consequences of poor infant sleep behaviours.
Conclusions
Promotion of good sleep health and dissemination of sleep health messages, especially to young families struggling with sleep disturbance, can be delivered effectively both face-to-face and online. As such, accessibility of specialist services to families even in remote and regional areas can therefore be better achieved.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Each author has made either a substantial contribution to the concept and design of the work, and/or acquisition, analysis and interpretation of data and drafting of the manuscript.