
Abstract
Fatalities from perinatal asphyxia remain high in developing countries, and continually assessing its risk factors will help improve outcomes in these settings. We explored how some identified risk factors predict mortality in asphyxiated newborns, to assist clinicians in prioritizing interventions. This was a 4-year prospective study conducted at the Enugu State University Teaching Hospital, Enugu, Nigeria. All newborns who met the study criteria that were admitted to this facility in this period were enrolled and monitored. Data collected were analysed with SPSS Version 18. A total of 161 newborns with perinatal asphyxia were enrolled into the study with an in-hospital incidence rate of 12.81 per 1000 birth and a case fatality rate of 18%. Overall, the APGAR scores were severe in 10%, moderate in 22%, mild to normal in 68%, whereas the SARNAT stages were III in 24%, II in 52%, and I in 25%. In terms of mortality, 66.7%, 22.2%, and 11.1% mortalities were, respectively, observed with SARNAT scores III, II, and I (P = .003), whereas the findings with APGAR were 31.2% (severe), 25.0% (moderate), 25.0% (mild), and 18.8% (normal) (P = .030). Fatality outcome was more correlated with SARNAT (R = .280; P = .000) than APGAR (R = −.247; P = .0125). The SARNAT score significantly differentiated between the degrees of asphyxia in newborns based on gestational age at delivery (P = .010), place of delivery (P = .032), and mode of delivery (P = .042). Finally, it was noted that newborns that were female (P = .007), or born outside the hospital (P = .010), or with oxygen saturations <60% (P = .001), or with heart rate <120 (P = .000), and those with respiratory rate <30 (P = .003), all have significantly higher likelihood of deaths from asphyxia. Therefore, predictors of neonatal mortality from perinatal asphyxia in our centre include being female and being born outside the hospital, as well as low oxygen saturations, heart rates, and respiratory rates at presentation.
Introduction
Perinatal asphyxia is an important clinical condition in the newborn period. It is a leading cause of morbidity and mortality in newborn babies globally, with higher case fatality rates and consequent complications in developing countries due to poor health facilities. According to the World Health Organization, perinatal asphyxia accounts for over a million newborn deaths annually and is a major cause of long-term neurologic disability and impairment in children. 1 In 2013 alone, about 10.5% of newborns globally and 29% in Nigeria died from perinatal asphyxia. 2 The characteristic hypoxaemia, hypercapnia, and acidosis seen in this condition are principally due to impairment of blood-gas exchange. The aftermath of these biochemical changes is a multisystemic dysfunction involving mainly the central nervous, renal, respiratory, digestive, and cardiovascular systems. 3 These dysfunctions include but are not limited to hypoxic ischaemic encephalopathy, cerebral palsy, varying degrees of intellectual disability, shock, disseminated intravascular coagulopathy, necrotizing enterocolitis, and hypoglycaemia. 4 Documented risk factors for perinatal asphyxia include lack of antenatal care, cephalo-pelvic disproportion, breech delivery, mode of delivery, gestational age, and prolonged rupture of membranes.5,6 Continued assessment of these risk factors is important with the slow but progressive development in obstetric and intrauterine care in developing settings. We studied the interplay between some identified risk factors and clinical findings at presentation in predicting mortality of asphyxiated newborns in a tertiary health facility in Nigeria. The findings will not only constitute some prognostic indices but also help clinicians in prioritizing interventions when caring for asphyxiated newborns.
Materials and Methods
Study area and site
This was a prospective study carried out at the neonatal intensive care unit (NICU) of Enugu State University Teaching Hospital (ESUTH), Parklane. The site is located within Enugu, the capital city of Enugu State, South-East Nigeria. Enugu State University Teaching Hospital is a tertiary health institution that offers specialized medical services and serves as a referral centre to the primary and secondary health facilities within the state and its environ. Referrals are seen from Private, General, Mission hospitals, and other delivery homes within Enugu and neighbouring state. The NICU offers 24-hour services to sick babies born within and outside the hospital and is located near the labour ward with an average delivery rate of 144 per month. The NICU is equipped with 4 functional incubators, an open incubator (with radiant warmer), and facilities for Kangaroo Mother Care. The unit also has a newborn infant ventilator (SC-Y 200 infant ventilator), 6 improvized bubble continuous positive airway pressure devices, a unit of multiparameter monitor, a unit of handheld pulse oximeter. Other medications and equipment available in the unit include caffeine citrate injections, surfactant and oxygen delivery units, several units of bag-mask device, manual/electrical suction machines, etc. The NICU is manned on rotational basis by 2 consultant neonatologists, 5 resident doctors undergoing rotation in the unit, and 19 nurses, 3 of which are specialized paediatric nurses.
Newborn participation and enrolment
The study was conducted over a period of 3 years and 9 months (January 2013-October 2016). Newborn babies delivered in ESUTH (inborn) or referred to it (outborn) who had problems initiating spontaneous respiration were consecutively enrolled. Newborns with a number of conditions that could alter the diagnostic indices for perinatal asphyxia were excluded from the study. These include the following:
Newborn babies with congenital abnormalities, ie, congenital heart disease, hydrops foetalis, structural abnormalities especially those affecting the chest and abdomen, etc;
Newborn babies with extreme low birth weight <1 kg;
Newborn babies of mothers who received opioids and other depressant medications.
Prior to recruitment of each subject, a written informed consent in a language understood by study participants was obtained from every mother-newborn dyad. Participation in the study was entirely voluntary and no financial inducement whatsoever was involved. Consenting subjects were recruited consecutively as they were admitted and followed up with daily reviews till discharge or death.
Diagnosis of perinatal asphyxia
The diagnosis of perinatal asphyxia was clinically based on asphyxiation scores with laboratory investigations done to exclude and/or confirm other diagnosis. Asphyxiation scores used in clinical diagnosis were the APGAR and SARNAT staging (see below), whereas laboratory investigations done included serum electrolyte, urea, and creatinine in addition to random blood sugar at presentation. For this study, the diagnosis of perinatal asphyxia was confirmed by a neonatologist not involved in this study. A second paediatrician unaware of the initial diagnosis was also brought in to confirm or refute the diagnosis in all cases. The agreement rate was greater than 90%.
Measures
The following information was obtained on admission or at subsequent reviews using a structured researcher administered questionnaire. These include the outcome and predictor variables as follows. Outcome variables – this is the final outcome of newborns admitted for perinatal asphyxia in the special care baby unit during the study period. Newborn babies that had a fatal outcome were categorized as died and those discharged were categorized as survived. Predictor variables – these are independent variables that are related to newborn outcomes. They include birth and demographic variables, clinical parameters, laboratory parameters, and asphyxiation scores categorized as follows:
Birth and demographic variables: (1) age of patient at presentation categorized into <24, 24-48, and >48 hours of life; (2) sex – categorized into male and female; (3) gestational age at delivery (≥37 and <37 weeks), birth weight (<2.5, 2.5-4, and >4.0 kg); (4) head circumference (<33, 33-37, and >37 cm); (5) place of birth (inborn or outborn); (6) mode of delivery (spontaneous vertex ± assisted or operative); and (7) the indications for caesarean section where applicable were documented.
Clinical parameters obtained at presentation include rectal temperature using a mercury-in-glass contact thermometer (normal range: 36.0°C-38.0°C), respiratory rate (normal range: 30-60 cycles per minute), heart rate (HR) (normal range: 120-160 beats per minute [bpm]), and oxygen saturation using a handheld pulse oximeter (MD300A; ChoiceMMED Pulse Oximeter SN: 114007000084; Beijing Choice Electronic Technology Co. Ltd., Beijing, China). Normal range is ≥90%.
Laboratory parameters include random blood sugar using capillary blood obtained by heel prick and read using a glucometer (TysonBio EVOLVE Blood Glucose Meter SN: M14KA012202; Tyson Bioresearch, Inc., Chun-Nan, Taiwan). Normal range is 2.5 to 11 mmol/L. Electrolyte, urea, and creatinine – normal range: sodium 135-145 mmol/L, potassium 3.5-5.5 mmol/L, chloride 97-108 mmol/L, urea 2.5-8.8 mmol/L, creatinine 44.2-194.5 mmol/L).
Asphyxiation score using the APGAR score and SARNAT staging were both documented for each case. APGAR is an acronym for Appearance, Pulse rate, Grimace, Activity, Respiratory rate. The score is normally awarded at 1, 5, 10, 15, and 20 minutes after delivery and represents the degree of asphyxia in the baby. For this study, the APGAR score at 5 minutes was used because it correlates best with degree of asphyxia. For inborn newborns who presented before 5 minutes of birth, the APGAR parameters were assessed and scored. For outborn newborns, the APGAR score awarded at the delivery centre as recorded in the referral was documented. For outborn newborns with no APGAR score recording, the hospital where the baby was delivered was contacted for more information. Where the hospital could not be reached, a history of poor cry from birth with poor colour, respiratory distress, floppiness, and loss of primitive reflexes were used. The APGAR score was categorized as 0 to 3 (severe asphyxia), 4 to 5 (moderate asphyxia), 6-7 (mild asphyxia), and >7 (no asphyxia). To measure the degree of hypoxic encephalopathy in newborns enrolled for this study, a clinical staging using the Sarnat and Sarnat staging of hypoxic ischaemic encephalopathy 7 was applied at presentation and the babies were categorized into stages I, II, and III.
Overview of treatment of asphyxiated babies
Perinatal asphyxia is a neonatal emergency. Therefore, on presentation at the NICU, resuscitation is commenced immediately. If there is sign of meconium aspiration, the airway is thoroughly suctioned and intubated if necessary. However, if there is no sign of meconium aspiration present, the baby is dried thoroughly and any wet clothing removed. Airway patency is secured by placing the baby’s head in a sniffing position with slight extension of the neck, clearing the airway of any secretion at regular intervals as needed. In cases where admitted newborns are apnoeic and/or with HR below 100 bpm, positive pressure ventilation (PPV) is commenced immediately (after meconium aspiration has been excluded). Vital signs with particular interest to the HR are evaluated every 30 seconds by counting for 6 seconds and multiplying the rate by 10. If after 30 seconds of effective PPV, the HR is still <60 bpm, chest compression (CC) is commenced in addition to the PPV at a ratio of 3:1 (CC:PPV). This resuscitation process is continued for the next 30 seconds and reevaluated. Ionotropes such as epinephrine is given if HR is still <60 bpm after 1 minute of effective resuscitation. Other aspects of the management include the following:
Blood sugar is assayed at presentation and corrected if needed.
Venous blood samples are collected for electrolyte assay prior to fluid therapies. Any electrolyte imbalance detected is corrected accordingly.
Intravenous fluids such as intravenous normal saline bolus are used for cases with signs of hypovolemic shock. Other fluid therapies include dextrose water for the first day with subsequent addition of electrolytes (sodium) after 48 hours, and potassium after adequate urine output has been established.
Ionotropic agents such as dobutamine or dopamine are used to improve cardiac activity and/or renal perfusion if indicated.
Supplemental oxygen is given in cases where oxygen saturation (SP
Endotracheal intubations and/or mechanical ventilation are given for cases requiring prolonged PPV.
Anticonvulsants such as diazepam, phenobarbitone, and magnesium sulphate are used in cases with seizure.
Empirical antibiotic using broad-spectrum antibiotics is commenced as prophylaxis for neonatal infections.
Intravenous phenobarbitone is given for all cases with stage III hypoxic encephalopathy.
Cerebral decongestants such as intravenous dexamethasone are used in cases where cerebral oedema is suspected.
If asphyxiated newborn presents within 6 hours of birth, skin temperature is usually maintained at a range of 35.0°C to 35.6°C to offer some therapeutic hypothermia as the conventional cool cap for ideal therapeutic hypothermia therapy is not available in the study centre.
Data entry and analysis
The above measures were documented at presentation in the relevant sections of the questionnaire and subsequently transferred into a Microsoft Excel Sheet. Distribution of the measures of outcome and predictor variables were analysed and recorded in percentages. Missing data were excluded from the analysis. The χ2 analysis was used to assess predictor variables significantly associated with outcome in newborns with perinatal asphyxia. Data were analysed using IBM SPSS version 18.0 (SPSS Inc., Chicago, IL, USA). Statistical significance was set at P < .05.
Ethical consideration
Ethical clearance was obtained from the ESUTH Ethics Committee. Informed consent was obtained from every mother-newborn dyad in their own right before recruitment. Participation in the study was entirely voluntary and no financial inducement whatsoever was involved. Voluntary withdrawal at any stage of interaction was guaranteed for all subjects without any adverse effect for the mother or the baby. All information was handled with strict confidentiality.
Results
Characteristics of newborn enrolled in the study
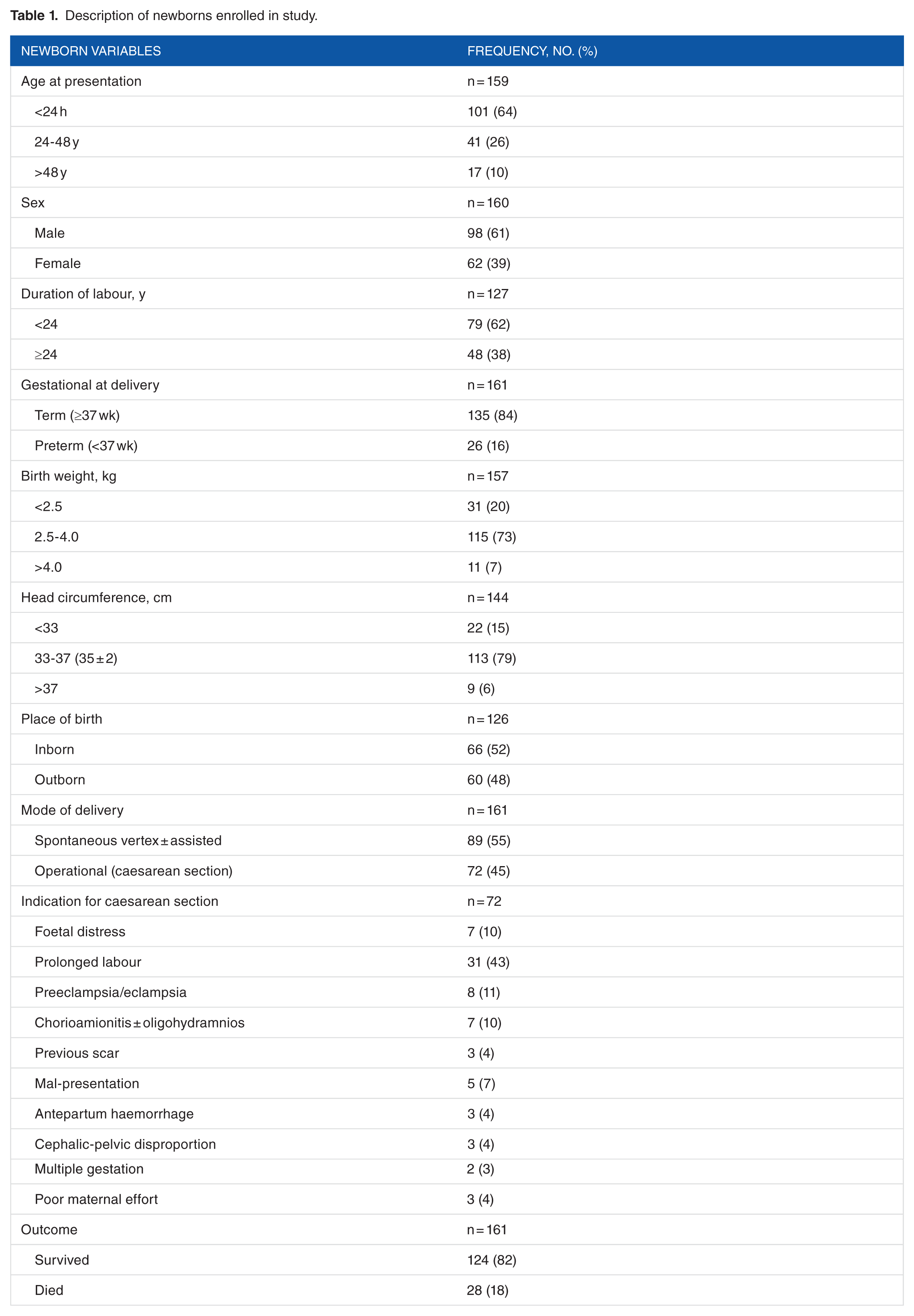
A total of 161 newborns who met the study criteria were enrolled into the study with approximately equal proportion born within and outside the ESUTH. Over 60% presented within the first 24 hours of birth, whereas 1 in 10 presented 48 hours after delivery. About 40% of the newborns were female and 61% were male. Most (84%) of the newborns were term babies, whereas the remainder were delivered before 37 completed weeks of gestation. Mode of delivery was via spontaneous vaginal delivery in 55% and caesarean section in the remaining 45% of cases. Prolonged labour accounted for almost half of the indications for caesarean section in all 72 cases of operative deliveries. Most of the newborns had birth weight (73%) and head circumference (79%) within normal range. Of the 161 newborns, 28 (18%) managed for perinatal asphyxia had a fatal outcome (see Table 1).
Description of newborns enrolled in study.
The mean age at presentation to special care baby unit for newborns born within ESUTH was 5.99 hours (confidence interval [CI]: 3.18-8.80) compared with 34.63 hours (CI: 23.34-45.92) for newborns born outside the hospital (T = 6.37, P = .001). The minimum age at presentation for newborns born within and outside the ESUTH was 0.1 hour (6 minutes) vs 1.3 hours (78 minutes) (T = 0.267, P = .790), whereas the maximum age at presentation was 24 hours (1 day) vs 192 hours (8 days) (T = 37.36, P = .000), respectively.
Table 2 shows some clinical parameters of admitted newborns. Random blood sugar (96%) and HR (86%) were within normal range of values in most of the asphyxiated newborns. Respiratory rate was above normal range in over half the newborns (51%), whereas oxygen was below normal saturation in 43% of the asphyxiated newborns. Electrolyte concentrations were mostly normal with potassium [K+] being the most commonly deranged ion with a value range of 3.1 to 7.2 mmol/L. Other electrolytes range of values included sodium [Na+] 126 to 146 mmol/L, chloride [Cl−] 88 to 112 mmol/L, urea 1.9 to 30.7 mmol/L, and creatinine of 3.0 to 172.5 mmol/L.
Clinical parameters on presentation.

Abbreviations: bpm, beats per minute; cpm, cycle per minute; HIE, hypoxic-ischaemic encephalopathy.
Newborn parameters, asphyxiation scores, and mortality
Of the 161 newborns with perinatal asphyxia enrolled, 88 (52%) were delivered in the hospital giving an in-hospital incidence rate of 12.81 per 1000 births. The APGAR scores were 0 to 3 (severe) in 10%, 4 to 6 (moderate) in 22%, mild to normal in 68% of the newborns with asphyxia, compared with SARNAT stage of III (severe) in 24% of newborns, II (moderate) in 52%, and I (mild) in 25% of the newborns. Both asphyxiation scores were highly correlated (R = −.459; P = .000) and significantly predicted severe asphyxiation in newborns with prolonged labour and fatality. However, only the SARNAT score significantly differentiated between the degrees of asphyxia in newborns based on gestational age at delivery (P = .010), place of delivery (P = .032), and mode of delivery (P = .042) (see Table 3).
Crosstabulation of newborn parameters and asphyxiation scores.
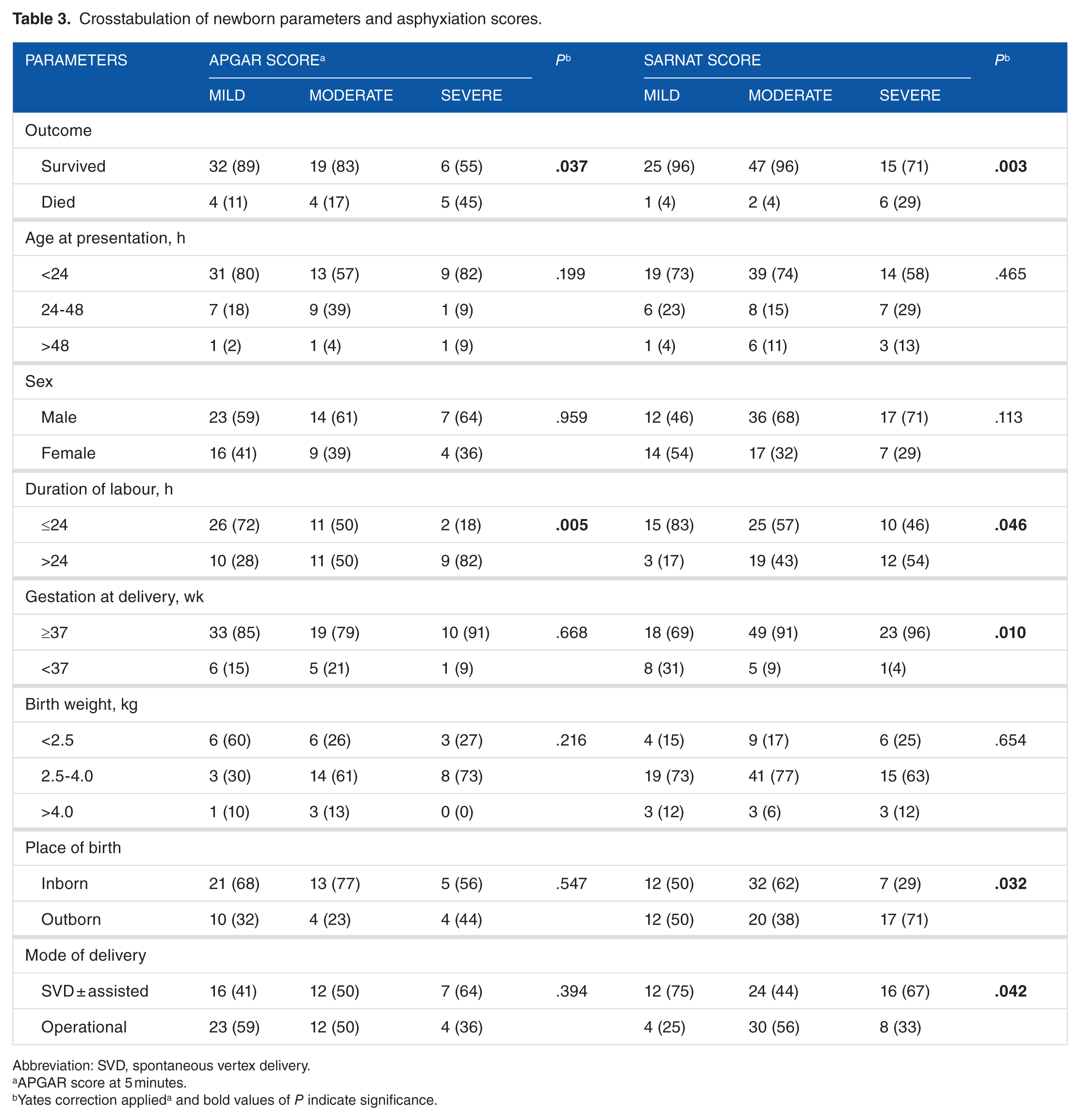
Abbreviation: SVD, spontaneous vertex delivery.
APGAR score at 5 minutes.
Yates correction applieda and bold values of P indicate significance.
A case fatality rate of 18% was observed among asphyxiated newborns. There was no significant difference in mortality between newborns that presented with temperature <36°C and ≥36°C (18.4% vs 17.2%; P = .868). Stratification based on asphyxiation score showed that 66.7%, 22.2%, and 11.1% of the mortality was among newborns with SARNAT stages III, II, and I, respectively (P = .003) compared with 31.2%, 25.0%, 25.0%, and 18.8% with newborns with severe, moderate, mild, and normal APGAR scores, respectively (P = .030). Fatality outcome was more correlated with the SARNAT staging system (R = .280; P = .000) than the APGAR scoring system (R = −.247; P = .0125).
Finally, it was noted that female newborns (P = .007), newborns born outside the hospital (P = .010), newborns with oxygen saturation less than 60% at presentation (P = .001), newborns with HR <120 (P = .000), and respiratory rate <30 (P = .003) at presentation were significantly more likely to die from perinatal asphyxia compared with newborns in the same subcategory (Table 4). Further analysis of case fatalities with SARNAT staging stratified by sex of the newborns further established that female newborns were more likely to die compared with male newborns across all stages of asphyxia, ie, SARNAT I (0.0% vs 7.1%), SARNAT II (3.0% vs 6.7%), and SARNAT III (6.7% vs 83.3%).
Determinants of mortality in asphyxiated newborns.
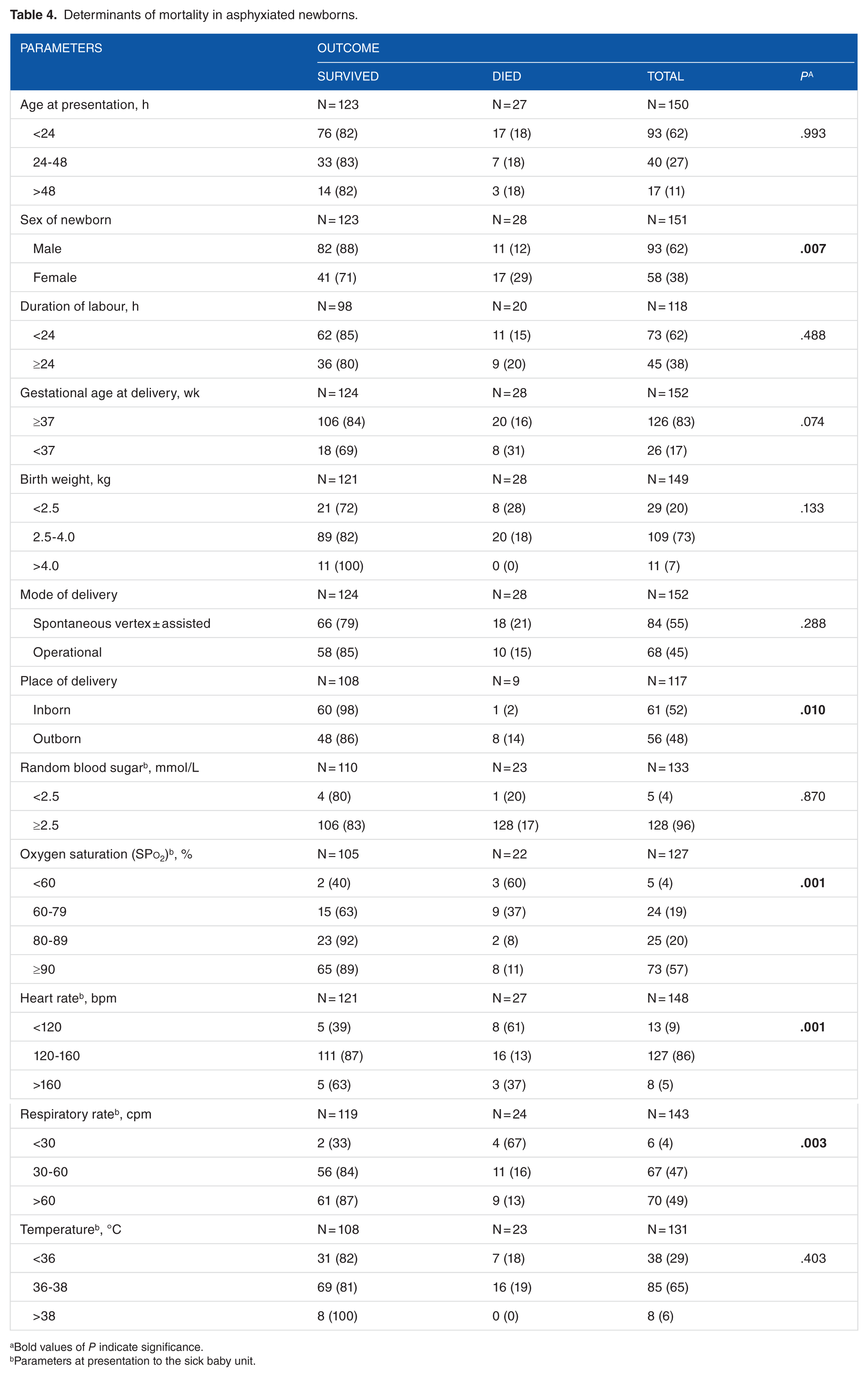
Bold values of P indicate significance.
Parameters at presentation to the sick baby unit.
Discussion
This study showed a high prevalence of operative deliveries due to prolonged labour (43%) which is a well-documented cause of perinatal asphyxia. The rates may be higher in developing than developed countries because of the higher prevalence of risk factors that predisposes to prolonged labour, as well as the lack of appropriate interventions. 8 In a study on 313 women during term labour in West Bengal, Eastern India, it was noted that perinatal asphyxia secondary to prolonged labour was the commonest cause of perinatal morbidity. 9 Recognizing the unacceptable maternal and child deaths together with the long-term neurological outcome of prolonged labour, the World Health Organization released in a document recommendations as to how to prevent prolonged labour during deliveries. These include training of birth attendants in resuscitation skills, risk factors identification, assessing pelvic outlet, diagnosing presentation and position of the baby, assessing descent of the foetal head, recognizing obstructed labour, and vacuum extraction when indicated. 10 Thus, basic resuscitation by birth attendants competent in resuscitation would substantially help reduce deaths from perinatal asphyxia. It has been reported that home-based interventions delivered by a team of traditional birth attendants (TBAs) and a semiskilled village health workers reduced the asphyxia-related neonatal mortality by 65% compared with only TBAs. 11
In addition, it was seen in this study that 18% of cases of perinatal asphyxia ended in fatalities with two-thirds of this been among the severely asphyxiated newborns. The rate seen in this study is lower than the case fatality of 25.5% recorded in a similar study in Gusau, Nigeria 12 ; 30% in Kathmandu, Nepal 13 ; and the 20% observed in Johannesburg, South Africa. 14 The difference in this prevalence may be related to the level of man power, skills, and facilities available in these centres for the care of asphyxiated newborns. However, such figures are still unacceptably high and demands intensified efforts in the improvement of skills and resources in the intensive care unit for management of newborns with asphyxia and related morbidity.
Perinatal asphyxia is an important cause of metabolic derangements and acute neurologic injury in newborns, and immediate aggressive treatment of these abnormalities could modify the entire outcome of the babies. 15 Electrolyte imbalance may also be used as a predictor of morbidity and mortality in asphyxiated neonates. Our study showed various degrees of electrolyte derangements with potassium and sodium ion being most affected. This agrees with the findings in a case-control study which noted that among cases, hyponatraemia and hypocalcaemia developed early and were directly proportional to each other and to the degree of asphyxia. 16 That study also reported that although mean potassium level was within the normal limit, the value was higher among cases than controls and was also directly proportional to degree of asphyxia. However, another study in Rawalpindi Hospital, Pakistan, found hyponatraemia and hypocalcaemia but normal serum potassium levels in perinatal asphyxia cases. 15
Furthermore, our study showed a higher correlation of SARNAT staging to mortality in perinatal asphyxia and its superiority in distinguishing between the various degrees of perinatal asphyxia than APGAR scores. This is not surprising as the SARNAT scoring system, unlike the APGAR score (which uses mainly physical and some vital signs to predict the degree of asphyxiation), is a more robust scoring system that incorporates levels of consciousness, neuromuscular control (muscle tone, stretch reflex, and posture), primitive reflexes (Monro, tonic neck and suck), autonomic function (pupillary reflex and HR), and presence or absence of seizures. 7 This is all in addition to the criteria included in APGAR scoring system. 17
It was also observed that the respiratory rate, HR, oxygen saturation at presentation along with the place of delivery, and sex of newborn were significantly associated with case fatalities in perinatal asphyxia. This could basically be explained by the fact that tissue oxygenation which is a function of respiratory rate, HR, and oxygen saturation is a key determinant of hypoxia and consequently hypoxic encephalopathy in perinatal asphyxia. Hypoxic encephalopathy measured by SARNAT staging system was seen to predict mortality in asphyxiated newborns in our study.
Similarly, it was found that newborn delivered outside ESUTH were more likely to die compared with those delivered within the hospital. This finding corroborates the observation of a similar study in Osogbo, Southwestern Nigeria. 18 This difference in mortality rate seen in our study between newborns delivered within the study facility and those referred from outside may be accounted for by several factors. First, being a tertiary hospital with relatively higher number of well-trained medical personnel and better facilities, it is expected that birth delivery services would be superior compared with services provided in most private hospitals, by TBAs and in home deliveries. 19 Second, mothers who delivered in the teaching hospital are more likely to have attended antenatal care services and associated services compared with those who delivered outside. 20 Consequently, their deliveries would have been better planned in anticipation of complications during labour. Third, the significantly higher age at presentation of neonates born outside the hospital as noted in this study which is reflective of late presentation may also be a factor in higher case fatality compared with newborns delivered within the hospital.
Finally, case fatality was seen to be higher in female newborns compared with male newborns. It is not clear why this is the case, but this finding seems to differ, in part, from the findings of studies which reported that preterm male babies are at higher risks of asphyxiation and require more resuscitations than their female counterparts.21,22 We believe, however, that future researches designed to resolve this finding would be worthwhile.
Conclusions
We conclude that the predictors of neonatal mortality from asphyxia in our centre include been female and born outside the hospital. In addition, the other predictors include neonates who had oxygen saturations of less than 60% on room air, a HR of ≤120 per minute, or a respiratory rate of less than 30 per minute.
Limitations
The authors used history and physical findings for scoring and diagnosis of perinatal asphyxia in some enrolled newborns delivered outside the hospital where this study was conducted. Using historical method in estimation of APGAR score is prone to recall bias and may lead to errors in classification.
Recommendations
There is need for training and retaining of health workers in the art of newborn resuscitation, especially those taking deliveries outside the tertiary health facilities. They should also be trained to recognize danger signs early enough and initiate referral promptly. Government should enhance early referrals by providing ambulances and good roads linking the referral centres with other health faculties.
Footnotes
Acknowledgements
The authors wish to thank all the specialist registrars who assisted in data collection during their clinical neonatal paediatric posting in the Special Care Baby Unit. Of note are Dr Ani OS, Dr Agwu Samuel, and Dr Orji Ngozi. We are also grateful to the highly dedicated staff nurses in the Special Care Baby Unit and the Labour ward under the headship of Matron Onovo Priscilla, for their tireless efforts in some study-related documentations and heroic efforts in salvaging dying newborns.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was completely funded through equal contribution from all authors.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
This study was done in collaboration between all authors. UE and INA conceptualized the study, drafted the methodology, supervised data collection and reviewed the manuscript draft. CDIO contributed in drafting the methodology, did the statistical analysis and wrote the result and discussion section. IKN contributed to the writing of the result and discussion, assisted in supervision of data collection and reviewed the manuscript draft. CI wrote the abstract, contributed in discussion and reviewed the manuscript draft. ICC, WOO and IBO contributed in supervision of data collection and reviewed the final manuscript. OFA and JCO supervised the work and reviewed the manuscript.
Ethical Approval and Consent to Participate
Ethical clearance was obtained from the Enugu State University Teaching Hospital Ethics Committee. Informed consent was obtained from every mother-newborn dyad in their own right before recruitment. Participation in the study was entirely voluntary and no financial inducement whatsoever was involved. Voluntary withdrawal at any stage of interaction was guaranteed for all subjects without any adverse effect for the mother or the baby. All information was handled with strict confidentiality.