
Abstract
Background:
Numerous studies have shown that polymorphisms in the diabetes susceptibility gene, insulin-like growth factor 2mRNA–binding protein 2 (IGF2BP2), are associated with the occurrence and development of various malignant tumors; however, their correlation with the onset of diffuse large B-cell lymphoma (DLBCL) is still unknown. Therefore, this study aimed to explore whether IGF2BP2 polymorphisms increase the risk of developing DLBCL.
Methods:
This study included 295 DLBCL patients and 331 healthy individuals. Peripheral blood was collected, and polymerase chain reaction-ligase detection reaction (PCR-LDR) was used to detect IGF2BP2 gene polymorphisms. Logistic regression was used to assess the association between IGF2BP2 polymorphism and the risk of DLBCL, adjusted for age, sex, and body mass index (BMI). P < .05 indicated statistical significance.
Results:
The rs4402960 polymorphism in the IGF2BP2 gene was associated with the occurrence and development of DLBCL. After adjusting for age, sex, and BMI, GT (odd ratio [OR] = 1.54; 95% confidence interval [CI] = 1.08-2.19; P = .016), TT (OR = 2.00; 95% CI = 1.09-3.68; P = .026), and T genotype carrying (GT + TT) (OR = 1.62; 95% CI = 1.17-2.25; P = .004) significantly increased the risk of DLBCL. This study also found that the polymorphism rs1470579 was related to the development of DLBCL. After adjusting for age, sex, and BMI, AC (OR = 1.55; 95% CI = 1.11-2.17; P = .010), CC (OR = 2.18; 95% CI = 1.17-4.06; P = .014), and C genotype carrying (AC + CC) (OR = 1.64; 95% CI = 1.19-2.26; P = .002) significantly increased the risk of DLBCL.
Conclusions:
Our study found that polymorphism in the IGF2BP2 gene was associated with an increased risk of developing DLBCL.
Introduction
Diffuse large B-cell lymphoma (DLBCL) is the most common invasive lymphoma. Different subtypes of lymphoma have obvious heterogeneity in clinical manifestations and prognosis, and its main pathological features are the diffuse growth of abnormal lymphoid cells, destruction of normal structures, and invasive course of the disease.1,2 With the continuous updating of treatment options, the prognosis of DLBCL population is also improving, but about 40% of patients still indicate resistance to existing clinical treatment options, and show a poor prognosis. 3 Therefore, finding new drug targets and improving patient prognosis are urgent problems for clinical treatment. Current studies have shown that diabetes is an important risk factor for DLBCL, significantly shortening survival time and increasing the risk of death.4 -6 Insulin-like growth factor 2mRNA–binding protein 2 (IGF2BP2), which is located on chromosome 3 (3q27.2), is also associated with a higher risk of death. In combination with insulin-like growth factor 2mRNA, it can affect cell differentiation, proliferation, and epigenetic inheritance in various ways, playing a significant role in the development and occurrence of cancer. 7 As one of the diabetes susceptibility genes, IGF2BP2 is related to insulin resistance, lipid metabolism, and tumor development. 8 Numerous studies have found that polymorphisms in the IGF2BP2 gene are related to a higher risk of developing breast, colorectal, liver, non-small cell lung, oral, and pancreatic tumors.9 -14 However, associations between IGF2BP2 gene polymorphisms and DLBCL have not yet been reported. Further elucidating the pathogenesis of DLBCL is helpful to improve prognosis. Therefore, we aimed to investigate 4 nucleotide polymorphisms in IGF2BP2—rs4402960, rs1470579, rs9826022, and rs11705701—as well as their association with DLBCL risk.
Methods
Patients
In this study, 295 patients diagnosed with DLBCL at the Fourth Hospital of Hebei Medical University between January 2016 and December 2021 were selected as research subjects, and 331 healthy individuals from the physical examination center were selected as the control group. The inclusion criteria of the subjects were as follows: DLBCL confirmed by histological biopsy, immunohistochemical results, and complete case data. The exclusion criteria included other malignant tumors.
Clinical information
The following data were obtained from the clinical records: sex, age, height, weight, stage, international prognostic index (IPI), pathologic source, B symptoms, lactate dehydrogenase (LDH), β2 microglobulin, and immunohistochemistry.
The IPI was calculated according to the adverse factors: age >60 years old, disease stage III/IV, LDH higher than normal, Eastern Cooperative Oncology Group performance status score ⩾2 points, and number of extranodal involvement sites >1. The B symptoms were defined as unexplained fever, night sweats, and weight loss.
DNA extraction and genotyping
All subjects had an empty stomach overnight, and approximately 5 mL of elbow venous blood was extracted into a test tube containing an EDTA anticoagulant the morning of the next day. After the red blood cells were lysed, the whole blood genomic DNA was stored in the refrigerator at −80°C for extraction. The blood genome DNA extraction kit, Tiangen Biochemical Technology (Beijing) Co, Ltd/DP348/Beijing/China, was used in strict accordance with the instructions, and samples were stored at −20°C. The IGF2BP2 polymorphisms were detected using polymerase chain reaction-ligase detection reaction (PCR-LDR). Primers used for rs4402960 (G/T) were 5’-GTCTTGGAATCTAACAGCTCTAT-3’ (forward) and 5’-AAGGAATCTGCTTTGACCATT-3’ (reverse). The primers used for rs1470579 (A/C) were 5’-AAATGGCTACTGCAACTAAGA-3’ (forward) and 5’-TAGGCTTGTCTAT-GAGTGAGA-3’ (reverse). The primers used for rs9826022 (A/G) were 5’-CCTATGGCTT-GTTTCTACCTTT-3’ (forward) and 5’-TTATTCTCACTGCTGTGGTTG-3’ (reverse). The primers used for rs11705701 (G/A) were 5’-AGCCAGGAAATGAAATTCTACAG-3’ (forward) and 5’-GCGATCAAACCTTCAACTCTC-3’ (reverse).
Statistical analysis
The data were analyzed using SPSS (version 26.0; IBM SPSS Statistics, Armonk, NY, USA). The Hardy-Weinberg equilibrium test of the genotype distribution frequency was conducted using the chi-square test. The t-test or chi-square test was used to compare the differences in the distribution of IGF2BP2 genotypes between the case and control groups. Logistic regression analysis was used to assess the relationship between IGF2BP2 polymorphisms and the risk and clinicopathological parameters of DLBCL, with adjustments for age, sex, and body mass index (BMI). P < .05 showed statistical significance.
Results
Clinical analysis of patients with DLBCL and healthy controls
A total of 295 patients with DLBCL and 331 healthy controls were enrolled in this study. The age of the DLBCL group was 61.58 ± 13.25 years, and the age of the control group was 59.98 ± 12.53 years (Table 1). There was no statistical difference in age and sex between the DLBCL group and the control group (P > .05). The BMI of the DLBCL patients was 24.32 ± 4.30 kg/m2, much lower than that of the healthy control group (P = .008). In addition, there were 218 (73.9%) patients in the DLBCL group with stage III to IV disease, 164 (55.6%) patients with an IPI score of 3 to 5, 154 (52.2%) patients with B symptoms, 116 (39.3%) patients with germinal center B (GCB) cells, 145 (49.2%) patients with LDH levels higher than normal, and 135 (45.8%) patients with β2 microglobulin above the normal value.
Distribution of selected demographic variables and risk factors in DLBCL cases and controls.

Abbreviations: BMI, body mass index; DLBCL, diffuse large B-cell lymphoma; GCB, germinal center B cell; IPI, international prognostic index; LDH, lactate dehydrogenase.
Categorical variables were compared by the Pearson chi-square and represented by χ2 value; continuous variables were compared by analysis of variance and represented by F value.
Distribution of the insulin-like growth factor 2mRNA–binding protein 2 rs4402960 (G/T) allele and genotype frequencies in the diffuse large B-cell lymphoma and control groups
The frequency distribution of all genotypes in DLBCL group and the healthy control group was consistent with the Hardy-Weinberg equilibrium test, indicating the group population were representative (Table 2). The frequencies of GT (34.6%), TT (9.8%), and T genotypes (GT + TT) (44.4%) were higher than the frequencies of GT (27.8%), TT (6.0%), and T genotype (GT + TT) (33.8%) in healthy control cases. After adjusting for age, sex, and BMI, GT (odds ratio [OR] = 1.54; 95% CI = 1.08-2.19; P = .016), TT (OR = 2.0; 95% CI = 1.09-3.68; P = .026), and T genotype carriers (GT + TT) (OR = 1.62; 95% CI = 1.17-2.25; P = .004) showed a significantly increased risk of DLBCL.
Distribution of IGF2BP2 rs4402960 (G/T), rs1470579 (A/C), rs9826022 (A/G), and rs11705701 (G/A) allele and genotype frequencies in DLBCL cases and control cases.

Abbreviations: BMI, body mass index; DLBCL, diffuse large B-cell lymphoma; IGF2BP2, insulin-like growth factor 2mRNA–binding protein 2.
The odds ratio (OR) with their 95% CIs was estimated using logistic regression models.
Distribution of insulin-like growth factor 2mRNA–binding protein 2 rs1470579 (A/C) allele and genotype frequencies in the diffuse large B-cell lymphoma and control groups
The frequencies of AC (42.7%), CC (9.8%), and C genotypes (AC + CC) (52.5%) in DLBCL cases were higher than AC (34.7%), CC (5.8%) and C genotype (AC + CC) (40.5%) in the control cases (Table 2). After adjusting for age, sex, and BMI, AC (OR = 1.55; 95% CI = 1.11-2.17; P = .010), CC (OR = 2.18; 95% CI = 1.17-4.06; P = .014), and C genotype carriers (AC + CC) (OR = 1.64; 95% CI = 1.19-2.26; P = .002) showed a significantly increased risk of DLBCL.
Distribution of insulin-like growth factor 2mRNA–binding protein 2 rs9826022 (A/G) allele and genotype frequencies in the diffuse large B-cell lymphoma and control groups
The IGF2BP2 rs9826022 (A/G) gene polymorphism did not increase the risk of DLBCL (all P > .05) (Table 2).
Distribution of the insulin-like growth factor 2mRNA–binding protein 2 rs11705701 (G/A) allele and genotype frequencies in the diffuse large B-cell lymphoma and control groups
The IGF2BP2 rs11705701 (G/A) gene polymorphism did not increase the risk of DLBCL (all P > .05) (Table 2).
Association between the insulin-like growth factor 2mRNA–binding protein 2 rs4402960 (G/T) polymorphism and pathological parameters in patients with diffuse large B-cell lymphoma
The IGF2BP2 rs4402960 GT + TT genotype was associated with age >60 years, BMI <24 kg/m2, stage III to IV, and IPI scores of 3 to 5 (all P < .05) (Table 3). However, there were no significant differences in the sex, B symptoms, pathological diagnosis, LDH level, β2 microglobulin level, or related immunohistochemical (Ki67, BCL-2, BCL-6, and C-MYC) distributions (all P > .05).
Association between IGF2BP2 rs4402960 (G/T) polymorphism and pathological parameters of the DLBCL patients.

Abbreviations: BMI, body mass index; DLBCL, diffuse large B-cell lymphoma; GCB, germinal center B cell; IGF2BP2, insulin-like growth factor 2mRNA–binding protein 2; IPI, international prognostic index; LDH, lactate dehydrogenase.
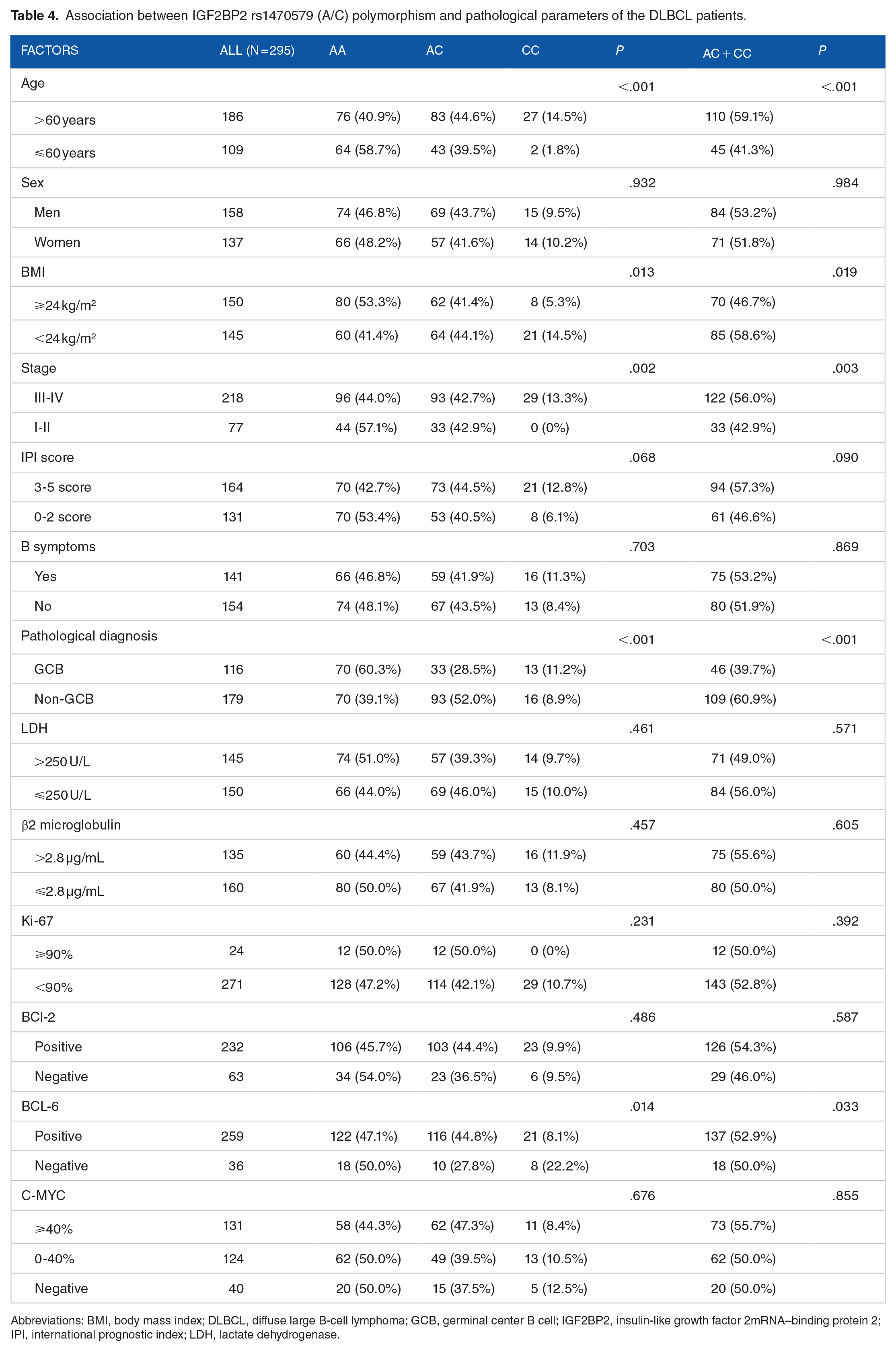
Association between the insulin-like growth factor 2mRNA–binding protein 2 rs1470579 (A/C) polymorphism and pathological parameters in patients with diffuse large B-cell lymphoma
The IGF2BP2 rs1470579 AC + CC genotype was related to age >60 years, BMI <24 kg/m2, stage III to IV, non-GCB, and BCL-6 positivity (all P < .05) (Table 4). In addition, there were no significant differences in sex, IPI, B symptoms, LDH level, β2 microglobulin level, Ki67, BCL-2, or C-MYC (all P > .05).
Association between IGF2BP2 rs1470579 (A/C) polymorphism and pathological parameters of the DLBCL patients.
Abbreviations: BMI, body mass index; DLBCL, diffuse large B-cell lymphoma; GCB, germinal center B cell; IGF2BP2, insulin-like growth factor 2mRNA–binding protein 2; IPI, international prognostic index; LDH, lactate dehydrogenase.
Discussion
The data in this study showed that the BMI in the DLBCL population was lower than that of healthy individuals, which may be related to weight loss after malignant tumors. More importantly, this study found that IGF2BP2 rs4402960 and rs1470579 polymorphisms were related to the development of DLBCL, and that their mutant bases, T and C, were both risk factors for the development of DLBCL. Previous studies have shown that IGF2BP2 polymorphisms are associated with a variety of malignancies,9 -14 which may include DLBCL, as evidenced by this study. Our study suggests that polymorphisms in IGF2BP2 may serve as influential factors for the early prediction of DLBCL events, thus providing relevant evidence for individualized treatment and prognosis.
In 2007, several studies reported that IGF2BP2 gene polymorphisms were significantly related to diabetes in European people.15,16 Subsequent studies in Chinese people have shown that IGF2BP2 rs4402960 polymorphism is associated with the occurrence of diabetes, establishing it as a susceptibility gene. 17 Ruchat et al 18 reported that the IGF2BP2 gene rs4402960 was related to glucose tolerance and insulin sensitivity, but not insulin secretion, potentially leading to the occurrence of diabetes by reducing insulin sensitivity. Another study involving 1731 individuals showed that IGF2BP2 overexpression was associated with poorer survival time in acute myelocytic leukemia (hazard ratio [HR] = 1.31; 95% CI = 1.16-1.49; P = .000), suggesting that IGF2BP2 can be used as a marker for predicting the prognosis of the disease. 19 In this study, we found that IGF2BP2 polymorphism increases the risk of DLBCL, which is similar to the conclusion of previous studies. In addition, patients with IGF2BP2 rs4402960 GT + TT and rs1470579 AC + CC tended to have a late clinical stage, indicating a poor prognosis. However, due to the short follow-up time, a relevant survival analysis could not be performed, which should be addressed in future work.
IGF2BP2 plays a role in promoting cancer cell survival, proliferation, and migration, but the underlying mechanisms by which it does so remain unclear.20,21 Studies have shown that a decrease in IGF2BP2 can downregulate NT5DC2 levels, thereby inhibiting cell proliferation of DLBCL by regulating the p53 signaling pathway. 22 In addition, cell experiments suggested that upregulated IGF2BP2 expression may promote the growth of pancreatic tumor cells by activating the PI3K/Akt signaling pathway. 14 Furthermore, the knockdown of the IGF2BP2 gene significantly reduced the invasion and migration of gastric cancer cells. 23 The IGF2BP2 polymorphisms rs1470579 and rs4402960, which are located in the intron region, may affect the risk of developing DLBCL through the post-transcriptional mechanism of IGF2BP2. However, the specific mechanism by which IGF2BP2 contributes to an increased risk of DLBCL remains unclear, and further studies are needed to explain the function of these IGF2BP2 polymorphisms.
One limitation of this study was that it was a single-center study, and the amount of data was relatively small. Further research with more data links is required to confirm these results.
Conclusions
In summary, our data suggest that the IGF2BP2 polymorphisms rs4402960 and rs1470579 are associated with an increased risk of DLBCL. However, further studies are required to confirm this hypothesis. If the above conclusions are confirmed, the corresponding intervention will greatly reduce the morbidity and mortality of the disease.
Footnotes
Author contributions
WZ and LL contributed to the study design. WLZ, QG, CH, LW, YW, and LF wrote the initial draft of the manuscript. All authors analyzed data and approved the final version of the manuscript.
Data availability statement
In accordance with the journal’s guidelines, we will provide our data for the reproducibility of this study in other centers if such is requested.
Ethics approval and consent to participate
The study was approved by the Medical Ethics Committee of the Fourth Hospital of Hebei Medical University (Hebei Tumor Hospital) (approval no. 2022KY384) and followed the principles of the Declaration of Helsinki. All subjects gave informed consent.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Department of Science and Technology of Hebei Province of China (nos 20221232 and 20230803).
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.