
Abstract
Background:
Alpha-fetoprotein-positive gastric cancer (AFPGC) is a subtype of gastric cancer that is rare in clinical practice and extremely malignant. Malignant tumors are often associated with hemorrhage, thrombosis, and even disseminated intravascular coagulation (DIC). The D-dimer test is used as a sensitive index in the diagnosis of DIC and fresh thrombosis in malignant tumors. Therefore, this study aims to investigate the relationship between D-dimer values and the clinical characteristics and prognosis of patients with serum AFPGC (AFP ⩾ 15 μg/L) patients.
Methods:
Overall, 120 healthy subjects and 120 AFP-negative gastric cancer (AFP < 15μg/L) patients from May 2017 to July 2018 at the Shanxi Cancer Hospital served as the control group in this retrospective cohort study. Additionally, 120 patients with pretreatment advanced serum AFP were chosen to analyze clinicopathologic features and factors that affect prognosis. The predictor was the D-dimer, and the outcome variable was overall survival (OS). Other variables included age, sex, tumor site, T-stage, distant metastasis, and preoperative serum tumor biomarkers. Differences in OS rate were analyzed by GraphPad Prism 9.2.0.332. The Cox regression model was used for univariate and multivariate analysis.
Results:
In comparison to AFP-negative gastric cancer, we discovered that D-dimer had a meaningfully higher presentation in patients with AFPGC (P < .001). Based on D-dimer median levels, the AFPGC patients were divided into two groups, including 39 patients with low D-dimer (<1000 ng/mL) and 81 patients with high D-dimer (⩾1000 ng/mL). The variables, including T-stage, distant metastasis, and expression of HER2, were associated with the value of D-dimer. The D-dimer levels were weakly related to the levels of tumor markers. The differences in AFPGC patients, with an OS rate of 30.76% for patients with low D-dimer (<1000) and 12.30% with high D-dimer (⩾1000; P = .0027), were statistically significant. Cox multivariate analysis of various parameters indicated that T-stage, distant metastasis, vascular embolism, level of D-dimer, and tumor biomarkers of AFP were independent risk factors for survival.
Conclusion:
Serum D-dimer levels may be a valuable indicator for predicting AFPGC metastasis and progression.
Introduction
Alpha-fetoprotein is a type of globulin that is secreted by the gastrointestinal tract, yolk sac, and liver of the fetus, and is also secreted in hepatoma cells and yolk sac tumor cells. 1 However, the serum alpha-fetoprotein levels in patients with primary gastric cancer (GC) sometimes increase. 2 Therefore, GC with high alpha-fetoprotein levels is known as alpha-fetoprotein-positive gastric cancer(AFPGC). According to statistics, AFPGC accounts for 2.7% to 8% of GC and is considered one of the most malignant subtypes. 3 D-dimer is a stable terminal degradation product that is produced by fibrin monomer cross-linked by activator XIII, and then hydrolyzed by plasmin.4,5 Malignant tumors were characterized by a high level of the fibrinolytic enzyme, which induces fibrinolysis and increases plasma D-dimer. Furthermore, a high level of D-dimer can accelerate the appearance of venous thromboembolism (VTE) in cancer patients. 6 Many studies have demonstrated that a high D-dimer can promote the rapid development of malignant tumors, 7 including colorectal cancer, 8 GC, 9 and liver cancer. 10 Tumor cells could stimulate the release of procoagulant substances, which activate the exogenous coagulation system to cause clotting abnormalities. At the same time, the plasminogen activator is activated and increased, and finally plasmin is locally produced, which can directly degrade the extracellular matrix, making tumor cells aggressive. As a very rare GC, AFPGC has both adenocarcinoma areas and liver differentiation areas. Some patients lose their surgical opportunity at the time of diagnosis. Even if radical surgery was performed, the probability of recurrence and metastasis was higher compared with patients with AFP-negative gastric adenocarcinoma. The standardized and consistent treatment of patients has not been previously addressed. To date, there are only a few studies that have reported the effect of D-dimer on AFPGC. Our study aims to investigate the relationship between the levels of D-dimer and the clinicopathology and prognosis of AFPGC.
Materials and methods
Patients
Overall, 120 AFP-negative GCs and 120 gastric patients with preoperative elevated serum AFP who underwent radical surgery in the Shanxi Cancer Hospital from May 2017 to July 2018 were evaluated in our study. However, 120 healthy people served as the control group. Epidemiological and clinical data were collected from patients’ medical records, including age and sex at diagnosis, tumor site, T-stage, and distant metastasis. Preoperative conventional serum tumor biomarkers were tested, including AFP (μg/L), CEA (μg/L), CA19-9 (U/mL), CA242 (U/mL), and CA72-4 (U/mL), across all inpatients.
The inclusion criteria were as follows:
Pathological confirmation of adenocarcinoma;
All patients had not received any treatment, including neoadjuvant chemotherapy and any antitumor therapy prior to the operation;
The levels of AFP and D-dimer in all the patients were measured prior to the operation.
The exclusion criteria were as follows:
Pathologically undiagnosed patients;
Patients with more than 50% of information missing.
Study variables
The initial predictor variable of our study was the pretreatment D-dimer value. Based on the median value, the patients were divided into two subgroups based on the optimal cut-off value of 1000 ng/mL.
Follow-up
Patient follow-up data were obtained through reviews of hospital records. Patients were observed until July 31, 2021. The overall survival (OS) was the interval between the dates of initial hospital admission and either the time of last follow-up or death due to AFPGC. Censoring occurred for patients who were still alive or deceased for other reasons at follow-up.
Statistical analysis
The collected data were processed using GraphPad Prism 9.2.0.332. Statistically significant differences among patients with AFP-negative GC, gastric patients with preoperative elevated serum AFP, and healthy people were determined using an unpaired t‑test. Correlation analysis was performed for the analysis and the relationships between peripheral biomarkers and D-dimer. Associations of D-dimer levels with clinicopathological characteristics were presented as counts and percentages, and were analyzed using a chi-square test. Survival curves were calculated using the Kaplan–Meier method. Univariate survival analyses and variables with statistical significance were entered into the Cox proportional hazards regression model analysis. Finally, Cox proportional hazards regression model analysis was used to identify the factors associated with OS. A P value of less than .05 was considered to be statistically significant. SPSS software (V.22.0) for Windows was used for all statistical analyses.
Ethical considerations
Since all the data from this study came from hospital records, there was no direct contact with patients’ families. The study was granted exemption from the ethical review committee of Shanxi Province Cancer Hospital (Ethics No. 202208).
Results
Patient characteristics
The results demonstrated that D-dimer levels were significantly higher among patients with AFP-negative GC (AFP < 15; P < .05) and AFPGC (AFP ⩾ 15; P < .0001), compared with healthy humans. Simultaneously, D-dimer was expressed to a significantly higher level in AFPGC (P < .001) compared with AFP-negative GC (Figure 1A). The results demonstrated that the D-dimer was an essential indicator in the development of AFPGC.
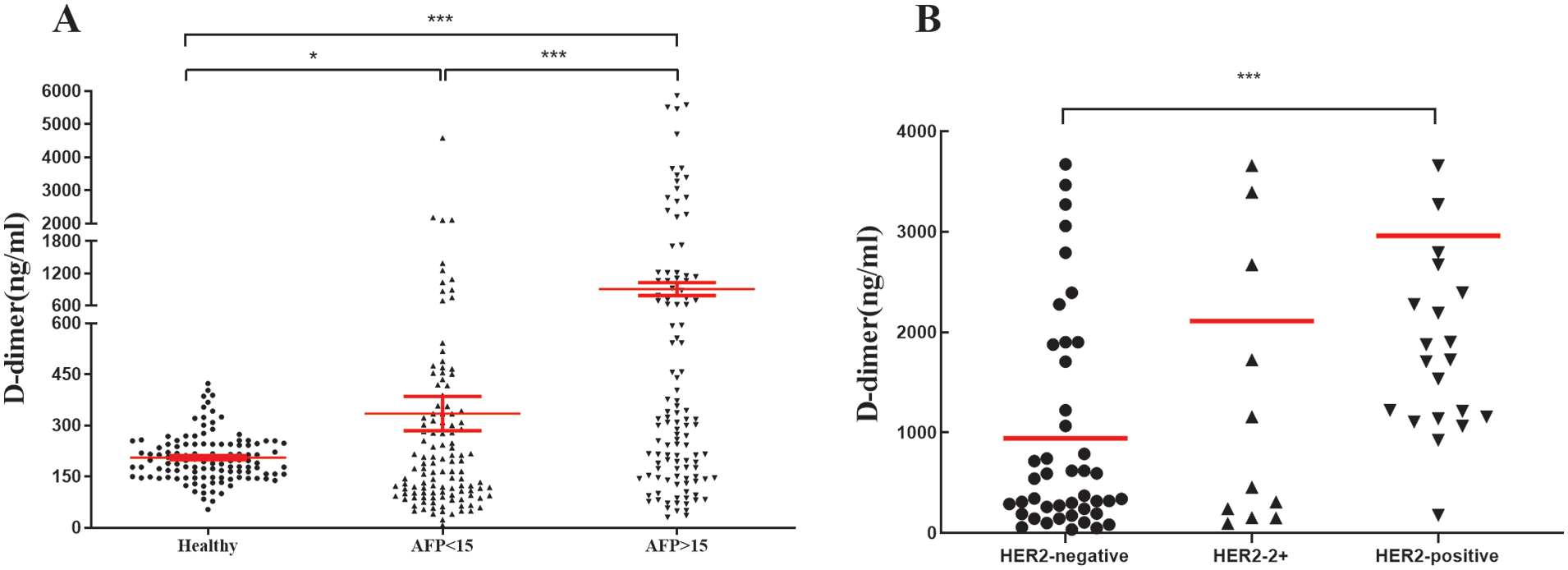
(A) D-dimer levels in healthy people, common gastric cancer (CGC) (AFP < 15 µg/L), and serum AFPGC (AFP ⩾ 15 µg/L). *P < .05, ***P < .001. (B). The scattered plot of serum D-dimer in the HER2-negative and -positive cases in AFPGC,***P < .001.
Clinical factors
We retrospectively collected 120 AFPGC patients. Based on their D-dimer average values, 39 patients with low D-dimer levels (<1000) and 81 patients with high D-dimer levels (⩾1000) emerged to form the team. The relationship with study variables vs D-dimer is presented in Table 1. The mean D-dimer was 1000 (36-13 170) ng/mL. The D-dimer was connected to 14 (45.2%) patients in the T4 stage of the D-dimer (<1000) and 54 (70.1%) patients in the T4 stage of D-dimer (⩾1000; P = .028). The value of D-dimer was found to be related to tumor metastasis, with 20 (52.6%) of low D-dimer (<1000) and 52 (88.1%) of high D-dimer (⩾1000; P < .001). However, there was a meaningful difference in the human epidermal growth factor receptor-2 (HER2; P < .001), including HER2 (3+) (2, 5.3%) of D-dimer (<1000) and HER2 (3+) (⩾1000; 22, 29.6%). Figure 1B shows a scattered plot of serum D-dimer in the HER2-negative and -positive cases in AFPGC (P < .001).
Clinicopathological variables versus D-dimer in patients with AFPGC.

P < .05, ***P < .001.
Our study also demonstrated that pretreating serum D-dimer levels was weakly associated with the levels of AFP (R2 = 0.043; Figure 2A), CA19-9 (R2 = 0.034; Figure 2C), CA242 (R2 = 0.147; Figure 2D), and CA72-4 (R2 = 0.093; Figure 2E). By contrast, there were no relationships between the levels of pre-treatment D-dimer and CEA in serum (P = .244; Figure 2B). Further study concerning the relationship between the stratified levels of D-dimer and the levels of AFP, CEA, CA19-9, CA242, and CA72-4 was discussed. Among the 120 AFPGC patients, there were significant differences in the serum AFP (P = .0000), CEA (P = .007), CA19-9 (P = .004) levels, and no significant difference in the CA242 (P = .531) and CA72-4 (P = .710) levels between 39 patients with low D-dimer (<1000) and 81 patients with high D-dimer (⩾1000) (Table 2). These data demonstrate that the value of D-dimer and tumor biomarkers may be irrelevant regarding tumor progression.

The relationships between peripheral tumor biomarkers and D-dimer in AFPGC patients. (A). The level of AFP was weakly associated with the D-dimer value (R2 = 0.043); (B). The level of CEA was not associated with the D-dimer value (P = .244); (C). The level of CA19-9 was weakly associated with the D-dimer value (R2 = 0.034); (D). The level of CA242 was weakly associated with the D-dimer value (R2 = 0.147); (E). The level of CA72-4 was weakly associated with the D-dimer value (R2 = 0.093).
Tumor makers vs D-dimer in AFPGC patients.

P < .001.
Survival and Cox multivariate regression analysis
All patients received follow-up. The survival curve analyses showed that there was a significant difference in the OS times between patients with low D-dimer (<1000), with a rate of 30.76% and high D-dimer (⩾1000) with 12.30% (P = .0027; Figure 3A). Compared to the high D-dimer group, the recurrence free survival (RFS) of the low D-dimer group was significantly shortened, and the difference was found to be statistically significant (P < .0001; Figure 3B). Furthermore, in this study, such significant characteristics, such as age, sex, tumor site, and D-dimer level, were chosen for a univariate analysis among the AFPGC patients. T-stage, distant metastasis, vascular embolism, the levels of D-dimer, and tumor biomarkers of AFP and CA19-9 in tissues significantly impacted the OS (Table 3). The Cox multivariate analysis of these parameters selected by univariate analysis identified them as independent predictive factors for OS. Fortunately, this result indicated that T-stage, distant metastasis, vascular embolism, level of D-dimer, and the tumor biomarker of AFP were all independent risk factors for survival (Table 3).
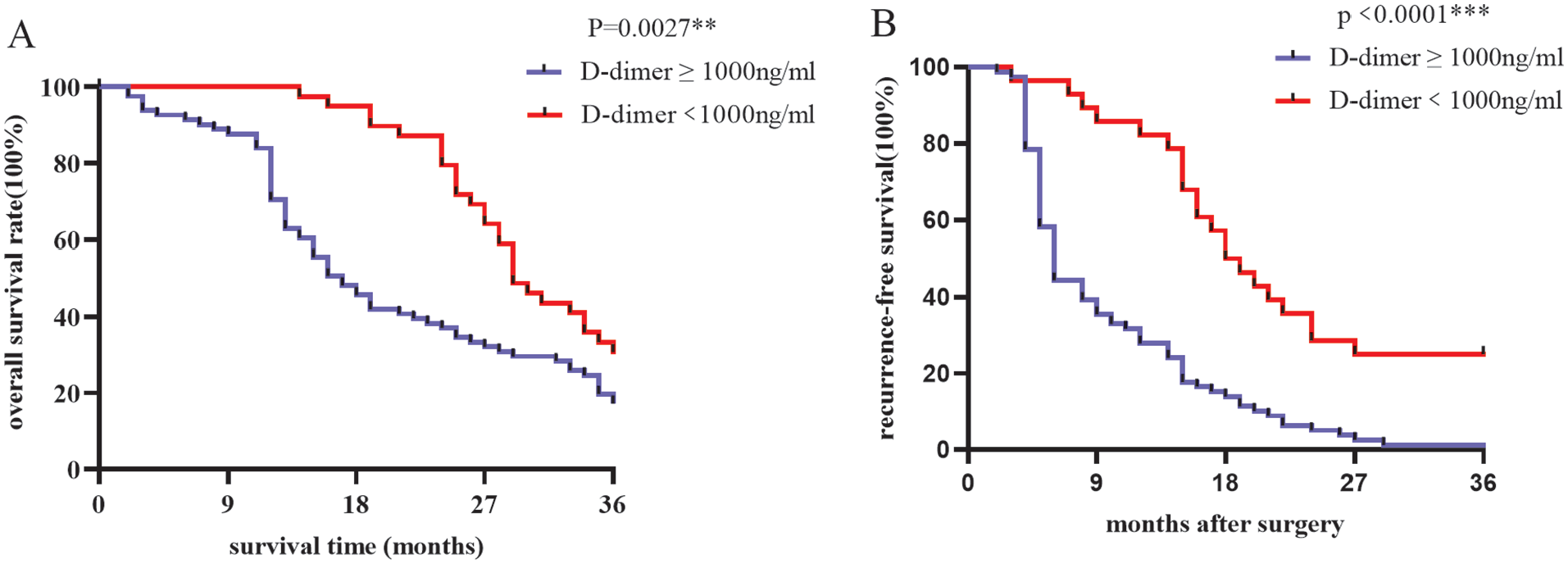
Survival curves were calculated by the Kaplan–Meier method. Take time as the horizontal axis and survival rate as the vertical axis. (A). 3-year OS curve of AFPGC patients stratified by serum D-dimer values (1000 ng/mL). The patients with low D-dimer (< 1000), with a rate of 30.76% and high D-dimer (⩾1000) with 12.3% (P = .0027). (B). 3-year RFS curve of AFPGC patients stratified by serum D-dimer values (1000 ng/mL). The patients with low D-dimer (<1000), with a rate of 18.5% and high D-dimer (⩾1000) with 6% (P < .0001).
Prognostic factors for AFPGC.

P < .05, ***P < .001.
Discussion
Worldwide, GC is most prevalent in China, as it accounts for approximately 40% of the 1.2 million new cases of GC in the world every year. AFPGC is a rare clinically malignant tumor that has a unique clinical pathology and bad prognosis. Therefore, improving the understanding of pathological morphology and immunophenotype of AFPGC can help prevent misdiagnosis for the more common adenocarcinoma, which can cause an underestimation of its malignancy, and provides better clinical treatment. As with ordinary GC, early diagnosis and radical surgery are the only means to cure it. However, advanced AFPGC is highly invasive and malignant, so chemotherapy is the main treatment. Because the pathogenesis and molecular mechanism of AFPGC are still unclear, the choice of targeted drugs is still based on common gastric adenocarcinoma. The D-dimer is a stable end degradation product that was produced by a fibrin monomer that is cross-linked by the activator XIII, and then hydrolyzed by fibrinolytic enzymes. 11 The presence of D-dimer indicates the existence of coagulation and subsequent fibrinolysis. D-dimer is widely used to diagnose disseminated intravascular coagulation, thromboembolism, and myocardial infarction. Recently, it has been reported that high levels of D-dimer can be detected across certain types of cancers, 12 such as lung cancer, 5 oral cancer, 13 prostate cancer, 14 and colorectal cancer. 15 Our research initially demonstrated that D-dimer levels were significantly higher among patients with AFPGC compared with healthy volunteers and AFP-negative GC (Figure 1A). Many people believe that increased plasma fibrinogen and D-dimer levels are related to metastasis, recurrence, and shortened cancer survival. Diao et al 16 demonstrated that serum D-dimer levels were advanced among typical stomach cancer patients, with metastasis of distant visceral. The same results were obtained for AFPGC with a tendency for distant metastasis (P < .001). It is believed that fibrin may form a protective barrier among tumor cells and promote angiogenesis, thereby making tumor cells resist endogenous defense mechanisms, promoting tumor growth, invasion, and metastasis. At the same time, it has also been reported that D-dimer in plasma is a procoagulant marker, which is able to express circulating tumor cells or micro-metastasis. 17 Recent studies have reported a positive correlation between circulating tumor cells and plasma D-dimer levels among patients with metastatic breast cancer.18,19 Diao et al 20 observed that among patients with GC with distant metastasis, particularly those with visceral metastasis, the plasma D-dimer levels increased significantly. SALL4 is widely expressed in yolk sac tumors, and also in AFPGC. 21 In addition, some articles pointed out that patients with SALL4-positive tumors were more likely to have metastasis.22-24 Therefore, we are able to speculate that the level of D-dimer is an essential indicator for the discovery of metastasis and progress of AFPGC.
To date, there has been no report about the indicator of poor prognosis with optimal cut-off point in AFPGC. In cancer patients who have higher D-dimer levels, there is a tendency for poor survival prognosis. We defined the cut-off value ⩾1000 ng/mL with predicting poor prognosis in AFPGC. It has been reported that D-dimer levels were influenced by age, but not sex, in patients.16,25 However, in our study, our sample size may not have been enough to get the best cut-off value, which eventually led to no significant difference among sex and age between D-dimer (<1000 and ⩾1000). A significant correlation was reported between high D-dimer, fibrinogen degradation product, and tumor node metastasis (TNM) staging of colorectal cancer. 26 In fact, they considered D-dimer to be a promising predictor of clinical staging among patients with GC. 20 It has been confirmed that the D-dimer level was related to the depth of tumor invasion in patients with colorectal cancer who underwent surgical resection. 27 The diagnosis of AFPGC is largely dependent on pathomorphology and immunohistochemistry. Studies have demonstrated that all AFPGCs express GPC3, and that the expression level of GPC3 may be related to the T-stage of the tumor. 21 Therefore, GPC3 can be used as a therapeutic target for AFPGC. Furthermore, it has also been confirmed that the level of D-dimer was found to be related to the cancer stages of AFPGC patients and was positively related to tumorigenesis (P = .028).
HER2 is a proto-oncogene that was encoded by ERBB2 on chromosome 17. According to earlier studies, it is now clear that HER2 is expressed across many tissues, including the breast, gastrointestinal tract, kidneys, and heart.28-30 Its main function in these tissues is to promote cell proliferation and inhibit apoptosis, which can help promote uncontrolled cell growth and tumorigenesis. HER2 is associated with the progression and adverse clinical outcomes among several types of tumors, such as advanced gastric and gastroesophageal junction cancer.31,32 Some molecular-targeted drugs can prolong OS and progression-free survival in HER2-positive cancers. 33 In AFPGC patients, HER2-positive expression of high D-dimer levels was higher compared with low D-dimer levels, which were 29.6% and 5.3%, respectively. HER2 is frequently expressed in common gastric cancer (CGC) and has become a common therapeutic target. 34 It is expected that additional anti-HER2 drugs will be developed and introduced into clinical practice to treat HER2-positive cancers, including AFPGC.
Due to the rapid progression of AFPGC, it is of great significance to study more convenient, economic, and nontoxic biomarkers, including AFP and CA19-9, to observe clinical progress. 35 Augmented CA19-9 and CEA levels were statistically significantly associated with 5-year disease-free survival and OS rates. 36 It is reported that there is an advanced pattern of serum CEA, CA19-9 among AFP-producing GC patients, 37 particularly regarding serosal involvement, lymphatic and venous invasion, and lymph node metastasis.38-40 Our present study revealed that preoperative serum D-dimer levels were weakly associated with other tumor biomarkers, including AFP, CEA, and CA19-9, in AFPGC patients. However, there was a significant difference in the serum AFP, CEA, and CA19-9 between patients with low D-dimers (<1000) and high D-dimers (⩾1000). The increase in D-dimer levels may indicate an increase in tumor growth and the activity of tumor cell expansion. In this study, we demonstrated that AFP, CA19-9, and D-dimer significantly impacted the OS of AFPGC patients. Our research showed that there was a significant difference in OS between low D-dimer (30.76%) and high D-dimer (12.30%; P = .0027). As with ordinary GC, early diagnosis and radical surgery were the only means to cure it. However, due to the rapid progression of AFPGC, and the high rate of liver metastasis, some patients have lost the chance to operate when they were diagnosed. Therefore, the study of AFPGC has certain practical significance for clinical diagnosis, treatment, and follow-up review (especially for some easily detectable indicators, such as D-dimer).
The abnormality of coagulation in a tumor is usually accompanied by the development of malignant tumor. Detecting levels of D-dimer have certain clinical application value for judging whether AFPGC has metastasis. Early medication and proper management can help improve the quality of life and prognosis of patients. The detection rate of early GC is relatively low in China, as is the case among western countries. Gastrectomy cannot be conducted in most AFPGC cases. The advantage of this study is that preoperative D-dimer levels were monitored and found to be related to the staging and metastasis of AFPGC, which truly reflects the prognosis. These findings will be helpful to further understand AFPGC and to develop interventional therapy in future clinical practice to improve prognosis. The deficiency of this study is that D-dimer was not detected after operation and during the change of disease. Hence, it is impossible to conduct a comprehensive analysis. Another limitation is that the sample size of AFPGC patients is small, and the observation time is short, which is worthy of further verification among a large cohort. Therefore, prospective and multicenter studies are needed to identify the accurate relationship between D-dimer and the prognosis of AFPGC patients.
Conclusions
Serum AFPGC is a clinically rare gastric malignant tumor that has significantly different biological characteristics from AFP-negative GCs. D-dimer was expressed significantly higher in AFPGC compared with AFP-negative GC. The variables, including T-stage, distant metastasis, and the expression of HER2, were found to be associated to the value of the D-dimer. It has been verified that the level of D-dimer may serve as an independent risk factor for survival in AFPGC patients, as high D-dimers (⩾1000) were seen to be at a higher risk of adverse outcomes compared with low D-dimers (<1000).
Footnotes
Acknowledgements
The authors thank the members of Department of Etiology and Tumor Marker Laboratory, Shanxi Province Cancer Hospital.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Contributions
XZ and JJ contributed in conception or design of the work; XZ, WW, and BT participated in experiment and data collection; XZ and YW contributed in data analysis and interpretation; XZ participated in drafting the article; JJ performed the critical revision of the article and contributed in final approval of the version to be published. All authors read and approved the final article.
Ethical Approval
The study was granted exemption from ethical review committee of Shanxi Province Cancer Hospital (Ethics No. 202208).