
Abstract
Background:
Nicotinamide N-methyltransferase (NNMT) and Dickkopf-1 (DKK1) play an important role in the development of breast cancer, and the purpose of this study was designed to examine the clinical and prognostic significance of NNMT and DKK1 in breast cancer.
Methods:
The GEPIA2 database was used to evaluate the expression and survival of NNMT mRNA and DKK1 mRNA of breast cancer. Then an immunohistochemical study was carried out on 374 cases of breast tissue to identify the protein expression and significance of NNMT and DKK1. Next, the prognostic significance of DKK1 in breast cancer was explored by COX and Kaplan-Meier models.
Results:
Protein NNMT expression was correlated with lymph node metastasis and histological grade (P < .05) while protein DKK1 expression was related to tumor size, pT stage, histological grade, and Ki-67 (P < .05). Protein DKK1 was related to disease-specific survival (DSS), and low DKK1 expression indicated a poor prognosis of breast cancer patients (P < .05). Combined expression of protein NNMT and protein DKK1 predicted different prognosis of DSS (P < .05).
Conclusions:
Nicotinamide N-methyltransferase and DKK1 were linked to breast cancer malignancy and invasion. Breast cancer patients with low DKK1 expression had a worse prognosis. Oncotypes of NNMT and DKK1 expression predicted patient outcomes.
Introduction
Breast cancer (BC) is the most common malignancy threatening women’s health worldwide. According to global cancer data released by the World Health Organization’s International Agency for Research on Cancer (IARC) in 2020, female BC had the highest incidence rate and the fifth highest fatality rate in the world in 2020. 1 In the same year, the BC data released by our National Cancer Center showed that BC was the number one cancer threatening women’s health in China. According to the data of previous years, the incidence of female BC increased year after year from 1988 to 2012 in China, 2 and the fatality rate climbed year after year from 1990 to 2015. 3 According to statistics, the global BC mortality rate exceeds 30% between 2012 and 2020.1,4 Breast cancer treatment currently relies heavily on surgery as the primary means of comprehensive treatment. 5 Early BC without metastasis can be adequately treated; however, advanced BC or those who were prone to recurrence or metastasis has a poor prognosis. 6 The main cause of death in cancer patients is uncontrolled invasion or metastasis of cancer cells that cannot be dealt with by conventional treatments. 7 Now we are still unable to accurately predict the prognosis of some postoperative patients due to the heterogeneity of BC. 8 Therefore, it is essential to seek new biomarkers to help predict the prognosis of postoperative BC patients and to guide clinicians in selecting appropriate postoperative management options for their patients.
Nicotinamide N-methyltransferase (NNMT) is a cytoplasmic enzyme that was previously implicated in vitamin B3 clearance, but subsequent the study has focused on its role in cancer. 9 Metabolic disorders and dysregulated methylation homeostasis are important links between NNMT and cancer development. 9 Nicotinamide N-methyltransferase expression that is abnormal can result in a number of malignancies, such as liver cancer, 10 nonmelanin skin cancer, 11 BC, 12 and so on. In recent years, researchers have focused on the importance of NNMT expression in cancer-associated fibroblasts (CAFs) in addition to epithelial cells. According to certain studies, CAFs may either promote or inhibit cancer growth.13,14 Eckert et al 15 found that NNMT is a major metabolic regulator of CAFs, and its overexpression in CAFs depletes large amounts of S-adenosylmethionine (SAM) and contributes to the reduction of histone methylation associated with genetic alterations in the tumor stroma, ultimately promoting the migration, accretion and metastasis of high-grade plasmacytoma cells in the ovary. Overexpression of the NNMT promotes invasion and metastasis in ovarian cancer, 15 gastric cancer, 16 and other cancers, which is indicative of a poor prognosis. Tumor-associated fibroblasts play an important role in the extracellular matrix of BC cells; however, its relationship with NNMT in BC has been less reported so far. 17 Kuo et al 18 constructed a 45-gene prognostic model for triple-negative BC by oligonucleotide microarray technology and validated it with data from a gene website, suggesting that the 45-gene prognostic model including NNMT is expected to be an effective marker for predicting recurrence of triple-negative BC. Wang et al 12 found that the expression level of NNMT was significantly higher in cancer tissues than in paracancerous tissue and benign hyperplastic breast tissues through a retrospective study of surgical specimens, and the protein expression level of NNMT was associated with the chemotherapy regimen of BC but not with clinicopathological characteristics such as age, estrogen receptor (ER), progesterone receptor (PR), human epidermal growth factor receptor 2 (HER2), Ki67, molecular typing, and tumor node metastasis (TNM) stage. So far, the clinical and prognostic significance of stromal NNMT in BC is not clear. Therefore, the clinicopathological features and prognostic value of NNMT expression in the epithelium and mesenchyme of BC deserve further investigation.
As a member of the Dickkopf gene family, DKK1 regulates both normal and cancerous cell proliferation,19,20 found in abundance in the placenta, liver, and bones.21,22 Cancer is frequently associated with aberrant protein spectrum expression. 23 As a secretory protein related to embryonic development, DKK1 has become a hot spot in cancer research in recent years. 24 Dickkopf-1 can not only act as a tumor suppressor in renal cell carcinoma, 25 melanoma, 26 colorectal cancer, 27 but also promote cancer development in pancreatic cancer, 28 non-small-cell lung cancer, 29 multiple myeloma, 30 and so on. Studies have shown that DKK1 is involved in the invasion or metastasis of BC through the WNT/β-catenin signaling pathway.31-35 However, Niu et al 36 proposed that DKK1 inhibits the invasion and metastasis of BC through β-catenin/MMP7 pathway. Zhuang et al 37 published an article on BC in Nature in 2017, which indicated that there is a significant organ-specific expression of DKK1 in BC that low expression of DKK1 promotes lung metastasis of BC through the atypical WNT/PCP-RAC1-JNK signaling pathway while high expression of DKK1 promotes bone metastasis of BC through the classical WNT signaling pathway. The authors indicated that the reason for the existence of this difference is related to the different tissue sources of DKK1 and differences in the tumor microenvironment. Zhou et al 38 indicated that there was a significant correlation between serum DKK1 expression level and TNM stage, histological grade, lymph node metastasis, ER and HER2 expression status and family history of BC in BC patients, but not with patient’s age, histological type, PR expression, radiotherapy, and menstrual status. However, Kasoha et al 39 had indicated that the significance of serum DKK1 expression may be influenced by the hormonal status of patients and drug therapy. The expression level and prognostic significance of DKK1 in BC tissues have been reported, but the drawback was that the sample size was too small.39,40 Although the mechanism of the action of DKK1 in BC remains unclear, but the relationship between its different expression levels and the clinicopathological features and prognosis of BC deserves further exploration through larger tissue samples.
All in all, both NNMT and DKK1 are potential prognostic markers for BC. At present, there is no combined study of the 2 biomarkers in BC. The purpose of this study was to examine the protein expression of NNMT and DKK1 in BC and to analyze their clinical value and prognostic significance in BC.
Materials and Methods
Database analysis of NNMT mRNA and DKK1 mRNA in BC
The Cancer Genome Atlas (TCGA) and Genotype-Tissue Expression (GTEx) are public databases for cancer research jointly established by the National Cancer Institute (NCI) and National Human Genome Research Institute (NHGRI). The Cancer Genome Atlas mainly provides data sets of tumor samples, while GTEx data come from sequencing of normal tissues during autopsies. 41 Expression Profiling Interactive Analysis 2 (GEPIA2) is an online analysis website based on TCGA and GTEx databases, which is efficient and easy to obtain. 42 In this study, data samples of BC projects in TCGA and GTEx databases were obtained from the official website of GEPIA2 (http://gepia2.cancer-pku.cn/) to analyze the expression of NNMT mRNA and DKK1 mRNA in normal breast and BC and their effect on the survival of BC patients. The total samples included 291 cases of normal breast and 1085 cases of BC.
Patients and tissue specimen
Breast tissue samples were collected from the second affiliated Hospital of Medical College of Shantou University (Shantou University, Shantou, China) between January 2014 and November 2018, including 24 cases of normal breast tissue, 20 cases of atypical hyperplasia and 330 cases of BC. Before the operation, none of the tissue samples received radiation, chemotherapy, or any other anticancer treatment. The morphological properties of hematoxylin and eosin (HE) staining were used to choose tissue wax blocks with distinctive regions for this investigation. The characteristics of the case (Table 1) included age, tumor size, clinical stage (according to the 8th edition of the American Joint Commission on Cancer staging Manual), pT stage, lymph node involvement, histological grade, vascular invasion, nerve bundle membrane, menopausal status, PR, ER, Ki-67, protein HER-2, GENE HER2, and molecular typing. All cases were diagnosed by professional pathologists Xingxing Wang and Haihua Huang. This study was approved by the Ethics Committee of the second affiliated Hospital of Shantou University Medical College. All the experimental specimens were signed by patients with written informed consent (2022-7).
Association of protein NNMT and protein DKK1 with the demographic and clinical variables of BC patients (N = 330).

Abbreviations: −/−, epithelial cells and CAFs were negative at the same time; −/+, (IHC HER2) interpretations of —or + for immunohistochemistry; −/+ (NNMT), epithelial cells were negative while CAFs were positive; +/−, epithelial cells were positive while CAFs were negative; +/+, epithelial cells and CAFs were both positive; BC, breast cancer; CAFs, tumor-associated fibroblasts; DKK1, Dickkopf-1; ER, estrogen receptor, HER2, human epidermal growth factor receptor 2; High, high expression; IHC, immunohistochemistry; Low, low expression; NNMT, nicotinamide N-methyltransferase; PR, progesterone receptor; pT, Pathological T-stage; Ki67, Nucleus proliferation-associated antigens.
Immunohistochemistry
The tissues arranged by tissue microarrays (TMAs) were characteristic regions selected by observing the morphological characteristics of HE sections, and each tissue was matched with the clinical information of the patient. Xylene and an ethanol-to-water gradient were used to dewax TMAs and paraffin slices. Before immersing the slides in the ethylenediaminetetraacetic acid (EDTA) of pH 9.0, it was heated to 80°C. Nicotinamide N-methyltransferase was repaired in 2 minutes with watertight high pressure, whereas DKK1 took just 40 minutes of heating at 100°C. The tissue sections were soaked with 3% H2O2 for 10 minutes to inhibit endogenous peroxidase. Preparing the first antibody working solution NNMT-antibody (#ab119758; 1:1600; Abcam, Cambridge, UK) and DKK1-antibody (#ab109416;1:600; Abcam, Cambridge, UK). Nicotinamide N-methyltransferase was incubated in a water bath at 37°C for 40 minutes, while DKK1 in a refrigerator at 4°C for 14 hours. The secondary-antibodies incubation slides of Elivision TM super HRP (mouse/rabbit) immunohistochemistry (IHC) kit (Kit-5930; Fuzhou Maxvision II, People’s Republic of China) were selected. Detailed information about antibodies can be found on the Human Protein Atlas website (https://www.proteinatlas.org/).
IHC staining of NNMT and DKK1
Staining results were made independently by 2 senior pathologists, and they did not know the specific information of the patients. The yellowish-brown granule in the cytoplasm of the epidermal cells and fibroblasts (CAFs) in the stroma of NNMT is the standard of positive cells. The total number of positive cells ⩽5% was defined as negative, while >5% defined as positive. According to the expression pattern of NNMT, they were divided into 4 subgroups: epithelial cells and CAFs were negative at the same time, epithelial cells were positive while CAFs were negative, epithelial cells were negative while CAFs were positive, epithelial cells and CAFs were both positive (expressed as −/−, +/−, −/+, and +/+). In this study, DKK1 staining was evenly distributed in epithelial cells. The yellowish-brown granules in the cytoplasm of the epidermal cells of DKK1 were taken as the positive standard. As DKK1 was expressed and stained uniformly in all breast tissues tested in this experiment, it was assessed according to the staining degree of epithelial cells in the tissues: weak positive was +; medium positive was ++; strong positive was +++. To facilitate statistical analysis, weak positive was classified as low expression, while medium positive and strong positive classified as high expression.
Follow-up and patient subgroup
Follow-up samples were chosen from consecutive instances between January 2014 and November 2018, and the cases were not picked based on subjective variables connected to the outcomes. Follow-up was carried out once a year. The total number of follow-up cases was 330. Disease-specific survival (DSS) time and disease-free survival (DFS) time were the endpoints. The time from surgery to death of BC patient (months) was defined as “disease-specific survival” (DSS), while the time from surgery to recurrence or metastasis was defined as “disease-free survival” (DFS).
Statistical analysis
The software GEPIA2 evaluated BC data from the TCGA and GTEx data sets, using the logarithmic rank sum test as its statistical approach. Then, descriptive summaries of the clinicopathological characteristics of the BC patients were generated, and the chi-square test and rank sum test were used to assess the association between NNMT, DKK1, and the clinicopathological characteristics of BC. Chi-square test was used to analyze the relationship between these two biomarkers and BC survival outcomes. Cox proportional hazard model was used to assess the risk factors influencing the BC prognosis. The possible prognostic factors were determined by univariate Cox proportional hazard model. Subsequently, a multivariate analysis was conducted on the significant prognostic factors (defined as P < .05 in univariate analysis). The Kaplan-Meier curve was drawn, and the survival results were analyzed by log-rank test. The relationship between NNMT and DKK1 expression was analyzed by Pearson’s correlation analysis and Pearson’s chi-square test. All statistical analysis was carried out by SPSS 25.0 software (IBM Corporation, Armonk, NY, USA). GraphPad Prism 9.0 was used for plotting.
Results
Database analysis of NNMT mRNA and DKK1 mRNA in BC
To investigate the importance of NNMT mRNA and DKK1 mRNA in BC, we consult the BC project’s public database. The level of NNMT mRNA expression was lower in BC than in normal breast (Figure 1A), and this difference was statistically significant (P < .05). Although DKK1 mRNA expression in BC was lower than in normal breast (Figure 1B), the difference was not statistically significant (P > .05). Kaplan-Meier curve showed (Figure 1C to F) that overall survival (OS) and DFS of BC patients were not affected by the expression of NNMT mRNA and DKK1 mRNA (P > .05).

Bioinformatics analysis of NNMT mRNA and DKK1 mRNA: (A) Expression level of NNMT from GEPIA2 of TCGA and GTEx BRCA samples. (B) Expression level of DKK1 from GEPIA2 of TCGA and GTEx BRCA samples. (C to F) Prognostic information for NNMT and DKK1.
Expression of NNMT and DKK1 in breast tissues
The expression of NNMT and DKK1 in 4 different pedigree breast tissues was depicted in the figure based on the results of this IHC experiment (Figure 2A and B). According to the histogram data, the distribution trend of NNMT expression patterns in breast tissues of 4 separate lineages was different (Supplemental Figure S1 A). In normal, atypical hyperplasia, carcinoma in situ, and invasive carcinoma tissues, the proportion of +/− grew gradually, but the proportion of −/+ decreased. The expression pattern of −/− was not identified in BC in situ, although it steadily diminished in the other 3 organizations. Normal tissues lacked +/+ expression, which was most prevalent in breast carcinoma in situ, followed by atypical hyperplasia, and least prevalent in invasive BC. The primary expression patterns of NNMT in breast carcinoma in situ and invasive BC were +/−, −/+, and +/+. In breast carcinoma in situ, +/− accounted for 24.0%, −/+ for 17.0%, and +/+ for 59.0%, but in invasive BC, the corresponding percentages were 18.0%, 43.8%, and 34.0%. The fraction of breast tissues with low DKK1 expression grew gradually in normal, atypical hyperplasia, carcinoma in situ, and invasive cancer, while the inverse was true for high DKK1 expression (Supplemental Figure S1 B). In other words, there was a significant tendency for NNMT to be elevated in BC compared to noncancerous tissue, especially in mesenchymal cells, whereas DKK1 was attenuated in BC.

Expression of protein NNMT and protein DKK1 in breast tissues: (A) staining of representative NNMT in breast tissues and (B) staining of representative DKK1 in breast tissues.
Associations between the 2 markers and the clinicopathological features of BC
In a subsequent investigation, the association between the protein levels of the 2 markers and the clinicopathological characteristics of BC patients was investigated. As indicated in Table 1, NNMT expression in BC was correlated with lymph node metastasis and histological grading (P < .05) but not with other clinical pathological parameters (P > .05). Dickkopf-1 expression was associated to tumor size, pT stage, histological grade, and Ki-67 (P < .05) but not to other clinicopathological characteristics (P > .05). The expression of Ki-67, ER, PR, and HER2 was shown in Figure 3.

Protein expression of ER, PR, HER2 and Ki-67 and fluorescence in situ hybridization (FISH) results of HER2. (A) HER2 was mainly expressed in the cell membrane of glandular epithelium, while ER, PR and Ki-67 were mainly expressed in the nucleus. (B) Positive and negative results of FISH of HER2 in breast cancer, Scale Unit: μm.
Cox regression model analysis
To assess the effect of DKK1 and NNMT on the survival outcome of BC patients, we selected DSS and DFS as end events. The findings of the chi-square test (Table 2) indicated that the expression of DKK1 in BC patients was associated to DSS (P < .05), but there was no significant difference in DFS (P > .05). The different groups of NNMT were not associated with DSS and DFS in BC patients (P > .05). Dickkopf-1 expression, Ki-67 index, pT stage, pN stage, age, tumor size, and adjuvant treatment were all linked with DSS of BC patients in univariate COX regression analysis (Table 3). It was found that BC patients with low DKK1 expression, Ki-67 > 30%, T3-T4 stage, N2-N3 stage, tumor > 4 cm, and no adjuvant chemotherapy had a shorter DSS (P < .05). Disease-free survival (DFS) of BC patients was linked to vascular tumor thrombus, Ki-67 expression, pT stage, pN stage, and tumor size. It was also revealed that patients with vascular tumor thrombus, Ki-67 > 30%, T3-T4 stage, N2-N3 stage, and mass > 4 cm had a lower DFS (P < .05). Further analysis of multivariate COX regression model showed that Ki-67 > 30%, N2-N3 and not receiving adjuvant chemotherapy were independent risk factors for DSS of BC, and their risk ratios (HR) were respectively 1.996 (95% confidence interval [CI] = 1.010-3.944; P = 0.047), 3.635 (CI = (1.900-6.955; P < .001) and 0.201 (CI = (0.088-0.460; P < .001). Ki-67 > 30% and N2-N3 stage were independent risk factors for DFS of BC, and their risk ratios (HR) were respectively 2.368 (CI = 1.295-2.333; P = .005) and1.850 (CI = 1.043-3.282; P = .035).
Correlation between protein DKK1 and protein NNMT expression in BC.

Abbreviations: −/−, epithelial cells and CAFs were negative at the same time; −/+, epithelial cells were negative while CAFs were positive; +/−, epithelial cells were positive while CAFs were negative; +/+, epithelial cells and CAFs were both positive; BC, breast cancer; CAFs, tumor-associated fibroblasts; DKK1, Dickkopf-1; High, high expression; Low, low expression; NNMT, nicotinamide N-methyltransferase.
P < .05.
Cox regression analysis of IHC (NNMT and DKK1 expression) and clinicopathological covariates of BC patients.
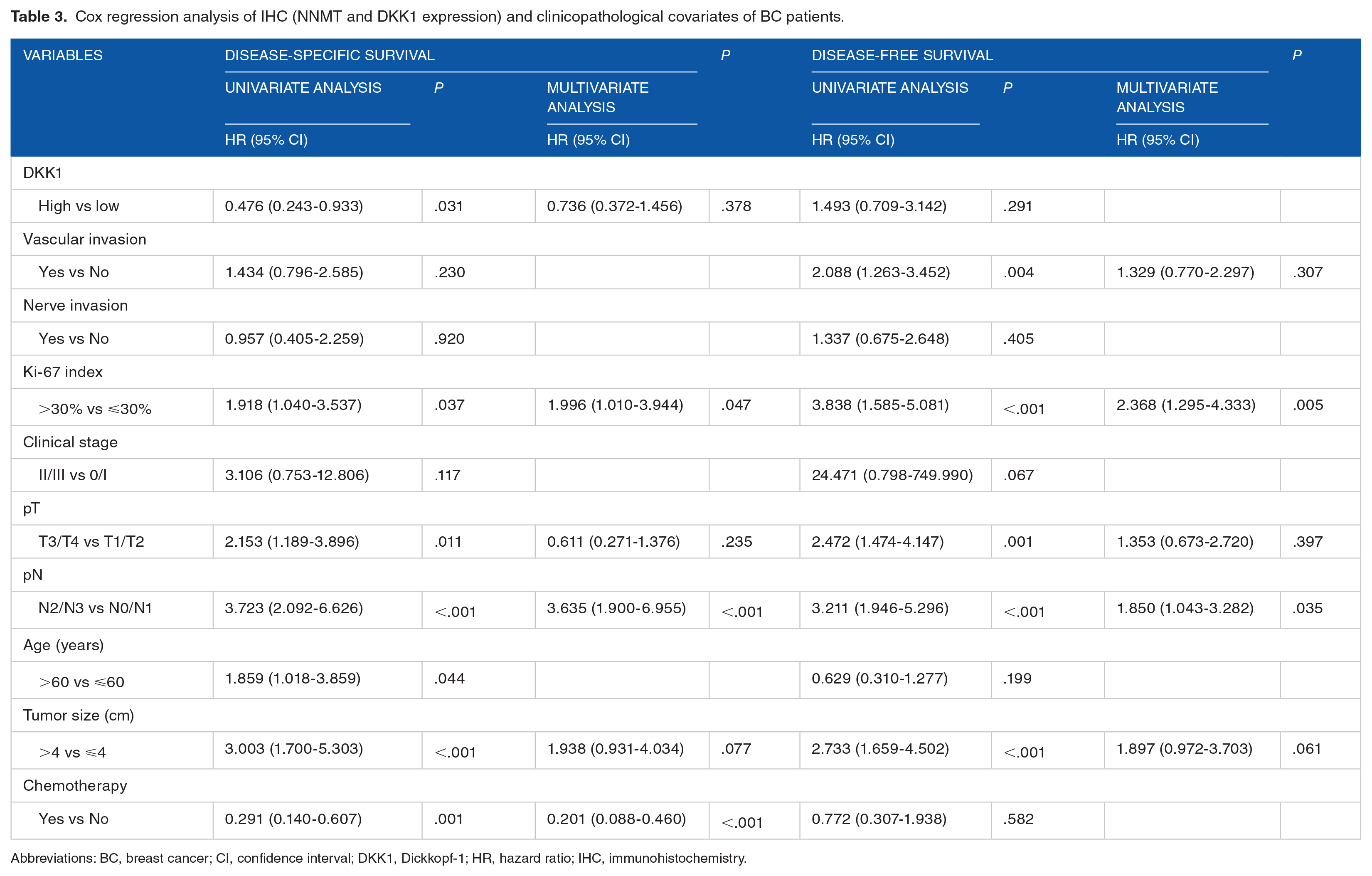
Abbreviations: BC, breast cancer; CI, confidence interval; DKK1, Dickkopf-1; HR, hazard ratio; IHC, immunohistochemistry.
Survival analysis of NNMT and DKK1
Survival analysis was conducted to further comprehend the association between the 2 biomarkers and the prognosis of BC patients. Kaplan-Meier curve (Figure 4A) showed that there was no significant difference in DSS or DFS among NNMT groups (P > .05). Disease-specific survival of BC patients with low DKK1 expression was dramatically shortened compared to those with high DKK1 expression (Figure 4B), and the difference was statistically significant (P < .05). In the DFS of BC patients, the survival curve of DKK1 was crossed, and there was no significant difference between the 2 groups (P > .05). The low expression of DKK1 at stage II and III of BC patients was significantly shorter than the high DKK1 expression of DSS (P < .05). For BC patients at stage 0 and I, there was no statistical difference in the effect of DKK1 expression on DSS (P > .05).

Survival analysis of protein NNMT and protein DKK1 in BC patients: (A) prognostic values of protein NNMT, (B) prognostic values of protein DKK1. P values were obtained by Kaplan-Meier analysis with log-rank test.
Effect of DKK1 expression on survival of BC patients with different molecular types
Further survival study was undertaken to understand the influence of DKK1 on the survival rate of distinct molecular types. Among BC patients with Luminal A or Luminal B type (Figure 5A), low DKK1 expression had lower cumulative survival rate with statistically significant difference (P < .05). For HER2+ and triple-negative BC patients, the survival rate of patients with low expression of DKK1 was lower than that with high expression, but there was no significant difference between the 2 groups (P > .05).
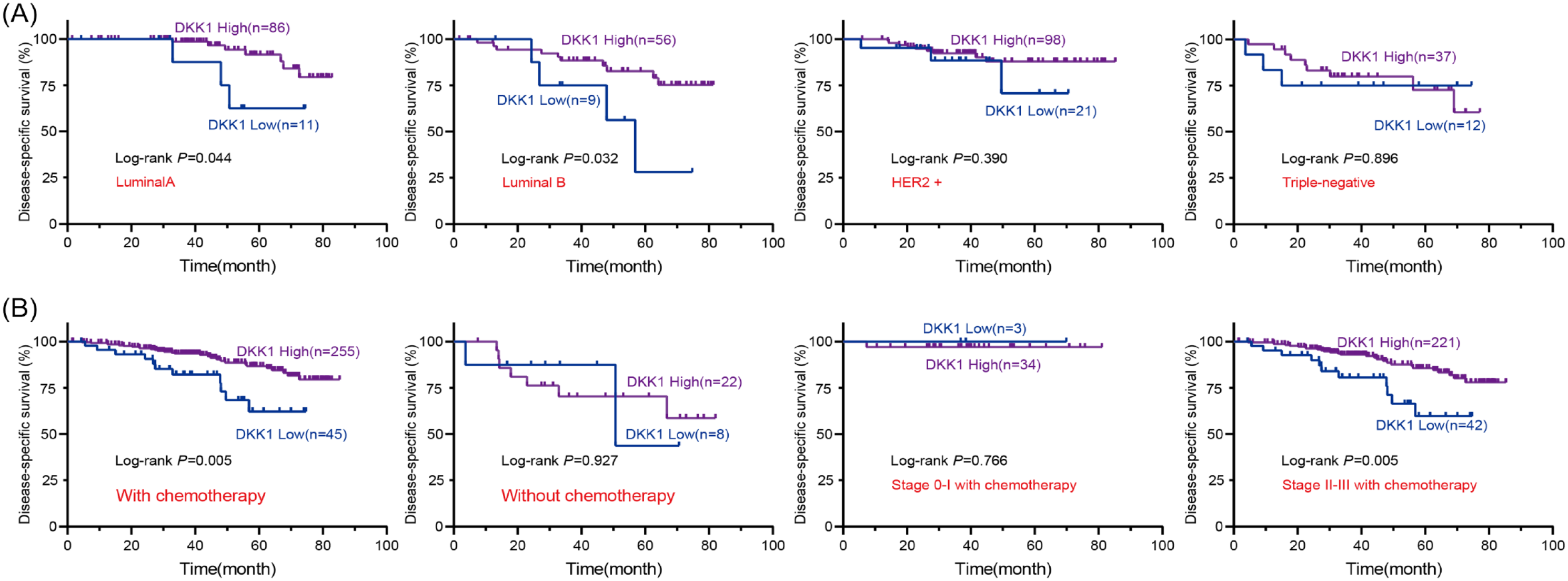
Survival analysis of protein DKK1 associated with different molecular typing and chemotherapy in BC patients. (A) Kaplan-Meier survival curves provided the DSS of Luminal A, Luminal B, HER2+ and triple-negative of BC patients, (B) Kaplan-Meier survival curves provided the DSS of chemotherapy or without chemotherapy in different stages. P value was analyzed by Kaplan-Meier analysis, using logarithmic rank sum test.
The relationship between DKK1 expression and therapeutic benefit of postoperative adjuvant chemotherapy
To evaluate the benefits of postoperative adjuvant chemotherapy in patients with BC, we recorded the chemotherapy information of BC patients during follow-up. As Kaplan-Meier curve showed (Figure 5B), BC patients who received adjuvant chemotherapy after operation, the cumulative survival rate of low DKK1expression was lower than that of high expression, and there was significant difference between the 2 groups (P < .05). For BC patients who did not receive adjuvant chemotherapy after surgery, there was no statistical difference in the influence of DKK1 on DSS (P > .05). We further analyzed the benefits of chemotherapy in BC patients at different stages, and the results suggested that BC patients who were of stage II and III after received postoperative adjuvant chemotherapy, low DKK1 expression had lower survival rate than the high (P < .05). For BC patients at stage 0 and I, the survival rate of high DKK1 expression was lower than the low after postoperative adjuvant chemotherapy, but there was no significant difference (P > .05).
The relationship between the expression of NNMT and DKK1 in BC
To investigate the relationship between NNMT and DKK1 in BC, we performed a combined analysis. According to the results of Pearson correlation analysis (Table 4), there was no relationship between the expression of NNMT and DKK1 in BC (P > .05). Kaplan-Meier curve showed (Figure 6) that the cumulative survival rate of BC patients with low expression of DKK1 and NNMT expression of −/+ was the lowest, followed by patients with low expression of DKK1 and NNMT expression of +/− ( P < .05). When the expression pattern of NNMT is −/−, the survival rate of BC patients was the highest regardless of the expression pattern of DKK1 (P < .05).
Correlation between protein NNMT and protein DKK1 expression in BC.

Abbreviations: −/−, epithelial cells and CAFs were negative at the same time; −/+, epithelial cells were negative while CAFs were positive; +/−, epithelial cells were positive while CAFs were negative; +/+, epithelial cells and CAFs were both positive; BC, breast cancer; CAFs, tumor-associated fibroblasts; DKK1, Dickkopf-1; High, high expression; Low, low expression; NNMT, nicotinamide N-methyltransferase.

Prognostic value of the combination of protein NNMT and protein DKK1 in BC patients: (A) Kaplan-Meier curve prediction of DSS with dual markers. (B) Kaplan-Meier curve prediction of DFS with dual markers.
Discussion
Owing to the significant heterogeneity of BC, it is important to comprehend its clinicopathologic characteristics to accurately predict its prognosis and determine the best course of treatment.5,8,43 Important pathologic characteristics associated with the prognosis and management of BC include age, histologic type, mass size, histologic grading, vascular invasion, nerve invasion, lymph node metastases, HER2 status, hormone receptor status, molecular typing, and so on.44-48 Recent advances in molecular techniques have made it possible for us to understand how clinicopathological characteristics in conjunction with potent molecular markers can help clarify the classification of BC and evaluate patient prognosis and treatment response. 49
In this study, the results suggested that there was a trend of elevated NNMT expression in BC compared with noncancerous tissues, especially in mesenchymal cells. In recent years, the expression of stromal NNMT in malignancies has received a lot of attention: scholars thought that stromal NNMT may be involved in the progression of malignancy.15,16,50 In previous research, NNMT was found to be elevated in BC.12,15 Our study was the first to examine the association between NNMT expression in the epithelium and mesenchyme with the clinical features and prognosis of BC patients. Lymph node metastasis and histological grade are essential components in the pathological report of BC 5 which have great value in guiding the treatment and predicting the prognosis of BC patients. Cui et al 51 hypothesized that NNMT expression was upregulated in esophageal squamous cell carcinoma and was linked to lymph node metastases. Apart from that, his study also found the invasive ability of esophageal squamous cell carcinoma cells was significantly reduced after the NNMT gene was knocked out. In this study, we found that NNMT was associated with lymph node metastasis and histological grade. This suggests that NNMT may be associated with the development of BC. In addition, Yu et al 52 discovered that NNMT can protect BC cells from oxidative stress-induced damage and inhibit autophagy. Their research also implied that targeted NNMT may offer promise as a future BC therapy option. Zhang et al 53 proposed that downregulation of NNMT through a mitochondria-mediated pathway induces apoptosis in BC cells. Some studies had shown that NNMT was a potential targeted drug and prognostic predictor for BC.18,53 Although its prognostic value may need to be further explored.
In this experiment, DKK1 was mainly expressed in the cytoplasm and we found a trend of diminished expression of protein DKK1 in invasive BC. In Sun’s study, they found that hormone-tolerant BC cell lines had higher DKK1 protein expression than hormone-dependent cell lines, while DKK1 mRNA expression was the same. In a retrospective study of surgical specimens, DKK1 expression was found to be associated with lymph node metastasis and TNM in BC and was an independent risk factor for recurrence-free survival in BC, and survival analysis also suggested a better prognosis in DKK1-negative patients. 40 However, the role of DKK1 in BC is very complex, and its specific mechanism of action has not yet been clarified. It can not only promote the development of cancer but also act as a tumor suppressor. The histological type of the tumor, hormonal condition, medication therapy, and other factors may all have an impact on the differential expression of DKK1 in BC.39,54 Since it is a secreted glycoprotein, variations in the protein’s secondary modifications or variations in the relative abundance of its ligands and their secondary modifications can affect the protein’s activity. Related research revealed that different cell subtypes or tissue sources (mesenchymal or epithelial) determine how DKK1 affects various cancer stages or types and that the mechanism may be influenced differently by the WNT signaling pathway in an autocrine or paracrine manner, promoting or inhibiting the growth of cancer.37,55,56 Some studies have shown that platelets, which are associated with tumorigenesis, metastasis and immune escape phase, are an important source of DKK1.57,58 In addition, the regulation of DKK1 on the activity of immune cells (lymphocytes, macrophages, dendritic cells, etc.) surrounding the tumor affects the tumor microenvironment, which in turn affects the development of tumor. 21 Most studies have concluded that DKK1 can be an effective marker for early screening of cancer.59,60 Hall et al 61 found that DKK1 expression levels were significantly higher in primary prostate cancer foci and bone metastases than in normal prostate tissue, while its expression levels were weaker in bone metastases than in primary foci. Regarding why DKK1 differs in different stages of tumorigenesis, the authors suggested that this might be related to the regulatory mechanism of the classical WNT signaling pathway, but its exact mechanism of action is still unclear. In our study, we found that the expression of protein DKK1 was related to tumor size, pT stage, histological grade, and Ki-67. These factors are important in the development of tumors, suggesting that the expression level of DKK1 in BC may influence the development of BC. In addition, survival analysis of follow-up data showed that low DKK1 expression predicted poor prognosis in BC patients and that clinical stage and molecular typing influenced the predictive effect of DKK1. A growing number of studies have shown that DKK1 is an effective marker for early screening of cancer.62-64 Our findings suggested that DKK1 was a good predictor for patients with stage II and III or Luminal A or B. The prognosis of BC is difficult to predict accurately, and DKK1 combined with clinical staging and molecular typing will be more helpful to improve the classification of BC. This provides a new perspective for individualized treatment and prognosis assessment. In addition, we found that DKK1 had a good predictive value for the benefit of chemotherapy in BC. Studies have shown that adjuvant chemotherapy has effectively improved the survival rate of BC patients in recent decades.65,66 It is worth noting that with the increasing understanding of adjuvant chemotherapy, researchers are increasingly concerned about the serious consequences of chemotherapy, such as secondary bone marrow tumors, cardiotoxicity, and nerve damage. 67 Adjuvant systemic therapy can effectively reduce the risk of recurrence and metastasis in patients with BC, but we are still unable to predict its benefits accurately now. 68 From our results, DKK1 is expected to be a predictive marker for the benefit of chemotherapy in BC. However, the limitation of our study was lack of data support from molecular biology experiments.
It has been reported that NNMT and DKK1 play an important role in BC,18,39,53 but no scholar has paid attention to their co-role in BC. From above, we found that NNMT and DKK1 were associated with the invasion and malignant degree of BC and low expression of DKK1 predicted poorer prognosis. Therefore, we explored their value in the prognosis of BC through the combined action of NNMT and DKK1 at the protein level. Consequently, we found BC survival was affected by the combination of NNMT and DKK1 expression patterns. Zhang et al 53 demonstrated that inhibiting NNMT reduced tumorigenicity in mice, indicating that NNMT is a promising therapeutic target for BC. Niu et al 36 highlighted that DKK1 is anticipated to be a potential alternative therapy for the prevention and treatment of BC. Our study offers a novel strategy for combining NNMT with DKK1 targeting in BC therapy. However, their exact effect on BC remains to be further studied.
This study’s shortcoming was the absence of more in-depth mechanistic studies. Further analysis of the sample size’s predictive relevance was hampered by the sample size’s relative inadequacy, particularly after NNMT was separated into 4 groups.
Conclusions
In conclusion, our findings suggested that the expression of NNMT and DKK1 in BC was of great significance. It was obvious that DKK1 had a good predictive value for the prognosis of BC, especially for different stages, different molecular typing, and the benefit of chemotherapy for patients.
Supplemental Material
sj-docx-1-onc-10.1177_11795549231168073 – Supplemental material for Correlation of NNMT and DKK1 Protein Expression With Clinicopathological Characteristics and Prognosis of Breast Cancer
Supplemental material, sj-docx-1-onc-10.1177_11795549231168073 for Correlation of NNMT and DKK1 Protein Expression With Clinicopathological Characteristics and Prognosis of Breast Cancer by Tairong Liang, Xiuqian Wu, Lan Wang, Tiantian Song, Peishan Wu, Yongdong Niu and Haihua Huang in Clinical Medicine Insights: Oncology
Supplemental Material
sj-png-1-onc-10.1177_11795549231168073 – Supplemental material for Correlation of NNMT and DKK1 Protein Expression With Clinicopathological Characteristics and Prognosis of Breast Cancer
Supplemental material, sj-png-1-onc-10.1177_11795549231168073 for Correlation of NNMT and DKK1 Protein Expression With Clinicopathological Characteristics and Prognosis of Breast Cancer by Tairong Liang, Xiuqian Wu, Lan Wang, Tiantian Song, Peishan Wu, Yongdong Niu and Haihua Huang in Clinical Medicine Insights: Oncology
Footnotes
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors thank all the people who have helped us and the foundations of the National Natural Science Foundation of China (grant no. 81772972), Natural Science Foundation of Guangdong Province (grant no. 2021A1515010776), Technology Planning Project of Guangdong Province Special Project Fund (grant no. 210728166902052), Shantou Science and Technology Project (grant no. 210610116490674), and Guangdong Medical Research Foundation (grant no. B2018050).
Author Contributions
YN and HH conceived and designed this project; TL and LW performed the experiments; TS and PW performed the experiments and the analyses; TL was responsible for writing the article; and HH and XW oversaw the writing of the manuscript. All authors read and approved the final manuscript.
Ethics approval and consent to participate
This study was approved by the Ethics Committee of the second affiliated Hospital of Shantou University Medical College. All the experimental specimens were signed by patients with written informed consent (2022-7).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.