
Abstract
Introduction:
Oral squamous cell carcinoma (OSCC) is one of the highest-ranking cancers among both genders in Pakistan. Obesity is linked to a much higher risk for developing multiple cancer types. Individuals with Diabetes mellitus (DM) face an increased risk for developing oral cancer. Hence, the objective of this study was to identify the effect of obesity and DM on the prognosis of OSCC patients.
Methods:
This retrospective cohort analysis was conducted on 386 patients diagnosed and treated for OSCC at The Aga Khan University Hospital, Karachi, Pakistan. Patient information was obtained from hospital medical records. Obesity was defined as having a body mass index (BMI) of ⩾25 kg/m2 according to the WHO Asian cut-offs for BMI. Patient BMI was correlated with diabetes status, clinicopathological features and overall survival. Kaplan-Meier survival analysis was performed, along with univariate and multivariate cox regression analysis to test the effect of obesity and diabetes on overall survival.
Results:
In a set of 386 patients, there were 296 males (76.7%) and 90 females (23.3%). The mean BMI was 24.4 (SD ± 5.25) and 42.7% of patients were found to be obese (⩾25 BMI). 64 patients (16.6%) were diabetic. The risk of death was significantly higher in underweight patients (P = .035) compared with normal weight individuals. Diabetics had a higher mean BMI compared with non-diabetics. However, DM was not a statistically valid predictor of survival.
Conclusion:
Underweight OSCC patients were at a higher risk of death compared with normal weight OSCC patients.
Introduction
Oral squamous cell carcinoma (OSCC) ranks as the sixth most common head and neck malignancy and makes up about 90% of all oral cavity cases. In Pakistan, it is the leading cancer in males and the second-highest in females. 1 The most common presentation for oral cancer in Pakistan is a male in his forties, with a low socioeconomic background and mouth habits that increase the risk for developing oral cancer. 2 In Karachi alone, the consumption of certain forms of chewing tobacco (gutka/niswar), cigarette smoking, alcohol, betel quid (paan), areca nut (chaliya), and their combinations have become a leading cause for oral malignancies. 3 Moreover, viral infections such as Human Papillomavirus (HPV) infection also increase the risk of developing oral cancer. HPV is a causative factor in up to 20% of oral cancers and 60% to 80% of oropharyngeal cancers. 4
Obesity is widely known as a leading cause of patient morbidity and mortality. As an invaluable indicator of patient nutrition status, body mass index (BMI) is frequently assessed in oncological investigations. Previous reports highlight the effect of BMI on treatment outcomes of breast, colorectal, oesophageal, and other cancers. 5 Moreover, some have suggested that about 3.6% of all cancer cases may be attributable to a high BMI, 6 while others have indicated that weight gain and obesity may cause up to 20% of all cancer cases. 7
There is limited data on the prevalence of obesity among the Pakistani population, however, available statistics show that a quarter of the population of Pakistan is overweight or obese. Middle-aged females of Pakistan have been reported to have the highest rates of obesity of any other group. A developing country such as Pakistan appears to be at a greater risk for obesity-associated diseases, and a large part of the population is at risk of disability or even death. 8 A study by Khan et al 9 also observed increasing comorbidities with increasing level of fatness in a dose-dependent fashion in the Pakistani population.
The term diabetes mellitus (DM) broadly refers to a group of metabolic disorders resulting from defects in insulin secretion and action, eventually leading to hyperglycaemia.10,11 In Pakistan, the prevalence of DM among individuals >5 years of age was noted to be 12%. 12 In 2000, it was reported that 5.2 million individuals suffered from diabetes and this number is predicted to increase to 13.9 million by the year 2030. 12 Although there have been several investigations regarding the role of diabetes in OSCC, the results so far are inconclusive. 13 It has been seen that diabetic OSCC patients suffer from a severe increase in risk of disease recurrence and mortality. 14 A meta-analysis of 13 studies conducted in 2015, including Asian studies, revealed diabetics to be at a higher risk of developing oral precancerous lesions and cancer, in comparison to non-diabetics. Furthermore, Type 2 DM is also associated with increased oral cancer mortality 13 and survival among diabetics was lower than non-diabetics. 15
There is a need to evaluate the impact of obesity, and its association with DM, in oral cancer patients among the Pakistani population which can potentially lead to the betterment of cancer care. 15 This study was aimed towards determining the demographic and clinicopathological factors associated with obesity among oral cancer patients and the association of DM and obesity with overall survival among OSCC patients.
Materials and Methods
Study design and patient population
For this study, we conducted a retrospective cohort analysis at The Aga Khan University Hospital (AKUH) Karachi, Pakistan. 386 patients who were diagnosed with biopsy proven squamous cell carcinoma of oral cavity and underwent surgery at AKUH from January 2008 to December 2013 were recruited.
Data sources
Data were collected on patient demographics, tumour site, tumour size, histological classification, lymph node involvement, preoperative body mass index (BMI) and DM status (both type 1 and type 2) from the hospital medical records. Patients follow up at their last clinic visit was also obtained from hospital medical records and patients were reported as either alive or dead. Patients with incomplete medical records and those who sought treatment outside AKU after their initial visit were excluded from the study.
Ethical considerations
Since this was study was conducted retrospectively using the hospital’s records, no patients were contacted directly. This study was granted exemption from ethical review committee of AKUH (ERC# 4335-Sur-ERC-16).
Assessment of body mass index (BMI)
Body mass index or Quetelet index is a measure of the relative size of the body and is defined as body mass in kilograms (kg) divided by the square of height in metres (m2). 16 The World Health Organization (WHO) defines a BMI as underweight (<18.5 kg/m2), normal (18.5-–24.9 kg/m2), overweight (25.0-29.9 kg/m2) and obese (⩾30 kg/m2) internationally. Specific to Asians, the cut-off values of overweight and obesity are lower than the WHO criteria to consider the higher body fat content in Asian populations. Proposed classification of weight by BMI in adult Asians is underweight (<18.5 kg/m2), normal (18.5-22.9 kg/m2), overweight (23.0-24.9 kg/m2) and obese (⩾25 kg/m2). 17
Statistical analysis
SPSS version 22 was used to perform statistical analysis of the data. Descriptive analysis was performed for continuous variables and reported depending on the normality assumption of the variables and assessed by independent t test or Wilcoxon rank sum (Mann-Whitney test), respectively. Chi-square test was used for categorical variables of independence if frequency in each cell was ⩾ 5 and if frequency was found to be ⩽ 5 in any cell, Fisher’s exact test was used. Kaplan-Meier survival curves and log-rank tests and Cox proportional hazards regression analysis were used to compare overall survival (death as endpoint). A second proportional hazard regression model adjusted for the other covariates of the study were used to examine the independent effect of treatment. Unadjusted and adjusted hazard ratio (HR) with their 95% CI was reported. A P value of <.05 was considered as significant.
Results
We enrolled 386 participants diagnosed with OSCC in our study. The study cohort comprised 296 males (76.7%) and 90 females (23.3%), with a mean age of 50.19 (SD ± 13.36). The mean BMI of study participants was 24.4 (SD ± 5.25) and 42.7% of study population was found to be obese (⩾25 BMI). Approximately 16.6% (64) participants had DM.
The mean BMI (25.7 ± 4.35) among DM patients was significantly higher compared with non-DM patients (24.17 ± 5.3) (P value .01). Similarly, DM patients were older compared with non-DM patients with a mean age of 59.70 ± 10.91 and 48 ± 12.97, respectively (P ⩽ .001). DM was found to be more prevalent in obese patients and this claim was supported by the calculation of 1.6% underweight patients that had DM whilst 56.3% obese patients had DM (P value .02) (Table 1).
Diabetes mellitus status in relation to demographic and clinicopathological characteristics among OSCC patients (n = 386).
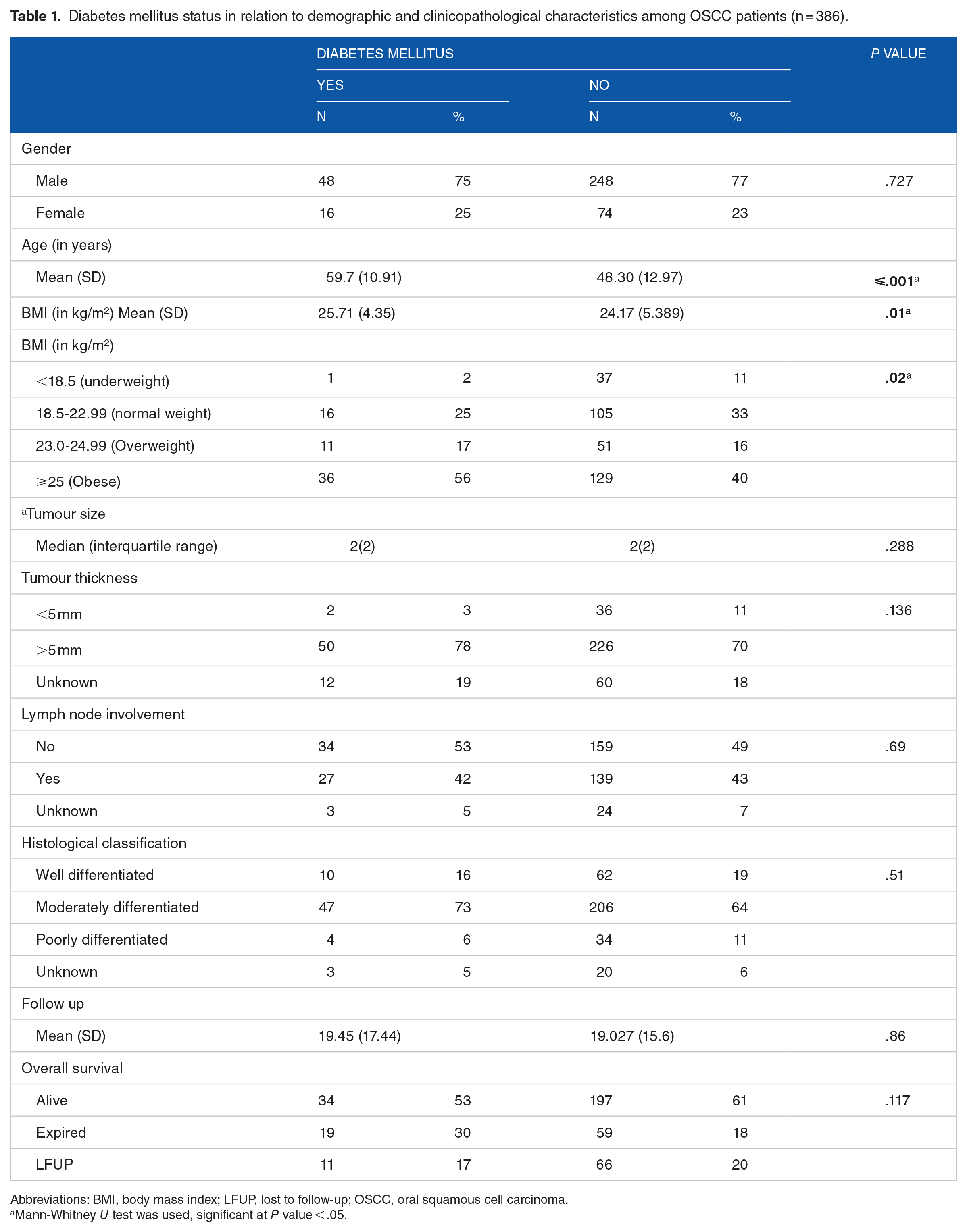
Abbreviations: BMI, body mass index; LFUP, lost to follow-up; OSCC, oral squamous cell carcinoma.
Mann-Whitney U test was used, significant at P value < .05.
Table 2 shows mean survival time of OSCC patients in relation to demographic and clinicopathological characteristics. The mean overall survival time for the study population was 52 months. There was no significant difference in mean survival times for OSCC patients having DM compared with non-diabetic individuals. The mean overall survival time of underweight patients was lower compared with those with normal, overweight and obese individuals, but the difference was not considered significant (P value = .074). Figure 1 shows the survival curves for patients based on diabetes status and BMI.
Mean survival time of OSCC patients compared with clinicopathological characteristics, BMI, and DM status.

Abbreviations: BMI, body mass index; DM, diabetes mellitus; OSCC, oral squamous cell carcinoma.
P value significant at < .05.

Kaplan-Meir overall survival curves of oral squamous cell carcinoma patients according to (left) body mass index categories (underweight, normal weight, overweight and obese: P value = .74) and (right) diabetes mellitus status (Yes, No: P value = .97).
The univariate analysis revealed that increasing age, larger tumour size and lymph node involvement led to poor survival (Table 3). Moreover, underweight individuals also had a significantly poorer survival (P value .019) compared with normal weight individuals. Diabetes status was not a significant predictor of survival on univariate analysis.
Univariate analysis to assess the relationship of factors associated with survival of OSCC patients.

Abbreviations: BMI, body mass index; CI, confidence interval; HR, hazard ratio; OSCC, oral squamous cell carcinoma.
P value significant at < .05.
To assess the independent effect of BMI on survival, multivariate analysis was performed which confirmed the univariate findings: underweight individuals had a higher risk of death (P value .035), meaning that low BMI was an independent predictor for worse survival (Table 4). To study the interaction of BMI and DM, an interaction model was run (shown in Table 4) with normal weight and non-diabetic individuals serving as reference. However, the interaction of BMI and DM was not statistically significant for survival. As observed in the univariate analysis, older age, bigger tumour size and lymph node involvement were all significant predictors for worse survival on the multivariate as well.
Multivariate analysis to assess the relationship of factors associated with survival of OSCC patients.

Abbreviations: BMI, body mass index; CI, confidence interval; OSCC, oral squamous cell carcinoma.
P value significant at <.05 by cox regression analysis.
Discussion
The present study investigated the role of obesity and DM as possible prognostic indicators for overall survival in a cohort of 386 OSCC patients. The mean BMI was significantly higher in the diabetic versus non-diabetic group (P value .01), and the diabetic group was also significantly older than non-diabetic individuals (P value ⩽ .001). A significant interaction between underweight BMI and survival was recognized (P value .035) on multivariate analysis as an independent predictor for survival.
The frequency of obesity among OSCC patients was about 42.7%, while 16 % of patients were overweight. Mean overall survival time for the study population was 52 months. The findings of this study substantiate the data of another study conducted on head and neck squamous cell carcinoma (HNSCC) which suggested that being overweight or obese was an independent prognostic factor for improved survival. 18 The possible explanation for this lies in the fact that obese people have unusually replenished energy stores which exhibit a protective effect. Therefore, in this study the energy stores among obese patients might have protected them from wastage of energy and inflammation. This provides reinforcement of the previous research confirming the action of adipose tissue as a buffer, in addition to providing an evolutionary survival advantage. 19 In the authors’ experience, it has been observed that adjuvant therapy in the form of radiation and chemotherapy is difficult to endure and has several detrimental health effects, which are often well-tolerated in patients of normal or above-normal BMI. Moreover, most patients present with advanced disease, and this further complicates their treatment and survival. Previously published work by the same authors on thyroid cancer also unveiled the majority of patients to be obese and female. 20 This tentatively suggests a trend of obesity among various cancer patients in Pakistan and further larger studies encompassing other cancer types might be able to highlight causative factors.
Although in this cohort, diabetes was not a significant predictor for survival, however, other studies have suggested a significant impact of DM on the overall survival of OSCC patients. 14 The majority of our study participants were male and previous studies suggest that men are more likely to sustain better metabolic control, directing to less levels of insulin and causing lesser oxidative damage to DNA, which might be a possible explanation for these results. 15
The frequency of DM in our OSCC patient cohort was about 16.6%. A study conducted in Hungary, known for a high incidence of type 2 diabetes and oral cancer, showed 25.9% prevalence of DM amongst oral cancer cases, highlighting a steady increase in the incidence of type 2 diabetes among oral cancer patients in the last 14 years. 21 In addition, our study results illustrated that about 83.4% OSCC patients were non-diabetic but no significant association of DM with OSCC was detected. A large pooled analysis of 12 case-control studies includes Asian, Hispanic, non-Hispanic White, and black races from 12 countries indicated a weak association between diabetes and Head and Neck cancer (HNC). 22 In our study the frequency of diabetes was lower among OSCC patients and the possible explanation of this is that it was a hospital-based study and in such studies prevalence cannot be determined. Therefore, to depict prevalence community-based studies are more appropriate. Furthermore, with limited access to healthcare facilities the possibility of unscreened cases of diabetes amongst the less privileged population must also be considered.
Moreover, our study results indicated that the mean overall survival time was equivalent in both males and females, which is in line with previous studies suggesting no significant difference in overall survival based on gender. 23
The study results also revealed that increasing age escalated the risk of death among oral cancer patients. These findings are consistent with reports from the previous literature; however, there is insufficient information regarding correlation of age and survival among oral cancer patients. 24
In the present cohort, longer survival was observed amongst patients with uninvolved lymph nodes compared with those with involved lymph nodes, which is a well-established predictor for survival. Similarly, consistent with other reports,25,26 our results suggested a high mean survival time in patients with well differentiated tumours which gradually decreased from moderate to poorly differentiated tumour patients with worse survival (P value .039).
Diabetes can have a negative impact on oral health.27,28 A WHO factsheet has predicted that by 2030, DM will be the seventh leading cause of death in the world, and approximately 80% of these deaths are projected to occur in low-to-middle income countries. 29 There is a dearth of information from Pakistan regarding the association of BMI and DM, and their prognostic role in OSCC. The findings of this study cannot be generalized on the overall population as it was a hospital-based study and there is an indisputable need for community-based studies for in-depth evaluation. But we can generalize our results to patients presenting to other tertiary care hospitals of Pakistan. Since these patients all underwent surgical resection, many of them later underwent radio- or chemotherapy as well. However, a large portion of these patients opted for public hospitals for these services due to economic reasons. Hence, due to missing information correlations between different adjuvant treatments could not be incorporated. Larger, multicentre prospective cohort analysis are warranted to fully elucidate the role of DM and BMI as prognostic factors for OSCC.
Conclusions
It is suggested that BMI may serve as an independent predictor of survival in OSCC patients, as underweight patients were seen to be at a higher risk of adverse outcome compared with normal weight individuals. In this cohort, diabetes status did not influence the survival of OSCC patients. Awareness campaigns and counselling of patients may be implemented so that the general population is made aware of the possible risks associated with obesity and a culture of regular exercise and healthy lifestyle may be promoted to maintain a healthy bodyweight.
Supplemental Material
sj-docx-1-onc-10.1177_11795549221084832 – Supplemental material for Body Mass Index and Diabetes Mellitus May Predict Poorer Overall Survival of Oral Squamous Cell Carcinoma Patients: A Retrospective Cohort From a Tertiary-Care Centre of a Resource-Limited Country
Supplemental material, sj-docx-1-onc-10.1177_11795549221084832 for Body Mass Index and Diabetes Mellitus May Predict Poorer Overall Survival of Oral Squamous Cell Carcinoma Patients: A Retrospective Cohort From a Tertiary-Care Centre of a Resource-Limited Country by Yumna Adnan, Syed Muhammad Adnan Ali, Muhammad Sohail Awan, Nida Zahid, Muhammad Ozair Awan, Hammad Afzal Kayani and Hasnain Ahmed Farooqui in Clinical Medicine Insights: Oncology
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Research Program for Universities, Higher Education Commission, Pakistan (Grant ID: 9516/Sindh/NRPU/R&D/HEC/2017).
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
YA conceived and designed the study, performed literature search and manuscript writing. SMAA and MSA performed patient data collection, data interpretation, project supervision and provided financial support. NZ performed statistical analysis and assisted in data interpretation and manuscript writing. MOA and HAK performed literature search and assisted in data collection and manuscript writing. HAF performed data entry and data interpretation. All authors reviewed and edited the final draft of the manuscript.
Ethical Approval
This study was approved from ethical review committee of AKUH (ERC# 4335-Sur-ERC-16).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.