
Abstract
Background:
There is currently no consensus on the optimal management of de novo unilateral upper tract urothelial carcinoma (UTUC) in renal transplant recipients. We aimed to compare the surgical and oncological outcomes of simultaneous bilateral radical nephroureterectomy (SBRNU) and unilateral radical nephroureterectomy (URNU) to determine the appropriate surgical method.
Methods:
Patients who developed de novo UTUC after renal transplantation and underwent surgical treatment at our center were included in the study. Outcomes were compared between the SBRNU group (underwent bilateral RNU within 3 months) and the URNU group using the Mann–Whitney U-test for continuous variables, Pearson’s chi-square test for categorical variables, and the log-rank test for survival data.
Results:
A total of 48 patients were identified, including 21 and 27 patients in the SBRNU and URNU groups, respectively. Comparison of perioperative data showed that the SBRNU group had a significantly longer operative time (P < .001) and hospital stay (P = .040) than the URNU group but no statistically significant difference in the blood loss (P = .171) and morbidity rate (P = .798). After a median follow-up of 65 months, the SBRNU group had a significantly longer disease-free survival (P = .009), longer cancer-specific survival (P = .032), marginally longer overall survival (P = .066), and similar intravesical recurrence-free survival (P = .274) than the URNU group.
Conclusions:
Our data suggest that SBRNU contributes to improved survival without significantly compromising the perioperative outcomes compared with URNU. SBRNU can be considered a feasible option for de novo UTUC after renal transplantation in specialized centers. Prospective studies should be conducted to further explore the best treatment options for this group of patients.
Keywords
Introduction
With the progress of transplantation techniques and immunosuppressive therapy, patient survival and graft function after renal transplantation have improved significantly. However, this longer survival has led to an increased incidence of post-transplant malignancies, which have been identified as the third leading cause of death in renal transplant recipients following cardiovascular disease and infection. 1 In Western countries, the most common malignancies after renal transplantation are skin cancer and non-Hodgkin lymphoma. 2 However, urothelial carcinoma, predominantly located in the upper urinary tract, is a major post-transplant malignancy among the Chinese population.3,4 A previous study reported a 4.55% incidence of upper tract urothelial carcinoma (UTUC) after renal transplantation, which is approximately 10 times higher than the rate in Europe. 4
UTUC is a neoplastic growth of the urothelium from the renal calyces to the distal ureter. Radical nephroureterectomy (RNU) with excision of the bladder cuff serves as the standard treatment. However, it is unknown whether prophylactic contralateral RNU should be undertaken in renal transplant recipients with unilateral UTUC. Proponents found that patients after renal transplantation experienced a high risk of developing synchronous or metachronous bilateral UTUC;5,6 therefore, it is necessary to excise the contralateral upper urinary tract, which is no longer functional. Opponents argued that only case series without a control group exists, that prove the survival benefit of simultaneous bilateral radical nephroureterectomy (SBRNU); however, the limited evidence does not justify the complexity and potential higher complication rates associated with SBRNU. 3
Thus, we aimed to report our cohort on post-transplant UTUC with long-term follow-up and evaluate the feasibility and survival benefit of SBRNU for this group of patients.
Methods
Study design and population
This retrospective cohort study was conducted at the Peking University Third Hospital on receiving approval from their institutional review board (ID: IRB00006761-M2019146, date: March 29, 2019). The inclusion criteria were as follows: (a) any de novo UTUC occurring after renal transplantation and (b) patients who underwent RNU between January 2004 and December 2016. Patients, who presented with metastases, had other malignancies, or underwent simultaneous radical cystectomy were excluded.
Definitions of clinical characteristics
The tumor stage was based on the 2017 tumor–node–metastasis classification. 7 When multiple lesions were present, the pathological features (tumor size, tumor stage, tumor grade, and tumor architecture) were defined by the most advanced ones. If these multiple lesions involved both the renal pelvis and ureter, we attributed the location to “both”; or else, the location was attributed as “renal pelvis” or “ureter” only. Hydronephrosis was defined as positive if any side had a positive finding. Perioperative complications were defined using the Clavien–Dindo classification system. 8
Treatment modality and follow-up plan
UTUC was diagnosed using imaging studies (ultrasound combined with computed tomography urography or magnetic resonance urography). Patients who underwent bilateral RNU within 3 months were included in the SBRNU group; or else, they were included in the unilateral radical nephroureterectomy (URNU) group. 5 The detailed surgical method has been described in previous studies.5,9 Transurethral resection of the bladder tumor was performed in patients with concomitant superficial bladder cancers. Adjuvant chemotherapy (pirarubicin or epirubicin) was administered intravesically after 1 week. Most patients received triple-drug immunosuppressive therapy that combined cyclosporine, tacrolimus, and azathioprine or mycophenolate mofetil with prednisolone after transplantation. The dose of cyclosporine or tacrolimus was lowered after the diagnosis of UTUC, with the dosages lowered to two-thirds of the former dosage and then adjusted according to the level of blood concentration and serum creatinine. The follow-up plan was scheduled depending on the tumor stage and graft condition. Overall survival (OS) was defined as the period from the date of operation to the date of death or the last follow-up (if the patient was alive). Cancer-specific survival (CSS) was defined as the period between the initial surgery and death associated with cancer. Disease-free survival (DFS) was defined as the period from the date of initial surgery to subsequent recurrence or metastasis. Intravesical recurrence-free survival (IVRFS) was defined as the period between the initial surgery and subsequent bladder recurrence.
Statistical analysis
Continuous variables are presented as medians (interquartile range, IQR). Categorical variables are presented as the number of cases (percentage). Baseline features, surgical outcomes, and oncological outcomes were compared between the SBRNU and URNU groups. Continuous variables were compared using the Mann–Whitney U-test, and categorical variables were compared using Pearson’s chi-square test. The survival curve was drawn using the Kaplan–Meier method. The log-rank test was used to compare the survival difference between the two groups. Statistical analysis was performed using IBM SPSS 24, and P < .05 was considered statistically significant.
Results
Clinicopathological characteristics of the cohort
A total of 48 patients were included in the study. All seven patients who were diagnosed with bilateral UTUC preoperatively underwent SBRNU. Fourteen of 41 patients with unilateral UTUC underwent prophylactic SBRNU, while all others underwent URNU. The individual clinicopathological data are presented in Table 1. Female predominance was observed (44/48), with a median age of 58.5 (IQR, 52-64) years. Twenty-nine (60.4%) patients reported a history of consuming Chinese herbs before renal transplantation, which contained aristolochic acid. The median interval between transplantation and the diagnosis of UTUC was 7 (IQR, 4-10) years. Positive symptoms were noticed in 77.3% of the patients at initial diagnosis, which mainly comprised gross hematuria (24/48) and flank pain (14/48). Hydronephrosis was observed in 70.2% (33/47) of the cases, although eight of these 33 cases did not show definite lesions in their preoperative images. Patients in our cohort presented with an aggressive pathological feature, including 68.2% muscle-invasive diseases and 89.6% high-grade diseases. Histologic variants concomitant with urothelial carcinoma were identified in 25% of the patients. Squamous differentiation was the most common (n = 5), followed by sarcomatoid carcinoma (n = 3), glandular differentiation (n = 2), and lymphoepithelioma-like carcinoma (n = 1).
Comparison of the clinical features between the unilateral radical nephroureterectomy (URNU) and simultaneous bilateral radical nephroureterectomy (SBRNU) groups.
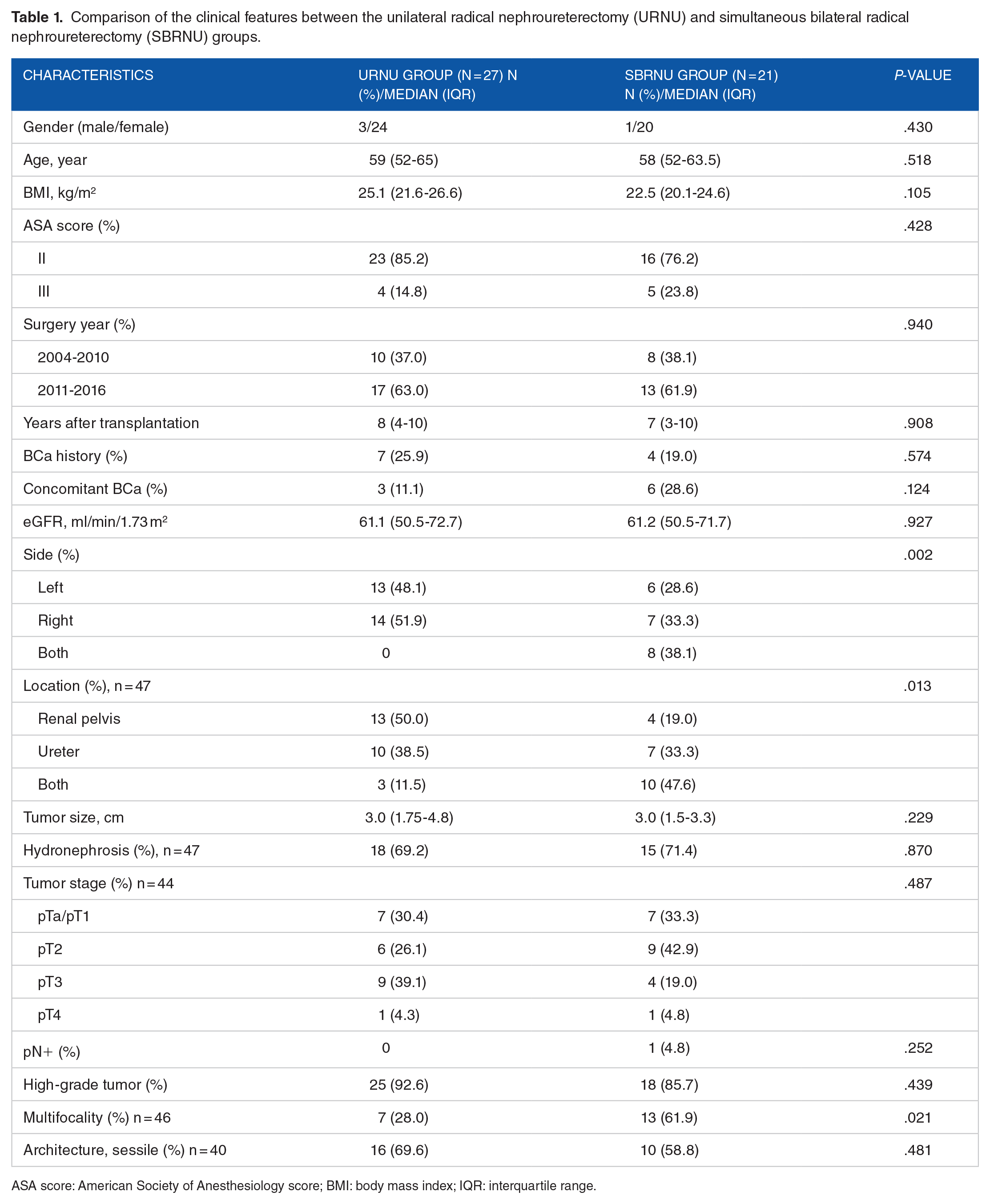
ASA score: American Society of Anesthesiology score; BMI: body mass index; IQR: interquartile range.
The consistency between the preoperative imaging and final pathology was also evaluated. Of the 21 patients who underwent SBRNU, 14 were diagnosed with unilateral UTUC, and seven were diagnosed with bilateral UTUC based on the preoperative images. Pathological results indicated that synchronous bilateral UTUC occurred in eight patients. Four of the 14 patients diagnosed with unilateral UTUC and four of the seven patients diagnosed with bilateral UTUC had bilateral lesions. The sensitivity and specificity of detecting bilateral UTUC were 50% and 76.9%, respectively.
Comparison of baseline features between the URNU and SBRNU groups
The intergroup differences are shown in Table 1. No significant differences were found in the baseline characteristics, except for tumor side (P = .002), tumor location (P = .013), and tumor multifocality (P = .002). The SBRNU group had a higher proportion of bilateral cases, a higher proportion of renal pelvis and ureter concomitant involvement, and a higher proportion of multifocal lesions.
Surgical outcomes
Surgical outcomes are compared between the URNU and SBRNU groups in Table 2. Although the SBRNU group had a longer operative time (230 min vs 125 min, P < .001) and hospital stay (9 days vs 8 days, P = .040) than the URNU group, as expected, no other outcomes were significantly different (blood loss [351.0 ml vs 231.5 ml, P = .171] and perioperative complication rate [9.5% vs 11.1%, P = .798]). Two Clavien–Dindo Grade II complications (ie, pneumonia and hydrops abdominis) and one Grade III complication (ie, small bowel injury) occurred in the URNU group, while two Clavien–Dindo Grade II complications (ie, ileus and anemia requiring transfusion) occurred in the SBRNU group. Perioperative renal function loss of the graft was not observed in either group.
Comparison of the surgical outcomes between the unilateral radical nephroureterectomy (URNU) and simultaneous bilateral radical nephroureterectomy (SBRNU) groups.

Oncological outcomes
The median follow-up period of the cohort was 65 (IQR, 33.8-90.5) months. The median OS was 86 (IQR, 52.0-114.0) months. Local recurrence and/or metastasis were observed in 25 (52.1%) patients, of which 12 subsequently died of UTUC. Intravesical recurrences were noted in nine patients, with a median time of 26 (IQR, 18-68) months from surgery to recurrence.
In the URNU group, 12 patients underwent contralateral RNU due to hematuria, flank pain, or hydronephrosis during the follow-up period, and recurrence was pathologically confirmed in nine patients, suggesting a high contralateral recurrence rate (33.3%). Most contralateral recurrences occurred within 2 years (7/8 patients, 87.5%) with a median interval of 22 (IQR, 17-23.5) months. The other 15 patients did not undergo contralateral RNU, and eight patients experienced local recurrence or distant metastasis with a median interval of 24 (IQR, 4-51) months.
We observed that SBRNU group had a marginally longer OS (median not reached vs 83.0 months, P = .066, Figure 1a), a significantly longer CSS (median not reached vs 92.0 months, P = .032, Figure 1b), a significantly longer DFS (125.0 months vs 25.0 months, P = .009, Figure 1c), and a similar IVRFS (125 months vs median not reached, P = .274, Figure 1d) compared with the URNU group. When we excluded contralateral recurrence in the URNU group, no significant difference existed for local recurrence or distant metastasis between the SBRNU and URNU groups (125.0 months vs median not reached, P = .748, Figure 1e).
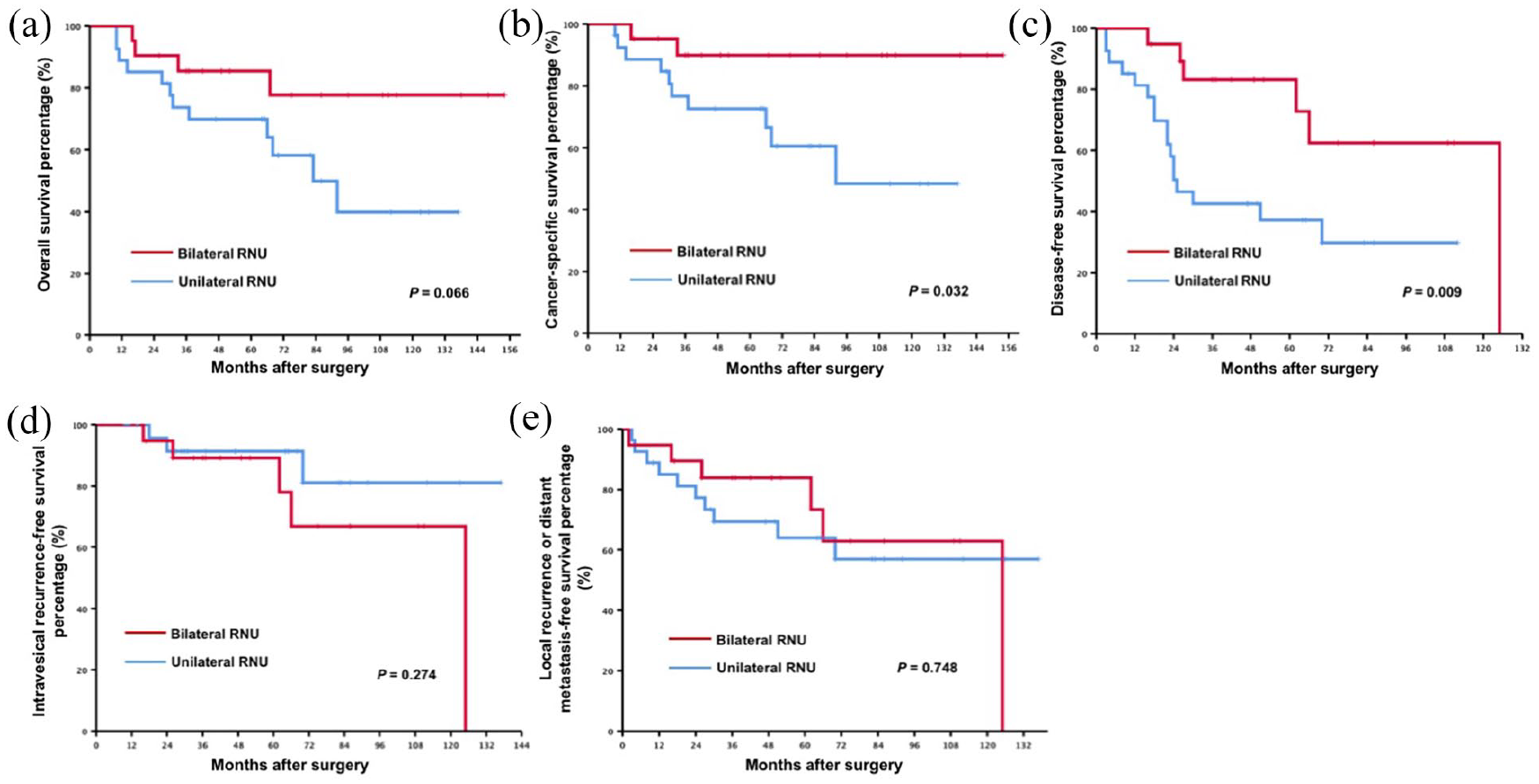
Comparison of the long-term prognosis for the entire cohort: (a) overall survival between the simultaneous bilateral radical nephroureterectomy (SBRNU) and unilateral radical nephroureterectomy (URNU) groups for the entire cohort, (b) cancer-specific survival between the SBRNU and URNU groups for the entire cohort, (c) disease-free survival between the SBRNU and URNU groups for the entire cohort, (d) intravesical recurrence-free survival between the SBRNU and URNU groups for the entire cohort, and (e) local recurrence or distant metastasis-free survival (excluding contralateral recurrence) between the SBRNU and URNU groups.
In the subgroup analysis, we excluded patients diagnosed with bilateral UTUC preoperatively. Results confirmed that SBRNU group had a significantly longer survival than the URNU group in all three outcomes: OS (median not reached vs 83.0 months, P = .005, Figure 2a), CSS (median not reached vs 92.0 months, P = .014, Figure 2b), and DFS (125.0 months vs 25.0 months, P = .008, Figure 2c).

Comparison of the long-term prognosis for unilaterally diagnosed upper tract urothelial carcinoma (UTUC): (a) overall survival between the simultaneous bilateral radical nephroureterectomy (SBRNU) and unilateral radical nephroureterectomy (URNU) groups for unilaterally diagnosed UTUC, (b) cancer-specific survival between the SBRNU and URNU groups for unilaterally diagnosed UTUC, and (c) disease-free survival between the SBRNU and URNU groups for unilaterally diagnosed UTUC.
Discussion
Malignancies in renal transplant recipients have recently attracted increasing attention. The type of malignancy presents considerable differences between different countries and areas. 3 Urothelial carcinoma was reported to be the predominant malignancy in Chinese renal transplant recipients, accounting for more than 40% of all de novo post-transplant malignancies. 3 Exposure to Chinese herbs containing aristolochic acid before transplantation may be the main cause for the higher incidence of post-transplant UTUC in the Chinese population.10,11 It has been reported that aristolochic acid-related DNA adducts were detected in samples of kidneys removed from patients with Chinese herb nephropathy. These adducts are specific markers of aristolochic acid exposure and are directly involved in tumorigenesis. 10 A previous study reported a 4.55% incidence of UTUC after renal transplantation, approximately 10 times the rate in Europe, making research on post-transplant UTUC more feasible in the Chinese population. 4 Herein, we reported our cohort on post-transplant UTUC with a long-term follow-up and evaluated the feasibility and survival benefit of SBRNU for this group of patients.
Our results showed a high proportion of aristolochic acid exposure (60.4%) and a female predominance (91.7%), which is similar to a previous report of UTUC in Chinese renal transplant recipients.5,11 Possible explanations for this phenomenon include frequent use of Chinese herbs among women and female susceptibility to aristolochic acid-related renal damage. The most common manifestations of these patients included hydronephrosis with or without positive lesions (70.2%), gross hematuria (50%), and flank pain (29.2%). Urologists should be vigilant of the possibility of urothelial cancers once renal transplant recipients present these signs, especially in female patients with long-term aristolochic acid exposure.
UTUC in renal transplant recipients shows aggressive pathological features. Muscle-invasive and high-grade diseases were observed in 68.2% and 89.6% of the patients in our cohort, respectively. Given that post-transplant UTUC is invasive and the native kidney is non-functional, RNU with excision of the bladder cuff serves as the standard treatment. However, there is no consensus on whether we should prophylactically resect the contralateral upper urinary tract. In fact, several studies have reported that renal transplant recipients are at high risk of developing synchronous bilateral UTUC. Kao et al 12 identified 24 patients with UTUC after renal transplantation, of which 14 underwent bilateral RNU. Nine (37.5%) patients were pathologically diagnosed with bilateral tumors. Similarly, Wu et al 13 reported 28 renal transplant recipients with UTUC, and bilateral disease was confirmed in 11 (36.7%) patients. On the other hand, contralateral recurrence after RNU is not rare. Fang et al 6 found that post-transplant patients had a greater than 15-fold increased risk of contralateral recurrence compared with non-transplant patients, and 60% (6/10) of the patients after renal transplantation developed contralateral tumors. Huang et al 14 demonstrated that the 5-year contralateral recurrence rate was 38.3% among patients who underwent renal transplantation or regular dialysis, and all recurrences occurred in the first 3 years. These reports preliminarily discussed the need for SBRNU; however, the long-term survival between patients who underwent SBRNU and URNU was not compared.
In our cohort, 48 renal transplant recipients with UTUC were divided into two groups. SBRNU was performed in 21 patients, of which 14 were prophylactic SBRNUs. Bilateral UTUC was pathologically confirmed in 38.1% (8.21) of the cases, including four patients with unilateral UTUC preoperatively. URNU was performed in 27 cases, of which 12 underwent contralateral surgery due to suspected recurrence. Pathology suggested that contralateral recurrence occurred in 33.3% (9.27) of the patients with unilateral UTUC. Given the high incidence of synchronous or metachronous UTUC, SBRNU should be considered as a routine even if unilateral lesions are radiologically detected.
We further observed that the SBRNU group had a significantly better CSS, DFS, and a marginally better OS than the URNU group but not IVRFS. Baseline characteristics did not differ between the groups, except for the tumor side, location, and multifocality, which had a more negative impact on the SBRNU group. When we excluded patients with preoperatively diagnosed bilateral UTUC, the prophylactic SBRNU group still had a significantly longer OS, CSS, and DFS. This improved survival may be associated with the resection of contralateral lesions in radiographically negative patients and the elimination of contralateral recurrences. Perioperative results showed that SBRNU had a close morbidity rate and blood loss compared with URNU. The operative time and hospital stay were also acceptable. Moreover, perioperative function loss of the graft was not discovered. Thus, we concluded that SBRNU contributed to significantly improved survival without compromising the perioperative outcomes.
Although three-quarters of UTUC in renal transplant recipients presented positive symptoms in our cohort, regular follow-up is crucial considering the high percentage of muscle-invasive disease (68.2%) at initial diagnosis. Previous experience has also demonstrated that using clinical symptoms is not enough for the early detection of organ-confined UTUC after renal transplantation. 15 Additionally, if patients undergo only URNU, upper urinary tract screening is important because a considerable proportion of patients experienced contralateral recurrence within 2 years.
There are certain limitations to this study. First, it was limited by its single-center retrospective design. Although most baseline characteristics were comparable between the groups, unmeasured selection bias may still exist. Second, despite being the largest case series to the best of our knowledge, the rarity of this disease limits its sample size. Finally, given the demographic and ethnic differences between Asian and Western patients with UTUC, the conclusion of this study should be examined prudently in the Western population. Multi-institutional collaborations should be encouraged to further confirm the safety and effectiveness of SBRNU.
Conclusion
After renal transplantation, patients present with aggressive pathological features and are at a high risk of developing synchronous or metachronous bilateral UTUC. SBRNU contributes to improved survival without compromising the perioperative outcomes compared with URNU. SBRNU may be the appropriate treatment for selected patients with a high risk of developing bilateral UTUC after renal transplantation, especially in female patients with long-term aristolochic acid exposure.
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by Wu Jieping Medical Foundation (item number: 70516-01).
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
QMZ and RZM contributed equally to this work. All authors participated in the design of the study. QMZ collected the data. RZM analyzed the data. QMZ and RZM drafted the article. XFH and LLM revised and proofread the manuscript. All authors read and approved the final manuscript.
Data Availability Statement
All data that support the findings of this study are collected objectively and are available from the corresponding author on reasonable request.
Ethical Approval
Following institutional review board approval from Peking University Third hospital, we conducted this retrospective cohort study at our medical center. The approval ID was IRB00006761-M2019146.