
Abstract
Background:
Surgical intervention, complemented by radiotherapy and chemotherapy with temozolomide, constitutes the conventional treatment protocol for patients with newly diagnosed grade 4 glioma. We have conducted a research to evaluate the efficacy and safety of an integrated treatment regimen that incorporates tumor-treating fields with concurrent chemoradiotherapy.
Methods:
This retrospective research analyzed the clinical data of 39 adults who were newly diagnosed with World Health Organization (WHO) grade 4 gliomas at the First Affiliated Hospital of Nanjing Medical University, between February 2022 and April 2023. Each participant received a concurrent treatment regimen consisting of temozolomide (75 mg/m2 daily), tumor-treating fields (200 kHz), and brain irradiation (60 Gy delivered in 30 fractions). Maintenance treatment comprised ongoing temozolomide and tumor-treating fields. Adverse events were documented in accordance with the Common Terminology Criteria for Adverse Events version 5.0 (CTCAE 5.0) and specific grading criteria for dermatological adverse events associated with tumor-treating fields.
Results:
Among the 39 enrolled patients, disease progression was observed in 22 individuals (56.4%), with a median progression-free survival (PFS) of 14.2 months (95% confidence interval [CI]: 13.1-14.3 months). The median overall survival (OS) was 18.2 months (95% CI: 17.3 months to not reached). Patients diagnosed with glioblastoma had a median PFS of 13.1 months (95% CI: 12.9-14.2 months) and a median OS of 18.2 months (95% CI: 17.3 months to not reached). In contrast, patients diagnosed with astrocytoma had a median PFS of 14.3 months (95% CI: 12.8 months to not reached) and a median OS of 17.0 months (95% CI: 10.6 months to not reached). Twenty-five patients (64.1%) experienced dermatological adverse events, and 30 (77.0%) experienced mild hematological adverse reactions related to chemoradiotherapy.
Conclusion:
The application of tumor-treating fields concurrent with post-surgery chemoradiotherapy is both safe and effective for treating patients with newly diagnosed WHO grade 4 gliomas, exhibiting only limited toxicity.
Introduction
Glioblastoma, characterized by rapid progression, aggressive invasion, and poor prognosis, 1 remains the most common primary malignant brain tumor in adults. The 2021 revision by the World Health Organization (WHO) in the classification of central nervous system tumors is substantially influenced by isocitrate dehydrogenase (IDH) mutation status. 2 This revision restricts the diagnosis of glioblastoma to IDH wild-type tumors; reclassifies tumors previously identified as glioblastomas with IDH mutations as astrocytomas, IDH mutated, and grade 4; and stipulates the presence of IDH mutations for the classification of astrocytomas and oligodendrogliomas. 3 This updated classification scheme provides clinicians with enhanced diagnostic accuracy, thereby improving prognostic assessments and therapeutic strategizing for patients.
With the evolution of medical technology, tumor-treating fields (TTFields), an innovative tumor treatment modality, has been incorporated into several prominent clinical guidelines, including the National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines in the United States 4 and the 2018 Edition of the Chinese Guidelines for Diagnosis and Treatment of Gliomas. 5 Recent research indicates that TTFields may disrupt DNA repair mechanisms in tumor cells and increase stress on DNA replication, potentially enhancing the effectiveness of concurrent radiotherapy and temozolomide (TMZ) chemotherapy.6,7 The TTFields inhibit mitosis in cancer cells primarily by exerting electrical forces on microtubule/septin proteins, causing a dielectrophoretic effect that suppresses the mitotic process of tumor cells. 8 Following radiation-induced DNA damage, TTFields downregulate the BRCA/FANC genes, affecting homologous recombination repair of DNA and inducing errors in, and disintegration of DNA replication forks, increasing DNA replication stress and double-strand DNA damage in tumor cells. 9 Concurrent TTFields and radiation therapy can synergistically increase the killing rate of tumor cells and delay DNA damage repair. The TTFields and TMZ can act at different stages of mitosis, and their combined use can have an additive cytotoxic effect. 6
Based on the theoretical constructs previously discussed and acknowledging the limited domestic research in this area, we support a rigorous investigation into the efficacy and safety of TTFields combined with concurrent chemoradiation in the treatment of patients newly diagnosed with grade 4 gliomas. We conducted a retrospective analysis in 39 patients who were newly diagnosed with WHO grade 4 gliomas. This research bridged the empirical gap in the practical clinical application of this treatment modality in China, especially considering an ongoing international multicenter Phase III clinical trial that has yet to yield conclusive data for this geographical region.
Materials and Methods
Patient clinical characteristics
This retrospective research analyzed the clinical data of 39 adults at the First Affiliated Hospital of Nanjing Medical University, between February 2022 and April 2023. Eligible patients included adults, aged ⩾ 18 years, with a Karnofsky Performance Status (KPS) score of ⩾ 60, who had a confirmed diagnosis of grade 4 glioma according to the WHO, and who completed a 42-day course of TTFields treatment concurrently with chemoradiation therapy. Patients with severe pre-existing conditions, multiple cancers, known allergies to conductive hydrogel, or previous radiotherapy or TMZ treatment were excluded. Cases involving palliative surgical resection of tumors located solely in the brainstem were also excluded given the high postoperative complications and mortality rates.
Pathology and molecular testing
The tumor O(6)-methylguanine-DNA-methyltransferase (MGMT) methylation status, IDH mutation status, and co-deletion status of chromosome arms 1p and 19q were tested on tumor specimens at the Department of Neurosurgery at the First Affiliated Hospital of Nanjing Medical University.
Tumor-treating fields
The NovoTTF-200A treatment device, which was authorized by the National Medical Products Administration in 2020, was used in this research. The initial preparatory steps included depilating the patient’s scalp to ensure a smooth surface, followed by disinfection with a gauze pad soaked in 75% medical alcohol. Under the guidance of a physician, four transducer array patches—two black and two white—were meticulously positioned on the scalp. The black patches were placed at the front and back, whereas the white patches were positioned on either side of the head, ensuring optimal adherence to the scalp. These patches, which are crucial for the device’s functionality and are connected via a junction box, required replacement at least biweekly or as frequently as every 4 days, in accordance with a strict protocol.
To minimize skin irritation caused by the adhesive patches being in a fixed position over a long period, the physicians instructed the patients to slightly move the new patches by 1 to 2 cm with each replacement. Research has shown that the effect of the TTFields arrays on the dosage received by the target area is negligible, remaining within a 2% variation, 10 allowing for the patches to remain in place during concurrent chemoradiation therapies. Patient compliance with treatment is significantly enhanced by combining the use of patches with a radiotherapy sponge mask.
Effect assessment
Serial brain magnetic resonance imaging (MRI), performed every 3 months and supplemented with regular telephone follow-ups, was used to monitor the treatment response and disease progression, adhering to the Updated Response Assessment Criteria for high-grade gliomas set by the Response Assessment in Neuro-Oncology Work Group (RANO criteria). 11 The specialist physician for TTFields examines the patient’s skin condition monthly to determine the dAE grade. The primary research endpoints were progression-free survival (PFS), defined as the interval from the initiation of radiation therapy to the first observation of disease progression or death, and OS, measured from the start of radiation therapy to the occurrence of death.
Toxicity
Routine follow-ups were meticulously conducted on patients, with adverse events (AEs) documented in accordance with the Common Terminology Criteria for Adverse Events version 5.0 (CTCAE v5.0) and the specific grading criteria for dermatological adverse events (dAEs) associated with TTFields. To assess safety concerns related to TTFields, both adverse and serious adverse reactions were monitored, along with the grading of skin-related AEs.
A professional physician assessed the dAEs at least once a month, categorizing them into the following four levels: grade 1 dAE, in which the patient is asymptomatic or exhibits mild symptoms, suggesting the need for local treatment (eg, antibiotics or steroid creams); grade 2 dAE, in which the patient shows moderate symptoms, indicating the requirement for local or systemic treatment (eg, antibiotics or steroids); grade 3 dAE, in which the patient presents severe or medically significant but not immediately life-threatening conditions, suggesting the need for local or systemic treatment, the need for surgical intervention, or an extended hospital stay; and grade 4 dAE, which is life-threatening and requires urgent intervention.
Routine blood tests, including complete blood counts and comprehensive biochemical profiles, were regularly conducted to monitor potential adverse reactions during treatment, with a focus on leukopenia, neutropenia, thrombocytopenia, anemia, and electrolyte imbalances. In the event of abnormalities, an adverse event assessment was performed and symptomatic treatment was provided.
Statistical analysis
The PFS and OS were evaluated across the cohort using Kaplan-Meier estimates. The log-rank test was employed to determine the statistical significance of survival disparities between the two comparative groups, with P-values < .05 indicating statistical significance. Similarly, the chi-square test confirmed these differences as statistically significant, also using a 0.05 threshold. Comprehensive statistical analyses were performed using R (v.4.2.3). Moreover, descriptive statistical analyses were conducted on data pertaining to acute toxicity and duration of TTFields usage.
Results
Clinical characteristics
A cohort of 39 patients with newly diagnosed WHO grade 4 gliomas underwent TTFields in conjunction with standard postoperative chemoradiotherapy. The group included 23 males (59.0%) and 16 females (41.0%), with a median age of 59 years, ranging from 18 to 81 years. The median KPS was 90, ranging from 60 to 100. The rate of complete surgical resection was 79.5% (with a partial resection rate of 20.5%, all presenting with multiple lesions; see Table 1). Comparative analysis of baseline characteristics between the astrocytoma and glioblastoma cohorts revealed no significant disparities (see Table 2).
Clinical characteristics of all patients.
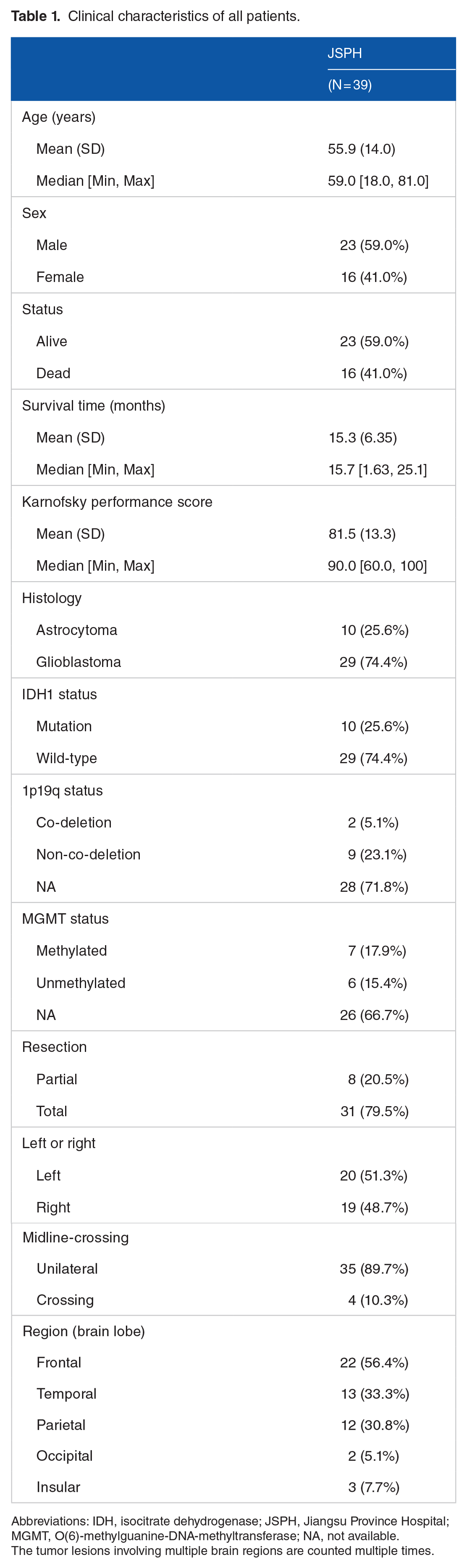
Abbreviations: IDH, isocitrate dehydrogenase; JSPH, Jiangsu Province Hospital; MGMT, O(6)-methylguanine-DNA-methyltransferase; NA, not available.
The tumor lesions involving multiple brain regions are counted multiple times.
Clinical characteristics of patients in the two cohorts.

Abbreviations: JSPH, Jiangsu Province Hospital; MGMT, O(6)-methylguanine-DNA-methyltransferase; NA, not available.
The tumor lesions involving multiple brain regions are counted multiple times.
During the administration of TTFields, the patients demonstrated good treatment compliance. The median total duration of TTFields was 1.8 months, ranging from 0.3 to 14.7 months. The median daily duration of therapy was 20.4 hours, ranging from 13.8 to 22.6 hours. Overall, the median compliance with the treatment regimen was 85.0%, ranging from 57.6% to 94.0%.
PFS and OS
At the time of writing, disease progression occurred in 22 (56.4%) patients, with a median PFS of 14.2 months (95% confidence interval [CI]: 13.1-14.3 months) and a 1-year PFS rate of 66.7% (95% CI: 53.4%-83.2%; see Figure 1). Among the subgroups, patients diagnosed with glioblastoma exhibited a median PFS of 13.1 months (95% CI: 12.9-14.2 months), whereas those diagnosed with astrocytoma demonstrated a median PFS of 14.3 months (95% CI: 12.8 months to not reached; see Figure 1). Analysis of treatment duration revealed that patients with less than 20 hours of daily usage had a median PFS of 12.9 months (95% CI: 12.8-13.1 months), whereas those with daily usage exceeding 20 hours had a median PFS of 14.3 months (95% CI: 14.2-16.0 months).

Kaplan-Meier estimates of progression-free survival and overall survival are represented by solid lines. The dashed lines indicate the corresponding 95% confidence intervals for these pointwise estimates. JSPH indicates Jiangsu Province Hospital; OS, overall survival; PFS, progression-free survival; SP, survival proportion.
The median OS was 18.2 months (95% CI: 17.3 months to not reached) and the 1-year OS rate was 74.4% (95% CI: 61.9%-89.4%; see Figure 1). Analyzing the subgroups, patients diagnosed with glioblastoma exhibited a median OS of 18.2 months (95% CI: 17.3 months to not reached), whereas those diagnosed with astrocytoma demonstrated a median OS of 17.0 months (95% CI: 10.6 months to not reached; see Figure 1). Regarding the treatment duration, patients receiving less than 20 hours per day showed a median OS of 17.3 months (95% CI: 17.0 months to not reached), whereas patients receiving more than 20 hours daily exhibited a median OS of 18.2 months (95% CI: 16.7 months to not reached).
Toxicity
During the 42-day administration of TTFields concurrent with chemoradiotherapy, scalp-related AEs were documented in 24 patients (61.5%). The majority of these events were classified as grade 1 dAEs, affecting 23 patients (59.0%), and a single case (2.6%) was recorded as a grade 2 dAE, necessitating temporary discontinuation of TTFields for drainage treatment of the affected area. There were no reports of grade 3 or 4 dAE events (see Table 3). Patients experiencing grade 1 dAEs received local treatment, which included adjusting the transducer array placement and applying antibiotic and steroid creams after ensuring that the wounds were kept dry; this approach led to an improvement in their condition. None of the patients with grade 1 dAE needed to interrupt their TTFields because of scalp reactions. In contrast, the patient who experienced a grade 2 dAE required drainage treatment for a purulent wound and had to temporarily cease TTFields. Illustrative examples of scalp adverse reactions are depicted in Supplementary Figure 1. Furthermore, in the group with less than 75% compliance (10 patients), all had grade 1 dAE, whereas in the group with compliance above 75% (29 patients), 15 showed no scalp reactions, 13 experienced grade 1 dAE, and 1 had grade 2 dAE (P = .009).
Dermatological adverse events.

Abbreviation: dAE, dermatological adverse event.
Routine blood tests and biochemical analyses indicated no severe adverse reactions, classified as grade 3 to 4 (see Table 4). Among the side effects closely related to chemoradiotherapy, hematologic adverse reactions were observed in 30 patients (77.0%). Within this group, two patients (5.1%) developed grade 1 leukopenia and one patient (2.6%) developed grade 2 leukopenia; three patients (7.7%) suffered from grade 1 neutropenia and one patient (2.6%) suffered grade 2 neutropenia; three patients (7.7%) exhibited grade 1 anemia, while one patient (2.6%) exhibited grade 2 anemia; one patient (2.6%) had grade 2 thrombocytopenia; and 15 patients (38.7%) experienced a reduction in lymphocyte count to varying extents. In addition, two patients (5.1%) were diagnosed with grade 1 hypoalbuminemia; electrolyte imbalances were noted in five patients (12.8%) with hyponatremia, four patients (10.3%) with hypokalemia, one patient (2.6%) with hypernatremia, and one patient (2.6%) with hyperkalemia, all of which were categorized as mild disorders.
Hematologic adverse reactions.

All adverse events were documented in accordance with the Common Terminology Criteria for Adverse Events version 5.0 (CTCAE 5.0). No related adverse events > grade 3 were noted during either concurrent or maintenance phases.
Moreover, there were no events of falls, fractures, or other complications that could be considered to be associated with improper administration of TTFields.
Discussion
The TTFields is emerging as a distinguished noninvasive approach in the oncology treatment landscape, particularly for glioblastoma, where it is now heralded as the fourth cornerstone of therapy. 12 The TTFields inhibits mitosis in cancer cells primarily by exerting electrical forces on microtubule/septin proteins, causing a dielectrophoretic effect that suppresses the mitotic process of tumor cells. 8 The antimitotic effect increases with the intensity of the electric field. In the case of glioblastoma multiforme, when the treatment frequency is 200 kHz, the maximum inhibitory effect on the tumor can be achieved.6,13 Following radiation-induced DNA damage, TTFields downregulate the BRCA/FANC genes, affecting homologous recombination repair of DNA and inducing errors in, and disintegration of DNA replication forks, increasing DNA replication stress and double-strand DNA damage in tumor cells. 9 Concurrent TTFields and radiation therapy can synergistically increase the killing rate of tumor cells and delay DNA damage repair. The TTFields and TMZ can act at different stages of mitosis, and their combined use can have an additive cytotoxic effect. 6 Recent researches mainly focus on the application of TTFields following radiotherapy and chemotherapy in patients newly diagnosed with grade 4 gliomas. However, the basic research results on the synergistic effects of TTFields with radiation and chemotherapy have prompted clinicians at home and abroad to combine TTFields with radiation and chemotherapy during the concurrent chemoradiotherapy period after surgeries for new diagnosis of WHO Grade IV gliomas. A single-center, single-arm, small-scale study in the United States (NCT03477110) found that TTFields combined with concurrent chemoradiotherapy could effectively control local tumor progression in patients with newly diagnosed glioblastoma. 14 The EF-32 study (NCT04471844) is an ongoing randomized, two-arm, multicenter clinical trial that is investigating the combined application of TTFields with concurrent chemoradiotherapy in newly diagnosed glioblastoma, with a planned enrollment of 950 patients. Our research constitutes one of the initial domestic investigations into the efficacy and safety profiles of TTFields in conjunction with chemoradiotherapy.
In our research, we observed a median PFS of 14.2 months and OS of 18.2 months. These figures surpass the survival metrics of the monotherapy cohort in the EF-14 trial, 15 thereby underscoring the significance of TTFields when used in conjunction with standard chemoradiotherapy to prolong patient survival. Furthermore, when contrasted with the Spare 16 study conducted internationally, which observed a median PFS of 9.3 months and OS of 15.8 months, our research demonstrates substantially higher PFS and OS. In addition, patients who used the device for less than 20 hours per day had a median PFS of 12.9 months (95% CI: 12.8-13.1 months), whereas those who used it for more than 20 hours per day had a median PFS of 14.3 months (95% CI: 14.2-16.0 months). The median OS for patients with less than 20 hours of daily use was 17.3 months (95% CI: 17.0 months to not reached), and for those with more than 20 hours of daily use, the median OS was 18.2 months (95% CI: 16.7 months to not reached). Patients who adhered to the TTFields for more than 20 hours a day, corresponding to a compliance rate higher than 83.3%, exhibited a longer survival than those with a compliance rate less than 83.3%. In summary, clinical research, both domestically and internationally, suggests that TTFields can effectively inhibit the progression and recurrence of gliomas, thereby improving patient survival.
Unlike TMZ alone, TTFields do not increase systemic AEs. However, studies have shown an incidence of mild to moderate skin irritation beneath the transducer arrays of approximate 52% 15 with typical symptoms including localized redness, dermatitis, blisters, ulcers, and erosion. 17 In domestic reports, Yang Qunying reported that among 24 cases of high-grade glioma treated with TTFields, the main AEs were grade 1 dAEs (58.3%) and grade 2 dAEs (12.5%), with no grade 3 to 4 dAEs. 18 In addition, a clinical study involving 10 patients treated with combined TTFields and chemoradiation therapy found that 80% of participants experienced grade 1 to 2 skin toxicity related to TTFields. 19 In the international SPARE study, 83.3% of patients experienced grade 1 to 2 dAEs, which naturally subsided after topical medication, and no grade 3 to 4 dAEs. 16 Therefore, the combination of TTFields with concurrent chemoradiotherapy may increase the incidence rate of skin adverse reactions. Our investigation focused on assessing the safety of a 42-day regimen of TTFields combined with chemoradiotherapy. The results demonstrated that 61.5% of the patients experienced scalp AEs, among which 58.9% were categorized as grade 1 and 2.6% as grade 2, with no instances of grade 3 to 4 dAEs. Our results are superior to those of concurrent treatments abroad and show no significant difference from others. Furthermore, in the group with less than 75% compliance (10 patients), all had grade 1 dAE, whereas in the group with compliance above 75% (29 patients), 15 showed no scalp reactions, 13 experienced grade 1 dAE, and 1 had grade 2 dAE (P = .009). This indicated that extended exposure may induce dAEs that do not affect daily life. However, the side effects are minor compared with the health benefits of following the treatment properly. Consequently, the integration of TTFields with concurrent chemoradiotherapy does not substantially exacerbate scalp adverse reactions among patients diagnosed with newly identified WHO grade IV gliomas. Moreover, the discomfort associated with treatment can be significantly alleviated through the application of topical corticosteroids, strategic repositioning of the transducer arrays, maintenance of dry skin conditions, and utilization of an antiperspirant containing aluminum chloride solution, particularly under conditions of perspiration, thus facilitating optimal wound healing.19 -21
The predominant adverse reactions associated with chemoradiotherapy in glioma treatment pertain to hematologic complications. According to the existing literature, the incidence rates among patients with glioblastoma subjected to a standard chemoradiotherapy regimen alone are as follows: grade 3 to 4 neutropenia at 4%, thrombocytopenia at 3%, leukopenia at 2%, and anemia at less than 1%. 22 In contrast, in our research, no severe (grade 3-4) hematological adverse reactions were reported (see Table 4). Although we did not observe a significant escalation in hematologic complications, considering that this regimen only covers a 42-day research period, close monitoring is still required during subsequent TTFields combined with TMZ chemotherapy.
Conclusions
The application of TTFields concurrent with post-surgery chemoradiotherapy is both safe and effective for treating patients with newly diagnosed WHO grade gliomas, exhibiting only limited toxicity.
Supplemental Material
sj-docx-1-onc-10.1177_11795549251315579 – Supplemental material for Concurrent Tumor-Treating Fields and Chemoradiotherapy: Outcomes in Grade 4 Glioma Patients
Supplemental material, sj-docx-1-onc-10.1177_11795549251315579 for Concurrent Tumor-Treating Fields and Chemoradiotherapy: Outcomes in Grade 4 Glioma Patients by Jintan Li, Jincheng Tao, Hongyu Lu, Xiao Fan, Zhichao Wang, Yingyi Wang, Xiefeng Wang, Wei Yan, Yongping You, Yuandong Cao and Junxia Zhang in Clinical Medicine Insights: Oncology
Footnotes
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors disclosed receipt of the following financial support for the research: This work was supported by the Jiangsu Province Hospital (the First Affiliated Hospital with Nanjing Medical University) Clinical Capacity Enhancement Project [JSPH-MC-2021-27].
Authors’ Note
All authors read and approved the final article.
Author Contributions
JL contributed toward writing – review and editing, writing – original draft, software, methodology, investigation, and data curation. JT contributed toward writing – review and editing, writing – original draft, investigation, data curation, and conceptualization. HL contributed toward writing – review and editing, writing – original draft, investigation, and conceptualization. XF was involved in the investigation, software, and data curation. ZW was involved in the investigation and data curation. YW, XW, WY, and YY contributed toward resources and data curation. YC contributed toward writing – review and editing, resources, project administration, and data curation. JZ was involved in writing – review and editing, supervision, resources, project administration, conceptualization, and data curation.
Consent for Publication
Data Availability
Data produced or analyzed for this research can be obtained from the lead author upon reasonable request.
Ethics Approval and Consent to Participate
This research was approved by the Ethics Committee of the First Affiliated Hospital of Nanjing Medical University (approval number: 2024-SR-1143). The patients provided written informed consent to participate in this research.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.