
Abstract
Introduction:
An education strategy was employed in our department to increase the rate of patients with uncomplicated painful bone metastases undergoing single fractionation radiotherapy (SFRT). The purpose of this report is to analyze the results of this strategy over a 5 year period.
Materials and Methods:
In January 2015, two meetings were organized in our department. In the first, data from an audit on the current SFRT rate were shown. In the second, evidence of SFRT efficacy in the relief of pain from uncomplicated bone metastases was presented. In addition, during the weekly discussion of clinical cases, the opportunity to use the SFRT was systematically recalled. Using our institutional database, all patients treated with radiotherapy for uncomplicated painful bone metastases in the period between 2014 (year considered as a reference) and 2019 were retrieved. Data regarding treatment date (year), radiotherapy fractionation, and tumor, patients, and radiation oncologists characteristics were collected.
Results:
A total of 627 patients were included in the analysis. The rate of patients undergoing SFRT increased from 4.0% in 2014 to 63.5% in 2019 (p < 0.001). At multivariable analysis, the delivery of SFRT was significantly correlated with older patients age (>80 years), lung cancer as the primary tumor, treatment prescribed by a radiation oncologist dedicated to palliative treatments, and treatment date (2014 vs 2015–2019).
Conclusions:
This retrospective single-center analysis showed that a simple but intensive and prolonged departmental education strategy can increase the rate of patients treated with SFRT by nearly 16 times.
Keywords
Introduction
Bone metastases (BMs) are a frequent complication of solid neoplasms and can produce pain and other symptoms significantly worsening the quality of life. 1 External beam radiotherapy (RT) is effective and safe in the relief of pain from BMs. In fact, about 70% of patients undergoing RT experience pain reduction, with complete resolution reaching 30% rate. 2
Several randomized studies have shown that single-fraction RT (SFRT) is equally effective in pain relief compared to multi-fractionated RT (MFRT) in uncomplicated BMs. 3 Furthermore, this result was also confirmed by some meta-analyzes.3–5 Moreover, SFRT produces equivalent results compared to MFRT not only in terms of pain relief but also in terms of quality of life evaluated by patients-reported outcomes 6 and is burdened by lower economic costs.7,8 Based on this evidence, national and international guidelines recommend the use of SFRT in this setting. 9
However, the common reluctance to use SFRT by radiation oncologists (ROs) is well-known, not only in the United States 10 but in most geographic areas.11–13 This preference for MFRT leads to the frequent use of the latter treatment, which is more expensive, potentially more toxic, and less comfortable for the patient. For these reasons, some strategies have been proposed to promote the use of SFRT in the treatment of uncomplicated painful BMs.
Unfortunately, the simple publication and dissemination of guidelines on this subject produced unsatisfactory results. In fact, studies on guidelines impact have shown the lack of increased SFRT prescription 14 or only minimal and temporary variations. 15 Therefore, there is a clear need for new strategies with the aim of achieving a significant improvement of SFRT rates in this setting.
Based on this background, the purpose of this report is to retrospectively analyze the immediate and long-term results of a strategy promoting SFRT in uncomplicated BMs in a large patients population.
Materials and Methods
Study design and setting
This was a retrospective single-center study. The study was approved by the local ethics committee CE-AVEC on 17 December 2020 (NAIVE 1065/2020/Oss/AOUBo). All patients signed a written informed consent to the scientific use of their data and, if feasible, for participation in the study. The medical staff of our RT department, during the analyzed period, included 10 ROs: two ROs with an academic position and eight with a non-academic role. In addition, the department was structured and comprised of two different units: one coordinated by a RO with an academic role and one coordinated by a RO with a non-academic role.
Inclusion criteria
All patients who underwent palliative RT for uncomplicated painful BMs between 2014 and 2019 were included in the analysis. The Cheon’s et al 16 definition of uncomplicated BMs was used for this purpose: “presence of painful BMs unassociated with impending or existing pathologic fracture or existing spinal cord or cauda equina compression.” Furthermore, oligometastatic patients undergoing stereotactic body RT, BMs re-irradiation, and patients younger than 18 years were excluded.
Endpoints
The primary objective of the analysis was to evaluate the SFRT rate from 2015 to 2019. This rate was compared to that of the reference period (2014) following an educational program carried out in January 2015. Secondary objective was to identify any parameters correlated to SFRT prescriptions.
Educational intervention
An internal audit carried out at the end of December 2014 showed that in our center, in the same year, less than 5% of uncomplicated painful BMs underwent SFRT. Therefore, in January 2015 two meetings were organized for our ROs. In the first meeting the results of the internal audit were presented. In the second meeting, the results of the randomized trials and meta-analyzes comparing SFRT and MFRT regimens, and suggestions from national and international guidelines were presented. Subsequently, in the weekly meetings on clinical cases referred to our center, the SFRT option was constantly proposed by the senior consultant in all cases of uncomplicated BMs.
Statistical analysis
Patient age, gender, primary tumor, treatment site, systemic therapy administered at the time of RT, whether the patient was hospitalized or outpatient, patient’s place of residence, and RO’s age and role were explored as potential factors predicting the choice of single versus multi-fraction RT regimen. Predictors of fractionation were explored by the Chi-square test which was used to assess statistical significance (p-value < 0.05 was considered significant). To detect temporal trends in fractionations prescription, SFRT rates were compared by year of RT using the Chi-square test. Variables resulting statistically significant at univariate analysis (p < 0.05) were selected for inclusion in the multivariable analysis. We used the multivariable logistic regression to confirm the potential predictors of SFRT prescription.
Results
Patients characteristics
Overall, 627 treatments were delivered to patients with uncomplicated BMs in the study time frame. Patient characteristics are summarized in Table 1. The male/female ratio was 46.4%/53.6% and patient’s age ranged from 18 to 94 years (median: 68 years). The spine was the treatment site in 49.3% of patients and the most common primary tumors were breast, lung, gastrointestinal, and prostate (31.4%, 24.1%, 13.9%, and 12.6%, respectively). At the time of RT, 50.6% of patients were undergoing some systemic therapy and most of them were outpatients with their place of residence in the same city of our RT department.
Univariate analysis.

Abbreviations: MFRT, multiple fraction radiotherapy; RO, radiation oncologist; RT, radiotherapy; SFRT, single fraction radiotherapy.
Overall intervention’s impact
The rate of SFRT in patients with uncomplicated BMs significantly increased during the study frame time (Figure 1). In fact, SFRT was prescribed in 4.0%, 47.0%, and 63.5% of patients before the audit and the first two meetings (2014), in the following 4 years (2015–2018), and in the last observation period (2019), respectively (p < 0.001).

Variations in radiotherapy prescriptions in the period between 2014 and 2019 (RT: radiotherapy).
Univariate analysis
The results of the univariate analysis on the impact of patients and tumor characteristics on prescribed dose/fractionation are reported in Table 1 and summarized in Figure 2. Patients older than 80 years were more likely to receive SFRT rather than MFRT (61.0% vs 39.0%; p = 0.006). Prostate and breast as primary tumors were correlated with higher rates of MRFT (53.2% and 64.5%; p = 0.033) while SFRT and MFRT rates were almost the same in gastrointestinal and lung cancer. The rate of SFRT was higher (56.7% vs 35.9%; p < 0.001) when the treatment was prescribed by a RO exclusively responsible of palliative treatments. Finally, ROs younger than 50 years were more likely to prescribe MFRT compared to SFRT (66.5% vs 33.5%; p < 0.001).
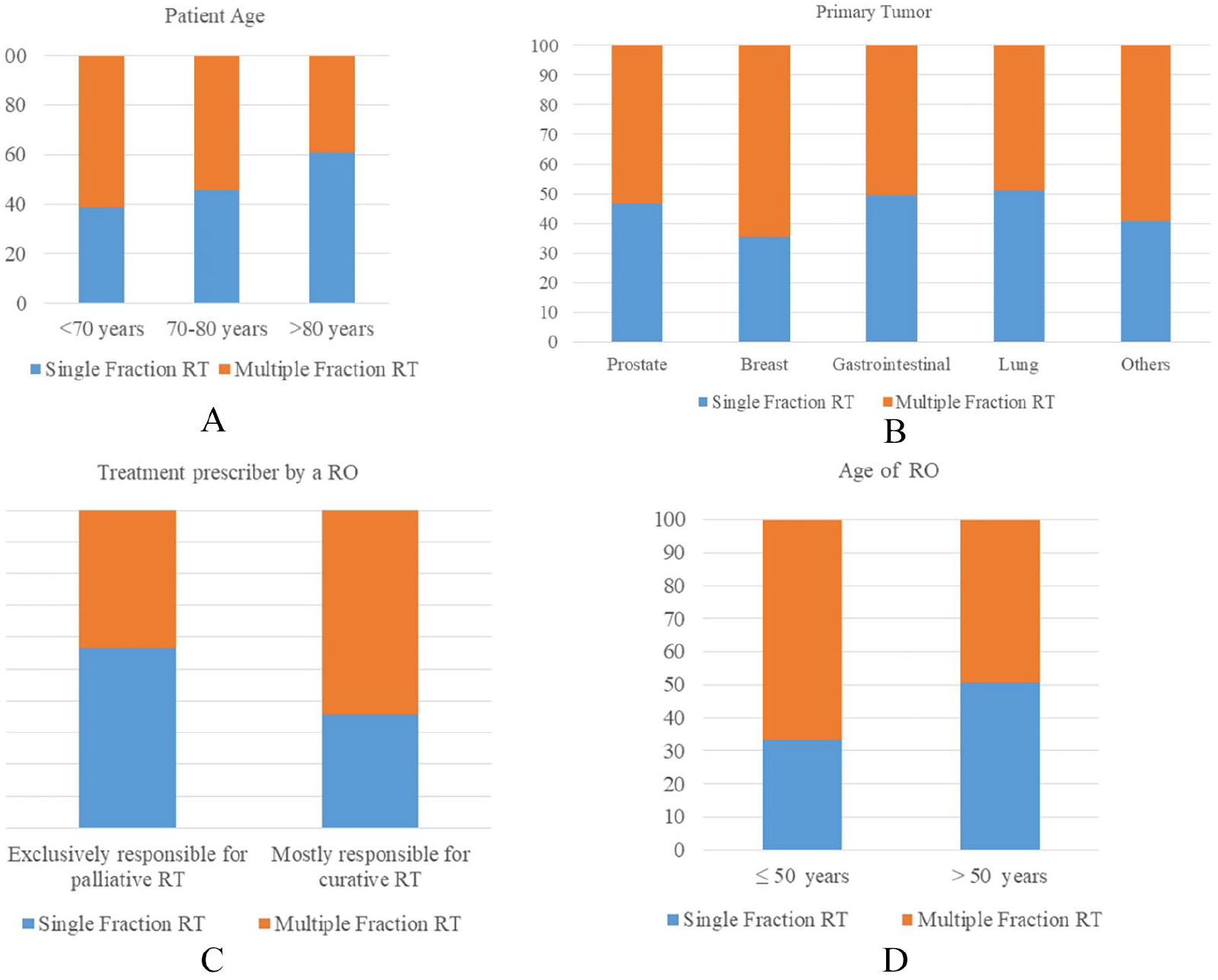
Impact of patients age (A), primary tumor (B), radiation oncologist subspecialty (C), and radiation oncologist age (D) on fractionation prescription.
Multivariable analysis
The results of the multivariable analysis are shown in Table 2. The parameters significantly correlated with SFRT prescription were patient’s age (adjusted odds ratio [AOR] 1.016; p = 0.036), primary tumor (lung vs breast; AOR 0.567; p = 0.019), main type of treatment managed by the RO (palliative vs non-palliative; AOR 1.463; p = 0.033), and period in which the treatment was performed (2015–2019 vs 2014; AOR 20.023; p < 0.001).
Multivariable logistic regression analysis.

Analyzed as a continuous variable.
Discussion
The results of our analysis show that this strategy significantly increased the percentage of patients undergoing SFRT from 4.0% in 2014 to 63.5% in 2019. This result can be considered as a success for the used strategy. However, the extent of this variation could be at least partially attributed to the very low percentage of SFRT before the educational intervention. In fact, considering that in 2014 most evidence and guidelines in favor of SFRT were already available, a compliance rate of only 4.0% is quite surprising. However, it should be noted that this data is very similar to that of other reports.17,18 Indeed, in the studies by Bekelman et al 17 and that of Olson et al, 18 the SFRT rate was 4.7% and 4.0%, respectively.
Our analysis showed a higher increase in SFRT prescriptions compared to other studies. In fact, Olson et al., performed in 2012 an education intervention in six cancer centers (British Columbia) based on the presentation to ROs of meta-analyses, guidelines, and recommendation on SFRT together with data on the regional use of SFRT. They then compared the SFRT rates of 5 years (2007–2011) period before and 1 year (2013) after the intervention. The study results showed a > 10% increase in the use of SFRT after the intervention. 18 Moreover, the same group of researchers published the results recorded in subsequent years (2013–2016), which confirmed a lasting and meaningful 10% increase in SFRT prescriptions. 19 The larger variation recorded in our study (59.5%) compared to that observed by Olson et al 18 (11.7%) may be due to the single intervention performed in the latter experience. On the contrary, in our study, the effect of the first two meetings was probably increased by the constant reinforcement in the weekly clinical cases discussion meetings. However, the observed difference between ours and the Olson’s et al, 18 study could also derive from the different settings. In fact, our experience was conducted in a relatively small RT department (only eight ROs in one single center). In contrast, the experience of Olson et al, 18 was conducted in six different RT centers and involved 10 times more specialists. The more confined environment in which our experience took place may have favored our better results. Furthermore, this positive effect of a non-sporadic intervention seems to be confirmed by the experience of Booth et al. 20 Indeed, these authors used three subsequent audits on fractionation in BMs in a single RT center and they observed the largest reduction of fractions per treatment only after the second audit. The limited results of strategies based on a single type of intervention seem confirmed also by the study by Walker et al. 21 In fact, in this analysis on the impact of dose and fractionation in BMs peer review during weekly chart rounds, the SFRT rate increase was only 11.1% (from 2.8% to 13.9%). Peters and colleagues recently reported on the adoption of single-fraction palliative RT for uncomplicated BMs in a tertiary center. 22 The results of their analysis showed that oncologist-related factors, like personal beliefs and level of training, are presumably the most important driving factors for the prescription behavior. Based on the results of our study, it could be assumed that our non-sporadic intervention was able to change personal attitude and level of knowledge of our ROs. Furthermore, Lievens et al 23 demonstrated a correlation between reimbursement systems and RT practice in the setting of BMs palliative treatment. However, we can rule out that such considerations influenced our results since our analysis was performed in a government hospital, and therefore the reimbursement arrangements have no economic implications for the ROs.
Our multivariable analysis also showed that SFRT prescription is correlated to other factors. In fact, a higher SFRT prescription was significantly correlated to an older age. This data is easily explained by the attempt to limit the discomfort to elderly patients caused by repeated trips from home to hospital. Furthermore, this data confirms analogous results observed in other studies.10,24,25 Similarly, a greater reluctance to prescribe SFRT has been observed in patients with breast cancer compared to lung cancer. The better prognosis of patients with BMs from breast cancer compared to BMs from lung cancer may explain this finding. Similar primary tumor-related differences were observed in other studies. For example, even in the study by Di Lalla et al, 25 lower SFRT rates were recorded in breast cancer patients. As previously mentioned, other studies have shown increased use of SFRT in patients with worse performance status.24,25 Unfortunately we are unable to confirm these results due to lack of available data in our series. Finally, ROs dedicated to palliative RT prescribed SFRT significantly more frequently than their peers. This data can be explained by the greater knowledge and continuous update on scientific evidence in this area. Furthermore, perhaps also by a greater awareness on the effectiveness of SFRT resulting from their clinical practice.
We believe that our study has some strengths. The analysis included a non-negligible number of patients (627), especially considering the mono-centric setting. In addition, the analysis covered a prolonged observation period after the educational intervention (5 years). This feature made it possible to analyze the long-term results of the adopted strategy. At the same time this report has several limitations mainly due to the retrospective design of the analysis. Indeed, this study design limited the analysis of a larger number of parameters that could potentially impact on SFRT prescription. In particular, data on patients’ performance status, which in other analyzes were correlated with SFRT,24,25 are missing in our database. Furthermore, detailed data on systemic therapies at the time of RT are largely missing. Moreover, we must recognize that other factors may have had an impact on SFRT rates variations. For example, starting from 2015, our RT department underwent a progressive technological evolution with the introduction of 4D-computed tomography-simulation, simultaneous protection integrated boost, image-guided RT, stereotactic body RT, and vessel-sparing RT in prostate carcinomas. This evolution led to the need for intensive staff training and a longer duration of some “complex” treatments. Consequently, there has been an extension of the waiting lists for RT start. These issues may have favored the choice of faster treatments in patients with BMs, regardless of the educational intervention.
In terms of generalizability of our results, some observations can be made. First, it was a single-center study. Therefore, the characteristics of the latter may have influenced the overall result. In particular, the study was conducted in a center with “mixed” characteristics, that is, with ROs with an academic and non-academic role. It is possible that in centers with only academic or only non-academic staff, the results may be different. In particular, the audit by Di Lalla et al, 25 performed in an academic center, recorded 85.4% rate of SFRT in uncomplicated BMs. Other studies confirmed that the rate of SFRT in this setting is higher in academic centers compared to community treatment centers.26,27
Conclusions
Results from our and other studies show that a significant increase of SFRT prescriptions in uncomplicated BMs is feasible. In addition, strategies based on an initial intervention (audit/meeting) followed by additional audits and/or periodic meetings reinforcing the concept of SFRT efficacy and safety seem more effective than a single intervention or a simple dissemination of guidelines. Therefore, combined and intensive strategies can be recommended in clinical practice, especially in centers with low SFRT rates in this setting.
Further studies in this field could be based on: i) use of even more aggressive strategies, based for example on the annual repetition of a meeting on this topic including a public sharing of data on SFRT prescription by the different ROs; ii) randomization of ROs into two groups, of which only one receiving an educational intervention in order to assess the impact of the latter while limiting the confounding effect of other factors.
Footnotes
Acknowledgements
we would like to thank Mrs. Cinzia Giacometti for her invaluable help in data retrieval.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Contributors
Conception and design: all authors. Data collection: CMD, EG, AZ, GS, SiC & AGM. Analysis and interpretation of data: EN, CMD, MLA, GS, SCa, FC & AGM. Manuscript writing: all authors. Approval of final article: all authors.