
Abstract
Background:
Concurrent chemoradiotherapy (CCRT) with tri-weekly high-dose cisplatin (HDC) is considered the standard regimen. However, due to significant toxicity, various weekly low-dose schedules have been increasingly used. We investigated the tolerability and survival of patients with head and neck squamous cell carcinoma (HNSCC) who underwent CCRT with low-dose weekly cisplatin (LDC) for Japanese population.
Methods:
A retrospective review was conducted among patients with HNSCC who were treated with CCRT/LDC in our institute. Ninety-five patients who met the criteria were enrolled in this study. We evaluated the cycle and cumulative cisplatin dose, completion rate of radiotherapy, adverse events, and survival outcome.
Results:
The mean cycles and cumulative cisplatin dose were 4.7 cycles and 187 mg/m2. All patients completed planned dose of radiation without prolonged breaks. Leucopoenia was the most frequent dose-limiting factor and 44% patients developed grade 3 or 4 toxicity. The 2-year overall survival and recurrence-free survival were 93% and 74%, respectively. The significant differences of survival outcomes between the patients with total cisplatin dose (⩾200 mg and <200 mg) or among age distribution (35-55, 56-75, and ⩾76) were not observed.
Conclusions:
Concurrent chemoradiotherapy/LDC can be safely administered with acceptable toxicity and survival outcome even if the patients with higher age, lower eGFR, and so on.
Introduction
Concurrent chemoradiotherapy (CCRT) with tri-weekly high-dose cisplatin (HDC) (100 mg/m2) is considered the standard regimen administered concurrently with postoperative or definitive radiotherapy for head and neck squamous cell carcinoma (HNSCC). This regimen administered up to 3 cycles (days 1, 22, and 43) is the preferred therapeutic regimen as category 1a in the NCCN Guideline of head and neck cancers (version 2020). However, due to significant acute or long-term toxicity, only 61% and 64% of the patients could complete 3 cycles even in trial settings.1,2 Various weekly low-dose schedules have been increasingly used in clinical practice.3-6
In Japan, some investigators reported that tri-weekly HDC at a dose of 100 mg/m2 was feasible and that the safety profile was identical to that of pivotal trials previously performed in Western countries. 7 However, other investigators reported that a reduced dose of 80 mg/m2 was recommended in CCRT for the Japanese, in terms of response rate and rates of adverse events (AEs). 8
The Japanese were thought to have weaker renal function because of the lower nephron number than other races, that is, almost two-thirds of white American people. 9 Moreover, hypertension, which is thought to be a nationwide prevalent disease due to dietary habits in Japan, has been reported to decrease the number of nephrons much lower.9,10 In addition, Japan has the highest life expectancy worldwide. For this reason, there is a large cohort of patients who were supposed to have contraindication for HDC due to higher age, insufficient renal function, and so on.
Recently, the results of a randomized phase-II/III trial of postoperative CRT comparing tri-weekly HDC with weekly low-dose cisplatin (LDC) in high-risk Japanese patients with HNSCC (JCOG1008 trial) 11 were presented in ASCO2020, 12 and CRT with LDC was proved to be noninferior to CRT with HDC for the postoperative setting and had a feasible toxicity profile. Therefore, the necessity and demand for CRT with LDC will be predicted to increase.
In this study, we investigated the tolerability, response rate, and survival of patients with HNSCC treated with CCRT and LDC (40 mg/m2/week) in our institute. We also focused on the results of the patients who supposed to have contraindication to CCRT using cisplatin in the clinical trial settings, such as patients with higher age, lower eGFR, and pre-existing cytopenia.
Materials and Methods
Patients and treatment
This study was a retrospective review. All the patients with head and neck cancer treated with CCRT with weekly LDC in definitive or postoperative settings at Kobe City Medical Centre General Hospital between September 2015 and March 2021 were pooled from our database and included in this study. The exclusion criteria were (1) metastatic disease at the time of presentation; (2) histology other than squamous cell carcinoma; (3) patients who discontinued treatment due to progressive cognitive or psychiatric problems; and (4) patient who did not have a first visit at outpatient clinic after discharge. A total of 99 patients were treated during this period. Out of which, 4 patients were excluded according to the exclusion criteria, and 95 patients were included in this study.
Administration of the weekly dose of 40 mg/m2 was chosen as institutional practice because we had encountered several patients with severe acute AEs when receiving CCRT with HDC. Maximum cycles/doses aiming at were set at 7 cycles/280 mg/m2. For patients with pre-existing renal dysfunction or cytopenia, weekly cisplatin dose reduced at approximately 80% (30-32 mg/m2). All patients received 1500 mL of fluid replacement with magnesium as pre and posthydration and were premedicated with a 5-HT3 receptor antagonist, a neurokinin-1 receptor antagonist and dexamethasone. Patients received radiotherapy simultaneously up to the planned dose: 60-70 Gy in 2 Gy fractions/day in definitive settings and 50-60 Gy in 2 Gy fractions/day in postoperative settings. Regarding the radiation modality, 89 patients received intensity-modulated radiotherapy (IMRT) and 6 patients received 3-dimensional conformal radiotherapy (3D-CRT). As for the radiation field, whole neck radiation including primary site was performed for 76 patients, ipsilateral hemi-neck and contralateral upper neck including primary site for 2 patients, ipsilateral hemi-neck including primary site for 11 patients, bilateral upper neck including primary site for 3 patients and primary site only for 3 patients. Weekly cisplatin administration continued until weekly laboratory examinations alerted us to the danger of critical cytopenia, renal dysfunction, and/or electrolyte imbalances. However, radiotherapy usually continued unless AEs would endanger patients’ lives; such as severe aspiration pneumonia and gastrointestinal bleeding needed endoscopic hemostasis. After several cycles of break, concurrent chemotherapy was restated in case that we confirmed recovery in the laboratory data. Seventeen patients received induction chemotherapy as an emergent avoidance of dyspnoea and/or dysphagia before CCRT (Table 1). Patients who were planned to undergo irradiation to the whole neck underwent prophylactic percutaneous endoscopic or surgical gastrostomy (40 patients), unless contraindicated or refused by the patient. When the intake by mouth became insufficient, the patients received feeding from gastrostoma or nasogastric tube for the prevention of malnutrition.
Clinical and treatment characteristics of patients.

eGFR, estimated glomerular filtration rate; PLT, platelets; S-1, oral tegaful; TPF, docetaxel, platinum, and 5-FU; WBC, white blood cell.
Distributions of sex, age, performance status, primary sites, new or recurrent case/setting of treatment, clinical tumor node metastasis (TNM) classification for fresh cases (UICC 8th), pretreatment white blood cell (WBC) count, pretreatment platelet count, pretreatment eGFR, and other conditions of the whole patient cohort are shown in Table 1.
Ethical approval and patient consent
This study was approved by the Institutional Review Board at the Kobe City General Hospital (approval no. zn210917), and the need for informed consent was waived because of the retrospective nature of the study.
Methods and statistical analyses
The cycles and total cisplatin doses, the total dose expressed in mg/m2 that a patient received during the irradiation period were estimated and compared among various conditions of the patients. The rate of acute and long-term AEs was also assessed according to the common terminology criteria for AEs, version 4.0 (CTCAE4.0).
Survival analyses were estimated using the Kaplan-Meier method, and differences in survival were compared using a log-rank test. Survival outcomes were compared between primary sites, and according to the cumulative dose of cisplatin and age distributions. Comparisons of variables, such as chemotherapy cycles and cumulative dose of cisplatin between groups were estimated using Mann-Whitney U-tests. EZR on R commander, version 1.42, was used for statistical analysis, and a P value of <.05 was considered significant.
Results
Cycles of chemotherapy, cumulative cisplatin dose, and completion of radiation
The mean number of cycles of cisplatin administration was 4.7 cycles. Three patients had only 1 cycle of cisplatin administration because of acute renal dysfunction, allergic reactions. One patients with acute renal dysfunction continued receiving radiotherapy using weekly cetuximab (anti-EGFR receptor). One patient with allergic reaction continued to receive platinum-based CRT using nedaplatin (CDGP) from the second cycle of concurrent chemotherapy up to 6 cycles. The other patient with acute renal dysfunction continued to receive platinum-based CRT using carboplatin (CBDCA) from the second cycle, but cancelled after third cycles because of gastrointestinal bleeding. One patient refused to receive concurrent chemotherapy after 2 cycles because of appetite loss but continued to receive radiotherapy without chemotherapy. The mean cumulative cisplatin dose of whole cohort was 187 mg/m2. The rate of administration of cisplatin ⩾ 200 mg as concurrent chemotherapy was 62%, and counting nedaplatin or carboplatin as platinum, the rate of administration of platinum ⩾200 mg as concurrent chemotherapy was 63%. The distribution of cycles and total doses of cisplatin in the various conditions of the patients were shown in Table 2. Female patients, patients with a postoperative treatment setting, patients after receiving induction chemotherapy, and patients with lower counts of WBCs or platelets tended to have lower cycles and lower total doses of cisplatin; however, any combinations of groups did not demonstrate significant differences of cycles or doses of cisplatin.
The mean cycles and cumulative dose of cisplatin according to clinical and treatment characteristics.

eGFR, estimated glomerular filtration rate; PLT, platelets; WBC, white blood cell.
As for the radiation therapy, all patients completed radiotherapy without prolonged break. The period of 50-Gy irradiation was in the range of 35 to 36 days, 60 Gy for 42 to 45 days, 66 Gy for 45 to 49 days, and 70 Gy for 49 to 58 days.
Adverse events
When analysing AEs, one patient who was administered cetuximab instead of platinum due to acute renal failure after 1 cycle of cisplatin was excluded from this study, and 94 patients were enrolled. Acute AEs according to CTCAE version 4 are listed in Table 3. The worst grade during treatment was counted. As expected, leucopoenia and oral/pharyngeal mucositis were the major problems during therapy. In the whole cohort, 31% of the patients had grade-3 mucositis and 44% developed grade-3 or -4 leucopoenia. Oral/pharyngeal mucositis could be managed using gastrostoma or nasogastric tube feeding and opioid administration, and leucopoenia was the most frequent dose-limiting factor for weekly cisplatin use. However, we encountered just 2 cases with grade-2 febrile neutropenia which could be managed with G-CSF and antibiotics administration. We experienced unexpected AEs, congestive heart failure, and gastrointestinal bleeding, but we managed them with diuretics and endoscopic hemostasis without a prolonged break in radiotherapy.
Distribution of acute adverse events graded by CTCAE version 4.0 (percentage).

CTCAE, common terminology criteria for adverse events, version 4.0; ND, not defined in CTCAE, version 4.0.
The long-term AEs according to CTCAE version 4 are also listed in Table 4. The grade was measured by conducting an interview with the patient at an outpatient clinic 1 year after treatment. Then, 20 patients without enough observation periods were also excluded. Although inner ear damage is known to be a major side effect of platinum-based chemotherapy, only a few patients (3%) claimed tinnitus or hearing impairment in this series of studies. Swallowing disturbance and loss of taste were the major problems as long-term AEs; however, the primary site of the disease might have affected the results. Especially, 3 patients with grade-3 swallowing disturbance, 2 with stage-4b hypopharyngeal carcinoma and another with stage-4b laryngeal carcinoma, already had pharyngeal stenosis due to the spread of the cancer before treatment.
Distribution of long-term adverse events graded by CTCAE version 4.0 (percentage).
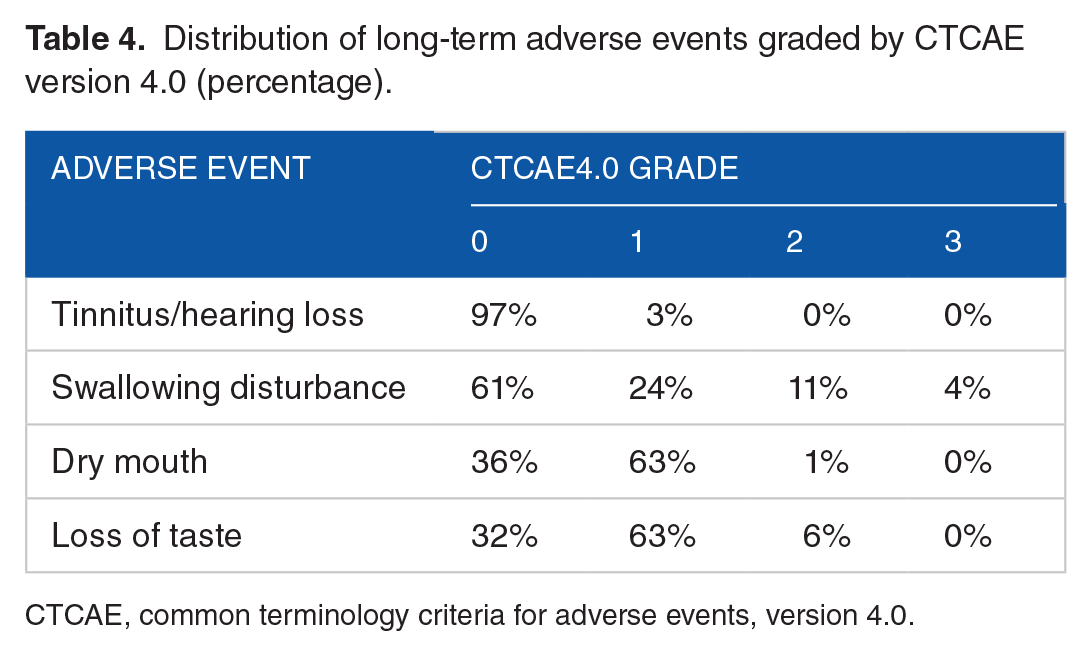
CTCAE, common terminology criteria for adverse events, version 4.0.
Survival outcomes
The median time to death or last follow-up of all patients was 29 months (2.4 years). Five deaths occurred because of the disease, and 3 deaths were due to other causes. Salvage operations were performed in 7 cases, and immune checkpoint inhibitors were used for 11 recurrent cases.
The 2-year overall survival (OS) and 2-year recurrence-free survival (RFS) rates were 93% and 74%, respectively, in the entire cohort of patients (Figure 1A). Looking at the difference between new cases and recurrent case, the 2-year OS rates were 95% and 67% in new cases, whereas the 2-year RFS were 75% and 67% in recurrent cases (Figure 1B and C). The OS outcome was significantly better in fresh cases than in recurrence cases (P = .02); however, significant difference was not observed between these groups in terms of RFS (P = .95).

(A) Overall survival curves and recurrence-free survival curves for the whole cohort of patients according to the Kaplan-Meier methods. (B) Overall survival curves for new cases (89 cases: New) and recurrent cases (6 cases: Recurrence) according to the Kaplan-Meier methods. There was a significant survival difference between these groups by Log-rank test (P = .02). (C) Recurrence-free survival curves for new cases (89 cases: New) and recurrent cases (6 cases: Recurrence) according to the Kaplan-Meier methods. There was no significant survival difference between these groups by Log-rank test (P = .95). OS indicates overall survival; RFS, recurrence-free survival.
The survival outcomes according to the primary sites were also shown in Figure 2. The 2-year OS rates were 100% in carcinoma of unknown origin (CUP), laryngeal carcinomas, nasopharyngeal carcinomas, 96% in hypopharyngeal carcinomas, 75% in oral carcinoma, 95% in p16-positive oropharyngeal carcinomas and 76% in p16-negative oropharyngeal carcinomas. The 2-year RFS rates were 100% in CUP, 75% in hypopharyngeal carcinomas, 91% in laryngeal carcinomas, 78% in nasopharyngeal carcinomas, 63% in oral carcinoma, 70% in p16-positive oropharyngeal carcinomas, and 65% in p16-negative oropharyngeal carcinomas (Figure 3).

Differences in overall and recurrence-free survival among the primary sites of the patients according to the Kaplan-Meier methods: (A) Overall survival; (B) recurrence-free survival. CUP indicates carcinoma of unknown primary (1 case); Hypo, hypopharyngeal carcinoma (30 cases); Larynx, laryngeal carcinoma (11 cases); Naso, nasopharyngeal carcinoma (10 cases); Oral, oral carcinoma (8 cases); Oro(p16−), p16-negative oropharyngeal carcinoma (9 cases); Oro(p16+), p16-positive oropharyngeal carcinoma (26 cases); RFS, recurrence-free survival.

Differences in overall and recurrence-free survival between patients receiving a cumulative cisplatin dose of ⩾200 mg/m2 and patients with a cumulative cisplatin dose of <200 mg/m2 according to the Kaplan-Meier methods: (A) overall survival and (B) recurrence-free survival. No significant difference was observed in terms of overall survival or recurrence-free survival. OS indicates overall survival; RFS, recurrence-free survival.
Survival outcomes were assessed according to total dose of cisplatin used in CCRT. As previously described, the rate of administration of cisplatin ⩾200 mg/m2 as CCRT was 62%. The 2-year OS rates for patients with total cisplatin doses ⩾200 mg/m2 and those with total cisplatin doses <200 mg/m2 were 94% and 91%, respectively (Figure 2A). Patients with platinum accumulated dose ⩾200 mg/m2 showed better prognostic outcome, but a significant difference was not observed (P = .12). As for the 2-year RFS, patients with total cisplatin doses ⩾200 mg/m2 showed better survival outcome than patients with total cisplatin dose <200 mg/m2 (Figure 2B); however, significant difference was not observed (79% and 67%, P = .19).
Finally, survival outcomes were assessed according to age distribution. As described, in the chapter ‘Cycles of chemotherapy, cumulative cisplatin dose and completion of radiation’, there were no significant differences in cycles or total doses of cisplatin among 3 areas of patients’ age, 35-55 years old, 56-75 years old, and 76 years old or more. As shown in Figure 4, there were no significant survival differences among those 3 areas of patients’ age, in terms of OS or RFS.

Differences in overall and recurrence-free survival among the distribution of patients’ age (35-55 years old, 56-75 years old, and 76 years and above) according to the Kaplan-Meier methods: (A) overall survival and (B) recurrence-free survival. No significant difference was observed in terms of overall survival or recurrence-free survival. OS indicates overall survival; RFS, recurrence-free survival.
Discussion
In this study, we retrospectively examined number of cycles, cumulative dose of cisplatin for patients treated using CCRT with LDC. The mean number of cycles of cisplatin administration was 4.7 cycles and the mean cumulative cisplatin dose was 187 mg/m2. The rate of administration of cisplatin ⩾200 mg as concurrent chemotherapy was 62%. The 2-year OS and 2-year RFS rates were 93% and 74%, respectively, in the entire cohort of patients. Leucopoenia was the most frequent dose-limiting factor for weekly cisplatin use in our series of patients.
According to the NCCN guidelines, version 2 2020, weekly administration of cisplatin 40 mg/m2 as concurrent chemotherapy is categorized into recommendation 2B. Two reports are referred for this recommendation: one study by Beckmann et al in 20053 and the other study by Medina et al in 2006. 13 After their report was published in mid-2000s, many reports have compared tri-weekly HDC and weekly LDC administrations directly and assessed the superiority in terms of outcomes and AEs that appeared in some journals.4,5,14-19 Oosting et al 4 compared patients with high-risk postoperative HNSCC treated in 2 different tertiary cancer centres with different institutional practices: one centre used CRT with HDC[tri-weekly 100 mg/m2] and the other used CRT with LDC [weekly 50 mg/m2]. The mean cumulative cisplatin dose and the rate of cumulative cisplatin ⩾200 mg/m2 were 239.8 mg/m2% and 85.2% in a centre using LDC, while those using HDC were 199.4 mg/m2% and 67.7%, respectively. The patients in a centre using LDC received a significantly higher accumulated dose of cisplatin and had a better recurrence-free rate. In contrast, Noronha et al 18 recruited 300 patients with locally advanced HNSCC and performed a phase-III randomized control trial to demonstrate the noninferiority of CRT with weekly administration of LDC [30 mg/m2] against CRT with tri-weekly administration of HDC [100 mg/m2]. In their report, the median cumulative cisplatin dose and the rate of cumulative cisplatin ⩾200 mg/m2 were 210 mg/m2% and 58% in the LDC arm, while the values were 300 mg/m2% and 95.3% in the HDC arm. Both estimated median progression-free survival and median OS were significantly lower in the LDC arm [17.7 months versus 28.6 months and 39.5 months versus not reached, respectively], and the HDC arm resulted in superior survival outcomes compared to the LDC arm, albeit with more toxicity. In 2017, Szturz et al 19 published a meta-analysis of 41 reports for definitive CCRT and 11 reports for postoperative CCRT with 4209 accumulated patients. In the definitive treatment setting, LDC was more compliant and significantly less toxic than HDC, while the 2 approaches showed almost equal compliance and toxicity in the postoperative setting. No significant survival superiority was found in OS neither in the definitive setting nor in the postoperative setting. Bauml et al 5 retrospectively examined the outcomes of 2901 patients with locally advanced HNSCC treated with definitive CCRT with tri-weekly HDC or weekly LDC using population-based Veterans Affairs data. They generated propensity scores for the use in the HDC arm to equalize variables potentially influencing treatment decisions, such as primary site, stage, and comorbidities. They concluded that the use of LDC was associated with survival outcomes similar to those in HDC in the definitive setting, and HDC was associated with significantly higher toxicity than LDC.
In Japan, the efficacy of LDC in the postoperative setting was estimated using a multiinstitutional randomized controlled trial (JCOG1008 trial), and the noninferiority of LDC was proven with better 3-year OS, 3-year RFS, and less grade 3 to 4 acute AEs despite the lower accumulated dose of cisplatin.11,12
By reviewing these reports, the superiority for survival outcome has been controversial between groups; however, fewer AEs were reported in LDC groups. We could expect to expand the indication of CRT with concurrent cisplatin use in patients who are supposed to be contraindicated for HDC. Oosting et al 4 reported in their study comparing weekly administration of HDC and tri-weekly administration of HDC that half of the high-risk patients with postoperative HNSCC did not receive CCRT because of higher age, higher PS score, insufficient renal function, and so on. In the JCOG 1008 trial, the inclusion criteria for patients’ recruitment were age no less than 75 years, ECOG-PS 0 or 1, eGFR more than 60, and so on. 11
In our series of patients, 9 patients were aged over 76, 8 patients were with lower eGFR less than 60, 1 patient had lower WBC count less than 3000 and 3 patients with lower platelet counts less than 10 000. These patients would be excluded from the JCOG1008 trial. However, in the real world, we often performed CCRT using cisplatin to the patients who supposed to have contraindication to this therapy in the clinical trial settings, and this was why the mean cycles and cumulative dose of cisplatin in our study were relatively low, 4.7 cycles and 187 mg/m2. However, the lower cumulative dose of cisplatin, radiotherapy brake did not occurred in our series.
As for AEs, 44% developed grade 3 or 4 leucopoenia, and this was the most frequent dose-limiting factor for weekly cisplatin. Acute renal failure was seen in only 4% of patients and all events were at most grade 2. In the previous studies, HDC tended to lead to a higher rate of acute renal toxicity than LDC;5,15,16 however, 1 paper from Iran reported that renal dysfunction was observed more in LDC group than HDC group. 14 This issue may depend on dietary habit or water intake of people of the nation.
Survival outcomes were excellent, especially in the fresh cases. Intimate follow-up using surveillance FDG/PET-CT and salvage surgery or therapy using immune checkpoint inhibitors might contribute to the excellent OS compared with RFS outcomes. In the recurrence cases, the difference of OS and RFS was not distinguished than new cases, mainly because of fewer choices of the treatment modalities. Patients with platinum-accumulated doses ⩾200 mg/m2 showed better prognostic outcomes than patients with platinum-accumulated dose <200 mg/m2, but a significant difference was not observed in terms of OS or RFS. This might be due to the lack of power of the number, which did not reach to yield the insignificant difference. However, one possible interpretation of this phenomenon is that the effect of cisplatin in a weekly regimen is rather radiosensitising than cytotoxic. The accumulated cisplatin dose may not greatly affect treatment outcomes. Indeed, the JCOG1008 trial resulted in better 3-year OS and RFS in the weekly LDC group despite the lower accumulated cisplatin dose, even if the differences were not significant. Strurz et al 19 reported that mucositis was significantly severer in patients treated with a weekly LDC regimen than those treated with a tri-weekly HDC regimen, which might be attributed to the radiosensitising effect of cisplatin. We may not persist on the accumulated dose of cisplatin in a weekly regimen, and this idea may expand the indication of CCRT with cisplatin to the patients who supposed to have contraindication to this therapy, such as the patients with age over 76. Actually, there were no significant differences among age distributions of the patients. A cohort of patients with age over 76 demonstrated acceptable survival outcomes in terms of OS and RFS (Figure 4).
We recognize the limitation of this study.
First, this study had retrospective nature, and we had not determined survey sample size a priori. The results of statistical analyses which did not reach to significant difference, such as the difference of OS between patients with platinum-accumulated doses ⩾200 mg/m2 and patients with platinum-accumulated dose <200 mg/m2, might be due to the lack of sample number.
Second, we had treated many patients during this study period and had recommended surgery rather than CCRT according to the patients’ condition and the stage of the disease. Healthy, high-stage patients with high-volume but resectable tumours tended to undergo surgery. There had been a selection bias for recruiting patients, who were expected to be controlled by CCRT in the view point of head and neck oncologist or were not indicated for surgery. This might result in a relatively better prognostic outcome in this study than in previous studies in trial settings.
Conclusions
In conclusion, our study showed that CCRT with LDC can be safely administered with acceptable acute and delayed toxicity. However, the mean cycles or the cumulative dose of cisplatin were relatively low, partially because of a cohort of patients with higher age, lower eGFR, and pre-existing cytopenia, the survival outcomes of the cohort were acceptable. This study may aid clinicians and investigators who have been experiencing a treatment dilemma to deal with the patients with advanced HNSCC who were supposed to have contraindication to CCRT with cisplatin.
Author Contributions
S.S. conceptualized study and drafted manuscript. S.T., K.H., T.M., Y.T., T.I., M.Y., and A.H. collected the data of chemotherapy and patients outcome. T.I., T.M., R.A., T.I., and S.O. collected the data of radiotherapy and adverse events of CCRT. All authors have read and approved the final version of this manuscript.
Supplemental Material
sj-pdf-1-onc-10.1177_11795549211048417 – Supplemental material for Concurrent Chemoradiotherapy With Weekly Low-Dose Cisplatin for Japanese Patients With Head and Neck Squamous Cell Carcinoma
Supplemental material, sj-pdf-1-onc-10.1177_11795549211048417 for Concurrent Chemoradiotherapy With Weekly Low-Dose Cisplatin for Japanese Patients With Head and Neck Squamous Cell Carcinoma by Shogo Shinohara, Shinji Takebayashi, Kiyomi Hamaguchi, Tetsuhiko Michida, Yota Tobe, Tadashi Ikenaga, Mami Yasumoto, Ayami Hamamoto, Toshiyuki Imagumbai, Takamasa Mitsuyoshi, Ryo Ashida, Takahiro Iwai and Shun Okabayashi in Clinical Medicine Insights: Oncology
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was financially supported by the Kasahara Fund for the Promotion of Cancer Research.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.