
Abstract
Background:
Soft tissue sarcoma (STS) is a rare malignancy that affects soft tissues. It encompasses various subtypes and requires different treatment strategies. Doxorubicin is a commonly used anthracycline in the management of localized and metastatic STS. However, high doses of doxorubicin are associated with cardiotoxicity, which can significantly impact patients’ long-term outcomes. This study aimed to evaluate doxorubicin’s effect on cardiac function in patients with sarcoma and to correlate the frequency of cardiotoxicity with potential risk factors.
Methods:
A retrospective analysis was conducted on patients with sarcoma who were treated with doxorubicin between 2016 and 2022 at King Abdulaziz Medical City in Saudi Arabia. Patient demographic information, comorbidities, cardiac measurements, laboratory values, systemic therapy, and treatment outcomes were collected from electronic medical records. A statistical analysis was performed to assess the association between cardiotoxicity and various factors.
Results:
A total of 133 patients were included in the study, with a median age of 30 years. Cardiotoxicity was observed in 9% of the patients. Female patients had a significantly higher risk of developing cardiotoxicity. Patients with a higher Eastern Cooperative Oncology Group (ECOG) performance status and lower troponin I levels also had an increased risk of cardiotoxicity. However, there was no significant association between cardiotoxicity and the number of chemotherapy cycles, total cumulative dose of doxorubicin, or history of radiation. Furthermore, patients with cardiotoxicity had a higher risk of mortality. The overall survival of the patients was 18 months.
Conclusion:
Doxorubicin-associated cardiotoxicity is a concern for patients with sarcoma. Female patients and patients with a higher ECOG performance status are at an increased risk of developing cardiotoxicity. Careful monitoring and risk assessment are crucial for mitigating the adverse effects of doxorubicin treatment in patients with sarcoma. Future studies are warranted to validate these findings and explore preventive strategies for doxorubicin-induced cardiotoxicity in patients with sarcoma.
Background
Sarcoma is a rare type of malignancy that affects bones and soft tissues, comprising only 1% of adult malignancies. 1 Soft tissue sarcoma (STS) has more than 100 subtypes and typically affects the extremities, trunk, retroperitoneum, as well as the head and neck. 2 Each type may have a different clinical presentation, preferred treatment strategy, and prognosis.1,2 Globally, there were 13 500 new cases of sarcoma in the United States with an incidence rate of less than 6 cases per 100 000 in 2021, representing 1% to 2% of all adult cancer cases. 3 According to data from the Saudi Health Council in 2018, soft tissue malignancies accounted for 2% of all malignancies in patients aged between 15 and 29. However, the incidence of these malignancies decreased as the patients aged. 4
The treatment approach for sarcoma varies based on its histological subtype and location. Tumors that are localized to the trunk and retroperitoneum can be challenging to resect and are typically managed with cytotoxic chemotherapy. 5 Surgery, with or without pre-operative radiation, is considered the mainstay of treatment for localized sarcoma, while chemotherapy is reserved for those who have failed surgical treatment or have metastatic disease. 6 In such cases, systemic chemotherapy is used with the aim to prolong survival and improve quality of life. Currently, anthracycline-based regimens are considered first-line therapy, either as monotherapy or in combination with alkylating agents such as ifosfamide or other agents. 7 Doxorubicin, an anthracycline, has been used for more than 40 years and is still considered first-line therapy for sarcoma and other types of malignancies. 8
Patients on doxorubicin might experience various side effects ranging from nausea to myelosuppression which require careful monitoring. 9 Cardiotoxicity is a serious adverse event that may occur with anthracycline-based chemotherapy. Several pathways have been proposed through which doxorubicin can cause cardiotoxicity including autophagy, oxidative stress, and regulated cell death. However, the precise mechanisms are still unknown despite intensive research. 10 One study reported that out of 731 cancer patients who received anthracyclines, 247 patients developed mild cardiotoxicity, characterized by a left ventricular ejection fraction (LVEF) greater than 50% with elevated biomarkers, or at least 1 additional abnormal echocardiography parameter. 11 Moreover, acute cardiotoxicity, which typically occurs 2 to 3 days after administration of doxorubicin, is estimated to have an incidence rate of approximately 11%. Conversely, the incidence rate of long-term cardiotoxicity, which occurs within 30 days of doxorubicin administration, is much lower, with an estimated rate of 1.7%.12,13
The Arabian Gulf region currently lacks comprehensive studies on sarcoma, which means that local physicians treating these patients do not have access to statistics on the morbidity and mortality of chemotherapy, specifically doxorubicin. Given that sarcoma can affect young patients, it is crucial to develop effective treatment plans that promote long-term survival. To achieve this, it is necessary to investigate the impact of doxorubicin on cardiac function and toxicity in patients with sarcoma, as well as identify risk factors for cardiotoxicity. By doing so, we can improve monitoring and treatment regimens for these patients. Therefore, this study aimed to evaluate the effects of doxorubicin chemotherapy on cardiac function in patients with sarcoma and correlate the frequency of cardiotoxicity with potential risk factors.
Methods
Study setting and design
The study was conducted at King Abdulaziz Medical City (KAMC), Department of Medical Oncology, Ministry of National Guard—Health Affairs, Riyadh, Kingdom of Saudi Arabia. King Abdulaziz Medical City is a government-funded tertiary care hospital that provides clinical care, training, academics, research, and advanced medical technologies.
Inclusion and exclusion criteria
All patients treated with doxorubicin for sarcoma between 2016 and 2022 were included. We have included patients who were referred from other centers to our center and received doxorubicin-based regimens. Patients with known cardiac comorbidities, missing data, referred to our institution solely for diagnostic workup, benign tumors, or suspected malignancies, and those lacking a pathology report or with an indecisive pathology report were excluded. Cardiotoxicity was defined as a reduction in LVEF, as accessed via echocardiography, falling by 20% from a previously established baseline ejection fraction within the normal range or an absolute LVEF of less than 50%. 14
Data collection
The required data were obtained by screening all the oncology electronic records (via the KAMC electronic system “BestCare”). The following data were collected: demographics, comorbidities, cardiac measurements including pulmonary artery pressure, left atrial pressure, LVEF initial at diagnosis, best result, and after recovering, cardiac comorbidities including atrial fibrillation aortic stenosis and regurgitation, mitral stenosis and regurgitation. In addition, laboratory values such as troponin values, B-type natriuretic peptide (BNP), and Eastern Cooperative Oncology Group (ECOG) performance status, systemic therapy, number of cycles, total cumulative dose of doxorubicin, and history of external beam radiotherapy were collected.
Statistical analysis
The data were analyzed using the Statistical Package for the Social Sciences (SPSS version 22). The results were presented as frequency and percentage for categorical variables and mean ± standard deviation for numerical variables. The association between categorical variables was tested using the chi-square or Fisher exact test, and an independent sample t test was used to test the association between numerical variables of patients who had cardiac toxicity and who had not. A two-sided P value less than .05 was considered significant.
Results
Baseline characteristics, demographics, and comorbidities
A summary of the patients’ baseline characteristics and comorbid conditions is shown in Table 1. A total of 133 patients between 2016 and 2022 were included in this study. More than half of the patients (n = 84, 63.1%) were male. The mean age of the patients was 36.2 ± 18 years, with a median age of 30 years. In addition, our patients had a mean body mass index (BMI) of 25.1 ± 8 kg/m². Comorbid conditions were present in a significant portion of the patients. The most notable ones were hypertension, diabetes, long-term lung disease, long-term kidney disease, dyslipidemia, and hypothyroidism, accounting for 17.29%, 14.29%, 6.02%, 4.51%, 3.76%, and 3.76% of the patients, respectively. Overall, the results indicated that only a small proportion of patients were smokers (n = 9, 6.77%), and 9.02% (n = 12) have been exposed to thoracic radiation. The most frequent types of sarcomas were Ewing sarcoma (30.83%), osteosarcoma (21.80%), and leiomyosarcoma (11.28%) (Table 2). The most frequent systemic therapy administered was a combination of vincristine, doxorubicin, cyclophosphamide alternating with ifosfamide, etoposide (VAC/IE), cisplatin plus doxorubicin, and doxorubicin plus ifosfamide, accounting for 30.83%, 21.05%, and 15.04%, respectively (Table 3). Only 7 patients (5.2%) received a second line of systemic therapy, including doxorubicin, a combination of gentamicin plus doxorubicin, and the doxorubicin ifosfamide dacarbazine (MAID) regimen. The mean total cumulative dose of doxorubicin was 250 + 142 mg/m², with a median of 225 mg/m2.
Patients’ baseline characteristics and associated comorbid conditions.

Sarcoma diagnoses among our patient cohort.
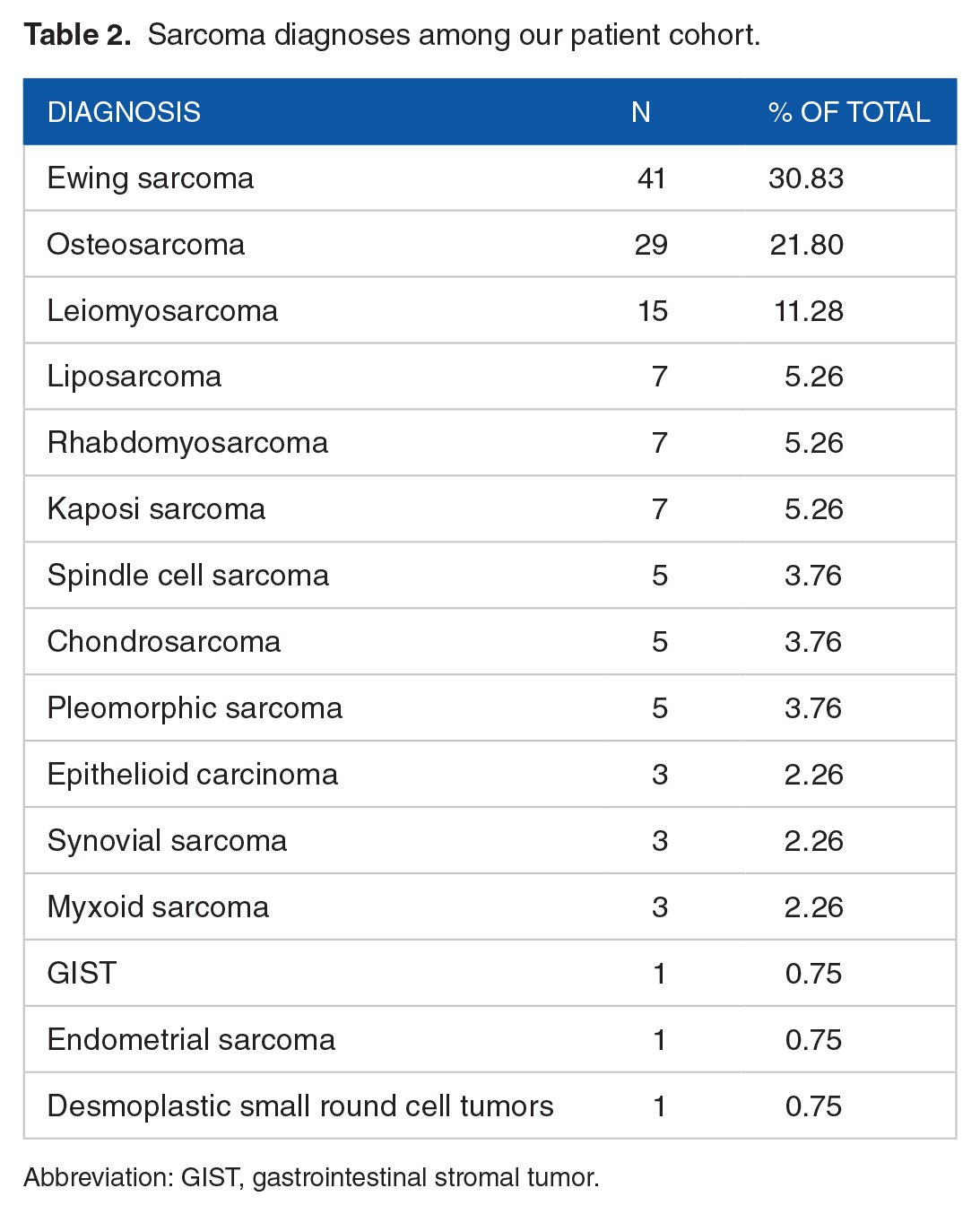
Abbreviation: GIST, gastrointestinal stromal tumor.
Types of chemotherapies/chemotherapy combinations given to our patient cohort.

Abbreviations: VAC, vincristine, adriamycin, and cyclophosphamide; IE, Ifosfamide, etoposide; VAI, vincristine, actinomycin D, and ifosfamide; MAP, methotrexate, doxorubicin, and cisplatin; MAID, adriamycin, ifosfamide, and dacarbazine.
Out of 133 patients, only 12 (9%) developed doxorubicin-associated cardiotoxicity (DAC). Table 4 shows the baseline characteristics of patients with cardiotoxicity. We found that female patients had a significantly higher risk of developing cardiotoxicity (P = .0089) compared with male patients. Cardiotoxicity was also more likely to occur in patients with a performance status of 4 (P = .0262). Interestingly, patients with a low troponin I level had a higher risk of developing cardiotoxicity (P = .0196). In addition, among patients with cardiotoxicity, there was a tendency for those without hypothyroidism to develop cardiotoxicity (P = .0643). Similarly, a tendency was observed in patients with low BNP levels (P = .0895). No significant difference was found in patients with a higher number of chemotherapy cycles, a total cumulative dose, and a history of radiation (P = .6899,.9031, and.2504).
Baseline characteristics of the study participants by cardiotoxicity.

Cardiotoxicity and Its Associated Mortality
Of the 133 patients, 44 had died, resulting in a mortality rate of 33%. The overall survival of deceased patients was 18 ± 19 months, with a median of 11 months. A summary of the deceased group’s characteristics is available in Table 5. The group with cardiotoxicity were found to be at a higher risk of mortality (P = .0271). Kaplan-Meier curve (Figure 1) shows the incidence of mortality among patients with cardiotoxicity and those without.
Adjusted multivariate Cox regression model for determining predictors of cumulative mortality.

Abbreviations: HR, hazard ratio; CI, confidence interval.
Model 1: Cardiotoxicity.
Model 2: Model 1 + age and sex.
Model 3: Model 2 + trop and hypothyroidism.
Model 4: Model 3 + malignancy grades (high, intermediate, and low), metastasis, and size.

This Kaplan-Meier graph displays the survival curves in all study patients who were treated with doxorubicin and developed cardiotoxicity (red line, n = 12) versus patients who did not (blue line, n = 121).
Discussion
Doxorubicin is a potent cytotoxic drug belonging to the anthracycline family. It is used for the treatment of various malignancies, including breast cancer, sarcoma, and lymphoma. 15 Anthracyclines act by inhibiting cancer cell proliferation through intercalation with DNA and by inhibiting topoisomerase II, which leads to DNA damage and apoptosis. 16 Doxorubicin exerts its cytotoxic effects by intercalating between base pairs in DNA, which inhibits DNA replication and transcription. Doxorubicin also forms complexes with topoisomerase II, which is responsible for cleaving and resealing DNA strands during replication and transcription. This results in the formation of doxorubicin-topoisomerase II-DNA complexes, which ultimately results in DNA damage and apoptosis. 17 Although doxorubicin is an effective chemotherapy drug, it can lead to various side effects, such as nausea, vomiting, alopecia, and myelosuppression. Hence, it is crucial to carefully evaluate the potential benefits and risks associated with the use of doxorubicin before administering it as a treatment. 18 Here, we aimed to study the association between doxorubicin and the incidence of cardiotoxicity.
Within our analysis, we observed that more than half of the individuals affected by sarcoma were men, which aligns with the findings of a Swiss study that reported 51.5% of cases were men. 19 However, in contrast to the study by Mans et al, 20 which found that approximately 52% of the affected patients were women. In this study, we found that 64% of our patients were aged 40 or younger, which differs from the Danish Sarcoma Database that shows a median age of 50 years. 21 There could be several reasons for this difference. First, we used our hospital’s digital database, which restricts us to patients treated at a single center from the years 2016 to 2022. Second, the geographical and age distribution in the Kingdom of Saudi Arabia could also be factors. It is worth noting that 80% of the Saudi population is under the age of 40, which could explain the high percentage of young patients with sarcoma in our study. 22
In this study, cardiotoxicity was observed in 12 out of 133 patients, which accounts for 9% of the patients. In this study, although 63% of our patients were male, we observed a significant association between cardiotoxicity and female patients (P = .0089). There are conflicting results regarding the cardiotoxicity associated with sex differences. A study conducted by Lipshultz et al examined the effects of doxorubicin therapy on children and adult patients (0.6-29 years) with a total of 150 patients. The findings of the investigation revealed a notable association between female sex and an elevated susceptibility to cardiotoxicity. The author contributed these findings for the increased left ventricle (LV) dimensions and reduced LV mass, which were more predominant in women. 23 In contrast to the aforementioned study, no significant differences were found between men and women regarding cardiotoxicity in adult-only patients. The Hrushesky et al study reported a higher ratio in female patients; however, Clements et al24,25 stated that the male sex was a strong independent risk factor for the development of cardiotoxicity.
It is also important to mention that the number of cycles of doxorubicin administration rarely exceeded 6 cycles, hence contributing to the low incidence of cardiotoxicity development in our cohort of patients. Cardiotoxicity affected only 12 out of 133 patients. This follows the established recommendations of considering discontinuing doxorubicin and closely monitoring cardiac function when approaching a cumulative dose of 400 to 450 mg/m2. The observed low percentage (9%) of affected patients with cardiotoxicity in our cohort can be attributed, in part, to the relatively low cumulative dose of doxorubicin administered. With a mean of 250 mg/m2 over an average of 6 cycles, our patients received a dosage regimen that is notably lower compared with other studies. This dose reduction strategy likely contributed to the mitigation of cardiotoxic effects associated with doxorubicin. Numerous studies have established a dose-dependent relationship between doxorubicin exposure and the risk of cardiotoxicity.26,27 Therefore, by administering a lower cumulative dose, we inadvertently minimized the overall cardiac exposure to the drug’s toxic effects. Consequently, the observed lower incidence of cardiotoxicity aligns with expectations based on dose-response relationships documented in the literature. This underscores the importance of dose optimization strategies in minimizing adverse cardiac outcomes in patients undergoing doxorubicin treatment.
Comparatively, a study conducted by Swain et al investigated a similar patient population and reported the incidence of cardiotoxicity. In their study, 32 (5%) out of 630 patients experienced cardiotoxic effects following treatment with doxorubicin. It is worth mentioning that 26% of patients who received a cumulative dose of 550 mg/m2 or more experienced cardiotoxicity. This difference in rates of cardiotoxicity could potentially be attributed to variations in treatment protocols and dosing strategies. 27 Furthermore, in our study, we adhered to established recommendations that suggest considering discontinuation of doxorubicin and closely monitoring cardiac function when approaching a cumulative dose of 400 to 450 mg/m2. By adhering to these guidelines, we aimed to minimize the risk of cardiotoxicity.
These contrasting findings highlight the importance of optimizing dosing strategies and adhering to guidelines in mitigating the risk of doxorubicin-induced cardiotoxicity. Our study’s approach, which involves limiting the number of cycles and cumulative dose of doxorubicin, as well as closely monitoring cardiac function, demonstrates a potential strategy for reducing the occurrence of cardiotoxic effects. However, further research is needed to validate these findings and identify the most effective dosing regimens that strike a balance between the potential benefits of doxorubicin and the risk of cardiotoxicity.
The ECOG performance status scale is a well-established prognostic tool used to evaluate the ability of cancer patients to perform daily activities and determine appropriate treatment strategies. The scale ranges from 0 to 4, with higher scores indicating more significant impairment. A score of 0 represents normal physical activity, while a score of 4 indicates complete immobility and confinement to bed. 28 Our study found a significant association between a higher ECOG score 4 and cardiotoxicity (P = .0262). This finding was expected finding given that a higher score indicates a worsening of the patient’s condition. This highlights the significance of evaluating a patient’s functional status using the ECOG score when evaluating treatment choices, especially in relation to cardiotoxicity.
The impact of cardiac mortality on cancer patients who underwent doxorubicin treatment is a crucial factor that cannot be overlooked. Our study revealed a strong correlation between cardiotoxicity and high mortality in these patients (P = .0271). It has been observed that the mortality rates of patients with DAC vary based on the severity of cardiac dysfunction. In a study involving 108 patients with DAC, the 5-year mortality rate was found to be 27% for those with asymptomatic left ventricular dysfunction, 48% for patients with symptomatic heart failure, and 60% for individuals requiring hospitalization due to severe heart failure. 29 Another study, which involved 61 patients with DAC, reported a 5-year mortality rate of 53% for those with severe left ventricular dysfunction, while those with mild-to-moderate dysfunction had a relatively lower 5-year mortality rate of 18%. 30 These studies highlight the significant detrimental effect of DAC on the overall prognosis of cancer patients. Hence, it is imperative to closely monitor patients undergoing doxorubicin treatment and take necessary measures to prevent or manage cardiotoxicity to improve their survival rates.
Cardiac troponin is a biomarker of myocardial injury. It is used for the diagnosis of myocardial infarction in patients presenting with chest pain. High troponin is also seen in patients with myocarditis and heart failure. Prior studies have shown that patients without troponin rise in the period of receiving chemotherapy are at low risk of developing cardiotoxicity.30,31 More recent studies with high-sensitivity troponin showed a dose-dependent increase in high-sensitivity troponin in patients receiving anthracycline, suggesting that high-sensitivity troponin may be used for the prediction of cardiotoxicity.32,33
In our study, lower troponin levels were associated with a higher prevalence of cardiotoxicity. This may be partly explained by the fact that troponin was not routinely measured in chemotherapy patients. Hence, most of the patients who had troponin measured were those with cardiotoxicity diagnosed by surveillance in whom the troponin may not be high.
A major limitation of our study is its retrospective design, which relies on digital medical record data from patients. These records are often subject to incomplete documentation and inconsistencies in reporting. The second limitation is the use of a single study center, which limits the generalizability of the findings, as the study population may not be representative of the broader population of patients receiving doxorubicin treatment. Furthermore, a notable limitation of this study is the small sample size, which may impact the statistical power and the ability to detect significant associations between doxorubicin treatment and cardiotoxicity. One of the key limitations of our study is the relatively low cumulative dose of doxorubicin administered to our patients compared with other studies. This factor may contribute to the observed lower incidence of cardiotoxicity in our patient population. However, it is important to note that the association between doxorubicin dose and cardiotoxicity is complex and multifactorial, with various other factors such as age, sex, pre-existing heart conditions, and concomitant medications potentially playing a role in determining the risk of cardiotoxicity. Therefore, while the lower cumulative dose in our study may provide 1 possible explanation for the reduced incidence of cardiotoxicity, it should not be considered the sole or primary reason for this observation. Finally, not all of our patients underwent a second echocardiogram following doxorubicin treatment. This inconsistency in follow-up assessments may lead to an underestimation of the true incidence of cardiotoxicity, as some cases may have gone undetected due to the absence of a second echocardiogram. To overcome these limitations, conducting a study with a larger and more diverse population would yield a more comprehensive understanding of the correlation between doxorubicin and cardiotoxicity. This would also help identify potential risk factors and protective measures that could be implemented in clinical practice.
Conclusions
Doxorubicin-associated cardiotoxicity is a well-known, serious, and potentially life-threatening condition that necessitates careful monitoring and management in high-risk patients. Based on our analysis of 133 patients, we found that cardiotoxicity was diagnosed in only 9% of the patients. Most of patients in our cohort were male (63%), with a median age of 30 years, and had a relatively lower cumulative dose of doxorubicin, which was 250 mg/m2. Interestingly, female patients, patients with an ECOG score of 4, and those with low troponin I levels were found to have a significantly higher risk of developing DAC. Further studies are needed to better understand the underlying mechanisms of DAC and to identify more effective prevention and treatment strategies. Our study, which is the first in our region to address cardiotoxicity in patients with sarcoma, contributes to the growing body of literature and provides valuable insights into the risk factors and clinical outcomes associated with it.
Footnotes
Acknowledgements
The authors thank the research and data management of Medical Oncology Department in King Abdullah Specialized Children Hospital, KAMC, for their valuable contribution in the data extraction.
Author Contributions
This article has been read and approved by all the authors. All authors met the requirements for authorship.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability Statement
The data collected/analyzed during this study can be accessed through the corresponding author on reasonable request.
Ethical Consideration and Consent
The Institutional Review Board (IRB) of King Abdullah International Medical Research Center, Ministry of National Guard—Health Affairs, Riyadh, Kingdom of Saudi Arabia (NRC32R/238/05) granted approval for the study. Informed consent was waived by the IRB as the study was retrospective in nature.