
Abstract
Background:
The burden of human immunodeficiency virus (HIV) in cervical cancer remains a major public health challenge in developing countries, like Togo. Precancerous lesions include all cellular abnormalities that have malignant potential that can develop into cancer. The objective of this study was to determine the prevalence and factors associated with precancerous cervical lesions in HIV-infected women in our context.
Methods:
A cross-sectional descriptive study was carried out from November 31, 2022, to January 31, 2023, in an HIV care center in Lomé (Non-Governmental Organization Espoir Vie Togo [NGO EVT] Grand-Lomé-Togo).
Results:
A total of 271 women were included with a mean age of 47.0 years and a standard deviation of 10.0 years, among whom 20.7% do not have any scholar education. Only 6.7% of them had previously performed cervical smear examinations. The prevalence of precancerous cervical lesions observed in people living with human immunodeficiency virus (PLHIV) was 11.4% with a 95% confidence interval (CI) of 5.0 to 15.4. Cytological abnormalities were marked by low-grade squamous intraepithelial lesion (LSIL) (5.1%), followed by the presence of atypical squamous cells of undetermined significance (ASCUS) (3.5%). A statistically significant association was found between parity and the presence of precancerous lesions (P = .014).
Conclusions:
In this study, more than 1 out of 10 women living with HIV had precancerous cervical lesions, and parity was the factor associated. The implementation of a systematic screening program for precancerous cervical lesions and human papillomavirus (HPV) infection integrated into HIV care is necessary for early treatment.
Background
Cervical cancer and the human immunodeficiency virus (HIV) present substantial public health challenges in developing nations, notably in Togo. 1 Human immunodeficiency virus–infected individuals face an elevated risk of human papillomavirus (HPV) infection. Although the type of HPV remains consistent whether an individual is infected with HIV or not, HIV-positive patients exhibit a heightened persistence of infections, particularly with oncogenic viral subtypes. 2 This persistent viral presence correlates with the development of dysplastic lesions, resulting in an increased incidence of epithelial cell abnormalities and cervical cancer (CC) in HIV-positive patients.2,3 Despite the potential for prevention through screening and vaccination, CC ranks as the second most common cancer in incidence and the leading cause of mortality among women, surpassing even breast cancer. 4 In 2020, there were approximately 604 000 new cases and 342 000 deaths attributed to CC worldwide, with nearly 90% recorded in low- and middle-income countries. 4 In Togo, the prevalence of CC in the general population according to the last study carried out in 2017 was estimated at 7.2%.5 Screening for precancerous lesions, especially through cytology, and subsequent treatment have demonstrated the potential to mitigate morbidity and mortality associated with CC, particularly in the context of HIV infection. 3 However, access to screening programs is markedly limited for women in developed countries. 6 Numerous studies across Africa have reported varying prevalence rates of precancerous cervical lesions among HIV-infected women, ranging from 4.4% to 42.4%.7-10 In Togo, the prevalence of precancerous lesions of the cervix in the general population was 8.6% in 2016.11 Nevertheless, there remains a notable absence of data on the prevalence of precancerous lesions specifically among the high-risk group of HIV-infected women in Togo. This study aims to determine the prevalence and identify factors associated with precancerous cervical lesions in HIV-infected women within our context.
Materials and Methods
Type and period of study
This was a cross-sectional descriptive study carried out from November 31, 2022, to January 31, 2023, a period of 3 months.
Setting and study population
The study was carried out in the Non-Governmental Organization Espoir Vie Togo (NGO EVT). The target population consisted of all patients living with HIV in Lomé. The source population consisted of patients living with HIV followed at the NGO EVT Grand Lomé. Women aged 18 and above, receiving antiretroviral treatment (ARVT), and who had undergone cervical smears in the 6 months preceding the survey were included. The participants in this study were selected using a nonprobability sampling method known as convenience. Thus, all women living with HIV seen in consultation in the said chosen center during the study period and who met the inclusion criteria were selected to participate in the study.
These were conventional smears, read separately by 2 pathologists, with diagnostic comparison for better interobservational reproducibility.
Sampling
The calculation of the number of subjects necessary was carried out with the following formula:
We made the following assumptions:
Variables studied
Variables included sociodemographic data (age, education, marital status, and profession), gynecological information (gestation, parity, cervical smear history, knowledge of CC risk, and gynecological follow-up), HIV-related details (age at diagnosis, virological profile, CD4 count, viral load, and treatment regimen), and cytopathological data.
Assessment and data collection
A standardized questionnaire, pretested for clarity and understanding, was administered to participants. Data on HIV-related clinical and therapeutic aspects were retrieved from medical records. Questionnaires were coded for anonymity.
Data processing and analysis tools
Completed questionnaires were checked for consistency and completeness. Data entry was done using EPI info 7 software and Microsoft Excel 2016. Descriptive statistics were employed, presenting results through tables and proportions for qualitative variables. Quantitative variables were expressed as means with standard deviations or medians with interquartile ranges. The chi-square, Fisher, and Wilcoxon tests were used for comparative analyses. Statistical significance was set at 0.05. R version 4.2.1 facilitated all analyses.
Results
Sociodemographic characteristics
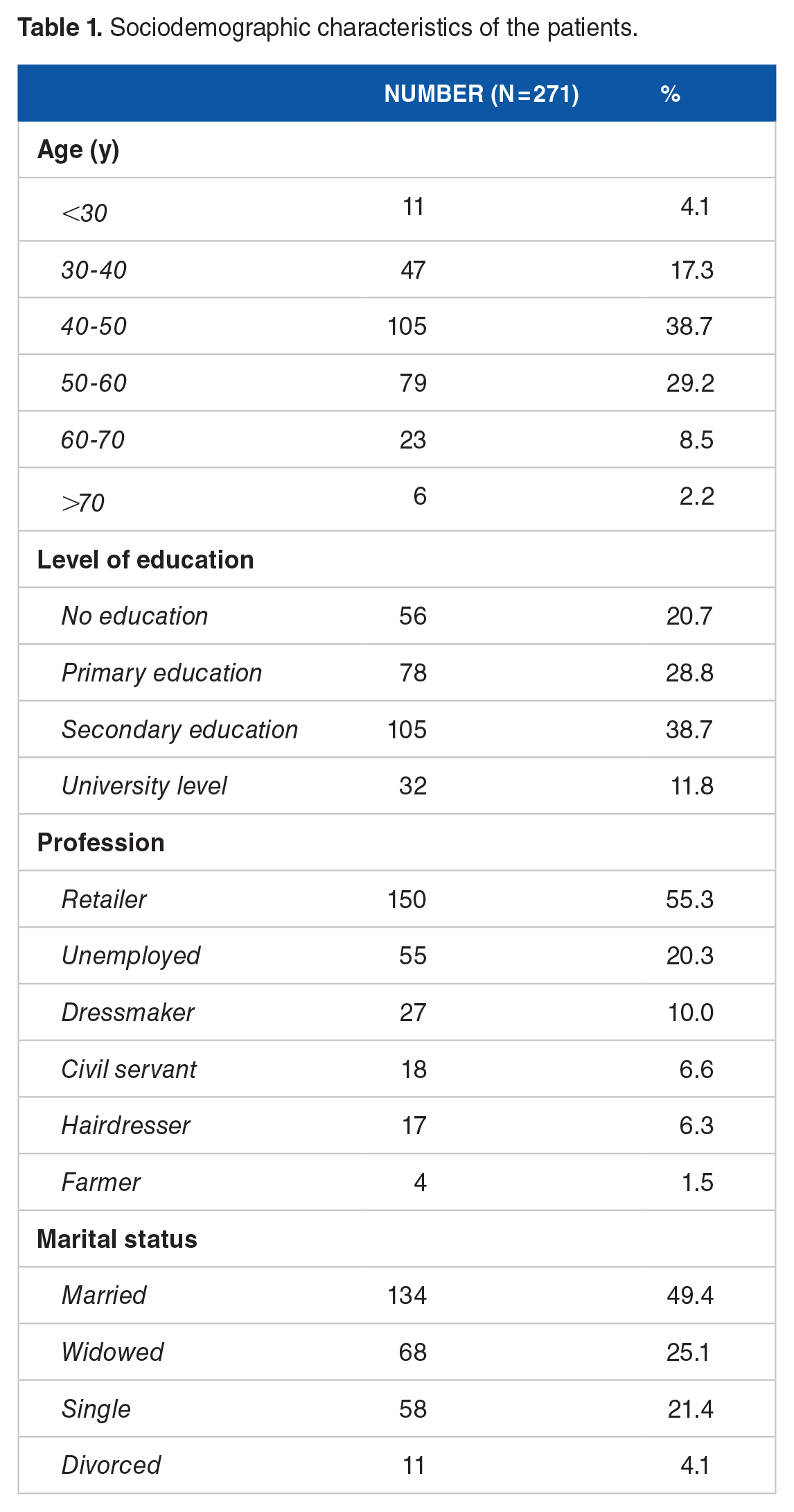
A total of 271 cervical smear cases were collected, with patients averaging 47 years of age, a standard deviation of 10.0 years, and age ranging from 22 to 93 years. Out of these, 105 patients (38.7%) were aged between 40 and 50 years. Concerning education, 105 patients (38.7%) had a secondary school level, while 56 (20.7%) were not in school. Marital status revealed 134 patients (49.4%) as married, and the employment distribution showed 150 resellers (55.3%) and 55 unemployed (20.3%) (Table 1).
Sociodemographic characteristics of the patients.
Gynecological data and Knowledge about the high risk of cervical cancer
The median gestational age among the respondents was 3 pregnancies with an interquartile range of 2 to 5 and extremes of 1 and 12 pregnancies. Among the respondents, 100 (36.9%) patients declared that they had multiple gestures. The median parity among the respondents was 2, with an interquartile range of 1 to 3 and extremes of 1 and 10. Sixty (22.1%) patients declared themselves multiparous. Seventeen (6.3%) patients had already taken at least 1 cervical smear. Among these patients, 17.7% claimed to have an abnormal smear; 76.5% of these smears were more than 3 years. Overall, 146 (53.9%) patients were aware of their high risk of developing CC. However, only 89 (32.8%) patients had regular gynecological follow-up (Table 2).
Summary of gynecological characteristics of patients.

Abbreviations: CC, cervical cancer; CUST, cervico-uterine smear test.
Data related to HIV infection
The median age of diagnosis of HIV infection was 13 years with an interquartile range of 6 to 16 years, a minimum of 1 year, and a maximum of 27 years. Ninety-three (34.3%) patients with age of 10 to 15 years had HIV infection. Seventy-seven (28.4%) patients had been diagnosed during a medical condition and 72 (26.6%) during routine screening. The median CD4 count among the respondents was 587 cells/mm 3 with an interquartile range of 412 to 785, a minimum of 41, and a maximum of 1820 cells/mm 3 . Among the respondents, 147 (54.3%) had a CD4 count between 500 and 1000 cells/mm 3 . Last HIV viral load results were available in 264 (97.4%) patients (Table 3). First-line ART was observed in 270 (99.6%) patients. The median duration of treatment was 13 years with an interquartile range of 7 to 17, a minimum of 1 year, and a maximum of 27 years (Table 3).
Summary of data relating to HIV infection.

Abbreviations:
Cytological data from cervical smears
The prevalence of precancerous lesions of the cervix was 11.4% with a 95% confidence interval (CI) of 5.0 to 15.4. Among the 271 patients who received smears, 94.5% were of satisfactory quality. The presence of cytological abnormalities concerned 11.4% of patients including atypical squamous cells cannot exclude high-grade squamous intraepithelial lesion (ASC-H) (0.4%), low-grade squamous intraepithelial lesion (LSIL) (5.1%), ASC (3.5%), and endocervical lesions (2.3%) (Table 4).
Summary of cytological data.

Abbreviations:
Factors associated with the occurrence of cervical anomalies
Bivariate analysis showed no significant association between sociodemographic or occupational characteristics and cytological abnormalities. Approximately 8.6% and 16.4% of nulliparous and primiparous women, respectively, had precancerous lesions. The frequency was 4.5% in pauciparous women compared with 17.5% in multiparous women, with statistically significant (P = .014). No significant association was observed between the presence of precancerous lesions and type of HIV infection, CD4 count, viral load, and type of ARVT (Tables 5 and 6).
Frequency of precancerous lesions/gynecological history.
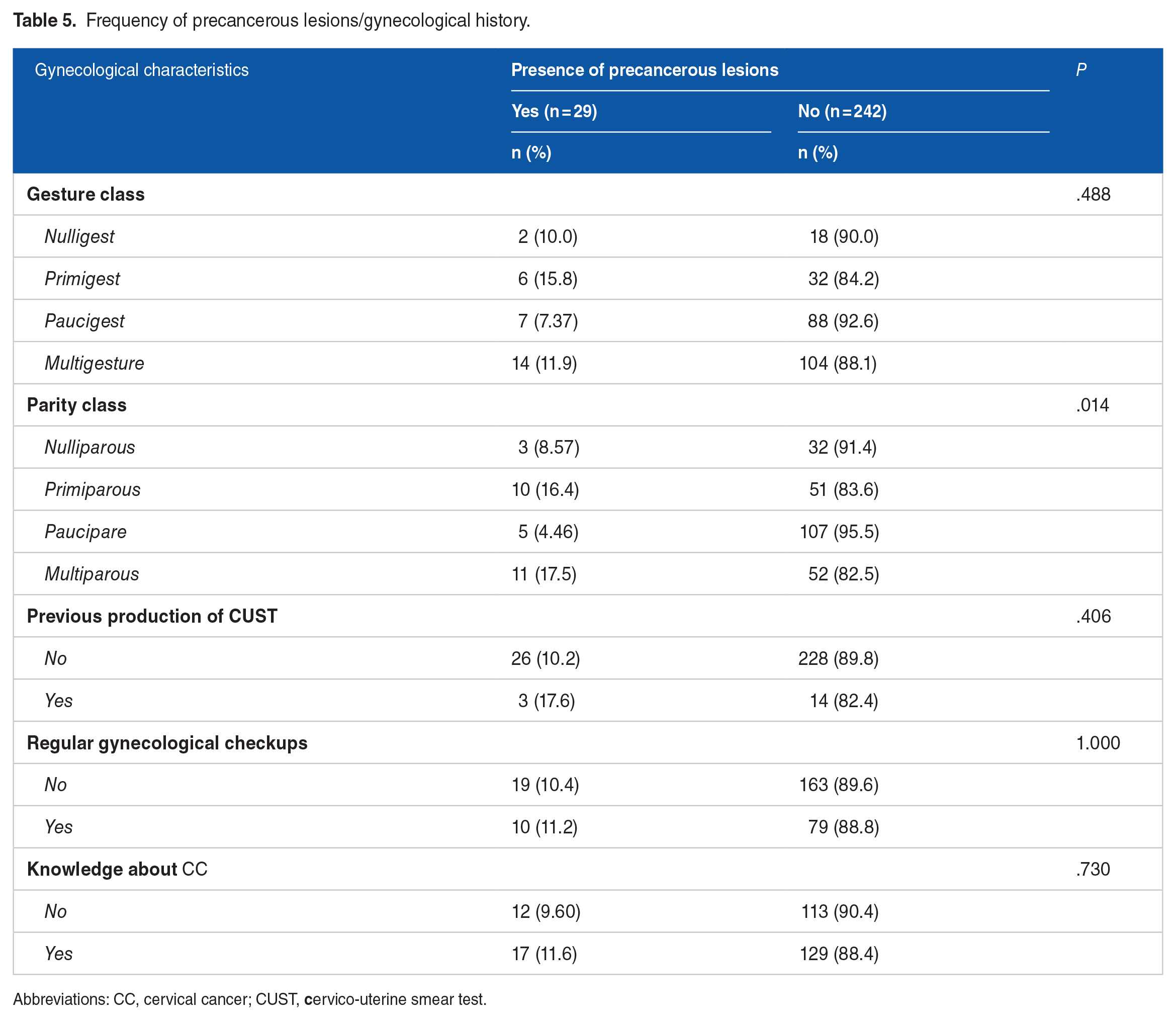
Abbreviations: CC, cervical cancer; CUST,
Frequency of precancerous lesions/characteristics linked to HIV infection.

Discussion
Cervical cancer is the second most common cancer in women in incidence and the first in mortality, even surpassing breast cancer. 4 In 2020, there were an estimated 604 000 new cases and 342 000 deaths from this cancer worldwide, nearly 90% of which were recorded in low- and middle-income countries. 4 The prevalence of CC in the general population of Togo was estimated at 7.2% in 2017. 5
The average age of our patients was 47 years, with a predominance in the 40 to 50 years age group. Fané et al and Aka et al reported mean ages of 41.6 and 39.3 years, respectively.14, 15 The emphasis on the 30 to 50 age range aligns with the target population for CC screening due to the heightened prevalence of cancerous lesions during this period. 16 Educational attainment emerges as a crucial social determinant of health, with more than half (50.5%) of our participants having attained a high level of education (at least equivalent to secondary school). This suggests receptivity to interventions that could substantially reduce factors predisposing individuals to precancerous lesions. Nearly half of our patients (49.4%) were married. Similar results were found by Moodley et al who identified 49.4% of married women. 17 This could be a link between regular sexual activity and the risk of developing precancerous lesions of the cervix in women living with HIV.
Multiparous women dominated our sample, constituting 23.2%. This aligns with findings by Fane et al, highlighting multiparity as a consistent risk factor for CC. 14 Multiparity remains a risk factor for CC according to the literature. Vaginal delivery, causing repeated trauma, induces architectural changes in the cervix leading to a dysplastic state. In addition, high parity (5 or more full-term pregnancies) appears to increase the risk of CC. 2 Only 6.3% of our patients had previously performed cervical smear examinations. Of these, 76.5% had a smear dating back more than 3 years on the date of the survey. These results are inconsistent with international recommendations regarding the frequency of performing the smear, namely a cervical smear every 3 years in the people living with human immunodeficiency virus (PLHIV) population. 18 Togo, like many other African countries, has not yet set up a national screening program, and screening is most often done opportunistically. The results of this study should, therefore, alert and motivate the implementation of interventions aimed at preventing CC in HIV-positive women.
The median age of HIV infection diagnosis was 13 years, with extremes of 1 and 27 years. Mortier et al found a median duration of follow-up for HIV seropositivity of 8 years, with extremes of 0 and 25 years. 19 Human immunodeficiency virus 1 predominated in almost all respondents (98.9%). Human immunodeficiency virus 1 remains the most predominant type of HIV in the world according to the literature.20, 21 CD4 count has been reported as an additional factor associated with the occurrence of precancerous cervical lesion. Since CD4 count is a vital indicator of immune status, a better immune system would help women protect against precancerous cervical lesions.22,23 Numerous studies have proven that there is a statistically significant association between CD4 count and precancerous lesions of the cervix in women living with HIV. A CD4 count >200 cells/mm3 remains an important factor in the prevention of precancerous cervical lesions.24,25 Indeed, according to the literature, HIV-positive women who have a CD4 count of less than 200 cells/mm3 are 1.75 times more likely to have cervical precancerous lesions than those who have a CD4 count of more than 200 cells/mm3-6 In our study, out of all 271 respondents, 258 had an accessible CD4 count, and only 4.8% of respondents had a CD4 count <200 cells/mm3. As for the HIV viral load, only 6 (2.3%) of the respondents had an unsuppressed viral load. This low proportion of unsuppressed viral load found could be attributable to the early initiation of antiretroviral treatment on discovery of HIV seropositivity and good follow-up of patients in said center. All the women were on ART, with a median duration of treatment of 13 years (IIQ = 7-17, min = 1 year, max = 27 years). The first line predominated at 99.6%. This is encouraging because ART started early would have a beneficial effect on the evolution of cervical lesions in HIV-positive women. 24 Studies conducted in Kenya and southern Ethiopia, and established the association between precancerous lesion of the cervix and the absence of ART in HIV-infected women.26, 27
However, unlike Kaposi sarcoma and some subtypes of non-Hodgkin lymphoma (NHL), no clear decline has been reported in the occurrence of infiltrative cervical carcinoma since the advent of ART. 28 The integration of effective CC screening programs among HIV-infected women and HPV vaccination of HIV-infected adolescent girls remains a priority in sub-Saharan Africa to prevent the occurrence of invasive cervical carcinoma.
Several studies have reported that women living with HIV appear to be a population particularly at risk of developing CC, particularly in West Africa.7,29 Indeed, there is an increased risk of HPV infection in patients infected with HIV; the type of HPV is the same in patients infected or not with HIV (in patients with the same risk criteria for HIV infection); but there is a higher rate of persistence of these infections in HIV-positive patients, especially in the case of an oncogenic viral subtype. The persistence of the virus is associated with the development of dysplastic lesions, and there is, therefore, a higher incidence of epithelial cell abnormalities and CC in HIV-positive patients. 2 The prevalence of precancerous cervical lesions was estimated at 11.4% in this study. Similar prevalences of precancerous cervical lesions in women living with HIV were found by Daniel et al and Belayneh et al, respectively, in 12.2% and 9.9%.30, 31 This relatively low prevalence in our study may be the result of viral load suppression, good monitoring of women living with HIV, and the increased use and availability of antiretroviral therapy, which have been reported to be associated at a reduced risk of developing precancerous lesions.32-35 The prevalence of precancerous cervical lesions observed in this study is significantly higher than that reported (8.6%) in the general Togolese population by Darré et al. 11
We observed a statistically significant correlation (P = .014) between the occurrence of precancerous cervical lesions and multiparity. Previous studies have also reported that multiparity is a risk factor for the occurrence of cervical precancerous lesions.36, 37 This association may be explained by the fact that multiple vaginal deliveries could lead to recurrent cervical lacerations increasing the risk of exposure to HPV during sexual activities and favoring the development of precancerous lesions.32, 33, 38 It would, therefore, be important to take multiparity into account when assessing the risk of precancerous lesions in women living with HIV. 39
Limitations
This study has several limitations that merit consideration. First, the research was confined to a singular health center in Lomé, limiting its generalizability to other populations of PLHIV beyond this center or in diverse health care settings. The outcomes derived from this study may not be universally applicable to the entire PLHIV population in Togo. In addition, the use of a convenience sampling method may introduce potential selection bias as participants were chosen based on their accessibility and availability for health care. The data collection process involved a questionnaire developed from a literature review and translated into various languages to enhance respondent understanding, thereby introducing the possibility of information bias. Participant responses may be influenced by comprehension errors linked to approximate translations of the questions or by a desire to provide socially acceptable answers. Human immunodeficiency virus–related clinical and therapeutic data were collected from medical records, which may be subject to reporting errors or filling errors or poor quality filling of records. The statistical analyses carried out in this study are mainly descriptive, which limit the possibility of identifying associations between the variables studied.
Conclusions
Cervical cancer is one of the leading cancers in women worldwide; most cases are reported in low- and middle-income countries like Togo. The widespread prevalence of HIV infection in sub-Saharan Africa exacerbates the risk of CC. This study found a relatively low, 11.4%, prevalence of cervical precancerous lesions in women living with HIV. However, this prevalence remains much higher than that found among women in the general population in Togo. Multiparous women living with HIV were identified by this study as having a higher risk of having a cervical uterine precancerous lesion. It would, therefore, be important to take multiparity into account when assessing the risk of precancerous lesions in women living with HIV.
Footnotes
Acknowledgements
The authors thank the team of NGO EVT Grand-Lomé-Togo.
Author Contributions
TD was responsible for the conception of the study; participated in the study design; undertook the field study; conducted the data collection, analysis, and interpretation; and wrote the article. TDj, KJOL, MKB, BD, and ASA were involved in the data collection, analysis, and interpretation, and wrote and finalized the article. DKE and BS are responsible for the overall scientific management of the study, analysis and interpretation, and the preparation of the final article. All authors have read and approved the final article for submission for publication.
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of data and materials
Extracted data are with the corresponding author and available under reasonable request.
Ethics approval and consent to participate
This study was approved by the “Comité de Bioéthique pour la Recherche en Santé (CBRS)” (Bioethics Committee for Health Research) from the Togo Ministry of Health, Ref No. 0101/2016/MS/CAB/DGS/DPLET/CBRS. Authorization from the director of the NGO EVT Grand Lomé was obtained before the start of the study. All patients and relatives of patients had received information on the purpose and procedures of this study and provided written and informed consent. The study has been carried out in accordance with relevant guidelines and regulations.