
Abstract
Purpose:
To evaluate clinical outcomes and failure patterns in patients with locally advanced cervical cancer (LACC) treated definitively using image-guided volumetric-modulated arc therapy (IG-VMAT).
Methods and materials:
This retrospective review included 18 consecutively treated patients with LACC. Treatment consisted of IG-VMAT and concurrent chemotherapy followed by intracavitary radiotherapy. The primary end points were overall survival (OS) and disease-free survival (DFS). Acute haematologic toxicity was evaluated using Radiation Therapy Oncology Group (RTOG) criteria.
Results:
A total of 16 patients were either stage IIB or IIIB and the median follow-up was 30.5 months (interquartile range: 13-36.25 months). The 2-year DFS was 63.3% (95% confidence interval [CI]: 52.8%-72.4%) and 2-year OS was 72.2% (95% CI: 62.1%-80.5%). There were 7 treatment failures, predominantly in-field. Acute haematologic toxicity was low.
Conclusions:
IG-VMAT is associated with favourable outcomes for patients with LACC.
Keywords
Introduction
Locally advanced cervical carcinoma (LACC) is a preventable disease and despite advances in screening and management, it still remains prevalent in the developing world along with a disproportionately high mortality rate.1–4 Delay in seeking early medical attention due to inadequate health services in rural areas, belonging to an economically disadvantaged population and prevalence of misconceptions about cancer stemming from a lack of education, leads to patients presenting with locally advanced disease.5,6 Standard management for LACC consists of concurrent platinum-based chemoradiation followed by intracavitary brachytherapy (ICRT) and trials to assess outcomes by adding adjuvant chemotherapy are currently underway.3,4,7
Radiotherapy delivery technique has evolved from bony landmark-based treatment portals to image-guided radiotherapy delivered by intensity-modulated radiation therapy (IMRT). 4 The evidence supporting IMRT in the postoperative and definitive setting is based on reduced side effects when compared with conventional techniques.8,9 Nevertheless, the routine use of IMRT in the treatment of LACC remains controversial and attention needs to be given to target positioning uncertainties arising due to inter/intrafraction organ motion.
Volumetric-modulated arc therapy (VMAT) belongs in the general category of IMRT, with the key advantage of treatment delivery speed, and when combined with image guidance (kilovoltage planar for bony alignment and cone beam computed tomography [CBCT] for soft tissue matching, via an on-board imager) prior to treatment delivery, could potentially overcome some of these issues.10–12 The goal of this study was to analyse clinical outcomes in patients with newly diagnosed LACC who were treated with image-guided VMAT (IG-VMAT) and concurrent chemotherapy (after an institutional policy change in December 2012).
Materials and Methods
Patients
Between January 2013 and December 2014, 22 patients (KPS [Karnofsky Performance Status] ⩾70) were treated for LACC, out of which 4 were excluded (2 received external beam radiation therapy [EBRT] at another institution and 2 were treated with re-irradiation for isolated para-aortic recurrences following prior treatment). Our institutional ethics committee approved this retrospective study.
All patients underwent a pretreatment evaluation consisting of comprehensive history, gynaecological evaluation, complete blood count (CBC), liver and kidney function tests (LFT and KFT), chest X-ray (CXR), cervical tumour biopsy, and contrast-enhanced CT (CECT) scan of the pelvis and abdomen. Parametrial score was recorded as per the work by Hsu et al. 13 Patients were staged as per the International Federation of Gynecology and Obstetrics (FIGO) clinical staging system in a multispecialty gynaecologic malignancy clinic comprising radiation, medical, and surgical oncologists. Informed consent prior to treatment was obtained from all patients.
All patients received a standard supportive care regimen during treatment, which comprised a proton pump inhibitor (pantoprazole 20 mg once before breakfast), 5-HT3 antagonist (granisetron 2 mg once before breakfast), sulfasalazine (500 mg twice daily), a low-residue protein-supplemented diet, and probiotic supplements. During the course of treatment, patient’s haematologic parameters were monitored weekly.
Simulation and treatment
All 18 patients included in this retrospective analysis received definitive radiotherapy with VMAT followed by high dose rate (HDR) ICRT. A radio-opaque marker measuring 5 mm × 5 mm was placed at the lowest end of the cervical growth at the time of simulation. Patients were simulated in the supine position with 4-point thermoplastic immobilization cast for the lower abdomen and pelvis, with a standardized foam block for reproducible separation of the legs. Intravenous contrast was administered as per patient’s body weight. All patients were simulated on Siemens Somatom Sensation Open (Siemens Healthineers, Erlangen, Germany) with a slice thickness of 2 mm and the scan range was set from T12-L1 interspace to mid-femur. About 30 minutes prior to simulation and treatment, patients were instructed to void urine and then drink 1 L of water, to ensure bladder filling. No specific rectal preparation protocol was followed at the time of CT simulation.
Contouring protocol
The clinical target volume (CTV) for all patients was contoured by a single radiation oncologist following the consensus guidelines by Lim et al. 14 The iliac vessels were contoured and given a 7-mm margin to generate CTV_Iliac, and this expansion was subtracted from bone laterally, but not from the bowel loops medially. This decision was taken to account for the fact that bowel loops are mobile and subtracting the CTV from them may lead to compromising the elective nodal CTV, a concern which has been raised by other investigators as well. 15 In addition, the CTV_Iliac was modified to include the space 1.5 cm anterior to the sacrum to include the presacral nodes. The vagina was contoured till 2 cm below the cervical marker, the parametrium was contoured as per guidelines, and the entire fundus of the uterus was included in it. 14 This was named CTV_Vag+Para. The entire mesorectum was treated due to the difficulty in identifying uterosacral ligament involvement in the absence of magnetic resonance imaging–based target delineation.14,16 To account for variable organ filling, a 5-mm isotropic inner margin was generated from the contours of the bladder and rectum. The CTV_Vag+Para was then extended up to these inner contours to generate an internal target volume. Finally, a Boolean operation was performed on CTV_Iliac and CTV_Vag+Para to generate CTV_Final. A representative patient with our contouring modifications is shown in Figure 1.

A representative patient’s contoured plan in the (A) axial and (B) sagittal plane. CTV indicates clinical target volume; PTV, planning target volume.
An isotropic margin of 7 mm was applied to the CTV_Final to generate the planning target volume (PTV_Plan). Organ-at-risk (OAR) was contoured as per Radiation Therapy Oncology Group (RTOG) guidelines. 17 Bowel bag was contoured starting 2 cm cranial from the most cranial slice containing the PTV and excluded the rectum and sigmoid colon from this structure in accordance with RTOG IMRT protocols.
VMAT treatment planning and delivery
All patients were planned on Eclipse treatment planning system v10 (Varian Medical Systems, Palo Alto, CA, USA) with the progressive resolution optimizer (PROII) as inverse planning optimizer, using anisotropic analytical algorithm (AAA) dose calculation algorithm along with modelling of the patient support system, therefore accounting for its attenuation and scattering during the VMAT planning process. All patients were treated on Clinac 2100c (Varian Medical Systems) with VMAT using 2 coplanar mono-isocentric arcs with photon energy of 6 MV. The PTV was prescribed 50.4 Gy in 28 fractions of 1.8 Gy each and was optimized such that 98% of the PTV received at least 98% of prescribed dose (PTV D95% ⩾ 95% was also accepted depending on the discretion of the treating radiation oncologist), Dmax was less than 107% of the prescribed dose, Dmin was greater than 93% of the prescribed dose, RTOG homogeneity index was ⩽0.1, and 98% of CTV received at least 98% of prescribed dose. The region of the PTV overlapping with the bladder and rectum was optimized to achieve Dmax < 103% of the prescribed dose. Two patients were prescribed hypofractionated RT (50 Gy in 18 fractions of 2.78 Gy each) at the discretion of the treating radiation oncologist.
The constraints applied for optimization were as follows: bladder (minus PTV), V45 < 30% (variation accepted, V50 < 35%); rectum (minus PTV), V30 < 60% (variation accepted, V50 < 35%); sigmoid colon, V30 < 60% (variation accepted, V50 < 35%); bowel bag, V40 < 30% and V45 < 195 cm3; femoral heads, V30 < 15% (variation accepted, V30 < 20%). Planning priority was to achieve PTV and CTV coverage first, followed by sparing of the OAR as much as possible without compromising target coverage and homogeneity. In addition to the above, a 3-cm shell optimization structure was created around the PTV to improve high and intermediate dose conformity in addition to preventing the creation of a hotspot outside the PTV.
All treatment plans were evaluated by the treating radiation oncologist and assessed by the medical physicist for deliverability prior to approval. Quality assurance checks were also performed with electronic portal imaging device–based portal dosimetry with a gamma index passing criteria of <3% and 3 mm. For the purpose of retrospective evaluation, dosimetric parameters were collected in accordance with level 2 reporting recommendations by the International Commission on Radiation Units and Measurements (ICRU) Report 83. 18
Online imaging verification was performed for all patients with kilovoltage planar imaging and a CBCT for the first 3 days. The acquired images were reviewed online and offline by the treating radiation oncologist and isocenter shifts were applied to eliminate systematic setup errors. Subsequently, imaging verification was performed on an alternating basis with either kilovoltage planar or CBCT for the remainder of the treatment course. Corrections were applied online for couch shifts exceeding 3 mm but less than 7 mm. For couch shifts exceeding 7 mm, the treating radiation oncologist was notified, and the entire patient setup procedure was performed again along with imaging reverification.
Brachytherapy planning
All patients received HDR brachytherapy with Fletcher-Suit intracavitary applicators. Planning for every fraction was performed on a simulation CT of the pelvis with the applicator in place. Brachytherapy was delivered in 3 once-weekly applications of 7 Gy prescribed to Point A (American Brachytherapy Society definition) with Iridium 192 afterloading source (ICRU bladder and rectal point dose was kept below 70% of prescription dose). 19 Brachytherapy planning was performed on BrachyVision treatment planning platform (Varian Medical Systems) and treatment delivered on Varian GammaMed Plus iX HDR afterloader (Varian Medical Systems). The total biologically equivalent dose in 2 Gy fractions (EQD2) for patients receiving standard dose EBRT with ICRT was 79.3 Gy and for patients receiving hypofractionated EBRT with ICRT was 83 Gy.
Chemotherapy
Chemotherapy was received by 83% of patients and almost all patients received concurrent cisplatin weekly at a dose of 40 mg/m2 (1 patient received carboplatin due to altered renal function). Compliance with chemotherapy was high with 93% of patients receiving the planned 5 cycles of chemotherapy. Chemotherapy was delayed if weekly absolute neutrophil count or platelets were less than 500/mm3 or 100 000/mm3, respectively. Packed cell transfusions were given if haemoglobin was less than 9 g/dL.
Outcomes
The end points were overall survival (OS) and disease-free survival (DFS). Acute haematologic toxicity was evaluated and the worst toxicity noted in the longitudinal variables of haematologic parameters (Hb, total leucocyte count, and platelets) was evaluated during the course of treatment. Reporting was performed according to the RTOG toxicity scale. 20 Patients were followed up every 2 months for the first year, every 3 months during the second year and 6 monthly thereafter. At every follow-up, history, complete physical examination, and relevant investigations (CBC, KFT, LFT, CXR, CECT pelvis) were performed. Information on treatment failure and survival was obtained through institutional records. Treatment failure was documented by positive biopsy, clinical examination, or radiographic findings and classified as in-field (within PTV) or out-of-field (outside PTV).
Statistical analysis
Descriptive statistics for scale variables were obtained using mean with standard deviation or median with interquartile range (IQR) and categorical variables were represented by frequencies with corresponding percentages. Treatment outcome was analysed as a function of overall and event-free survival. Overall survival was defined as the time from initiation of treatment to death or last follow-up. Disease-free survival was measured from initiation of treatment to the first event of treatment failure (local, regional, or metastatic) or death due to any cause. If treatment failure was not detected at last follow-up, the patient was censored at that time point for the analysis of DFS. The uniform 6, 12, 24 months DFS and OS estimates were calculated using the Kaplan-Meier method for different variables and differences were compared using the 2-sided Wilcoxon log rank test. The data were analysed using IBM SPSS for Windows v22 (Armonk, NY, USA). The 2-sided ‘P’ value <.05 was considered as statistically significant. Dosimetric data was extracted and compiled using DVHmetrics v0.3.5 (www.rdocumentation.org/packages/DVHmetrics) available for R software environment (www.r-project.org).
Results
Patient characteristics
Patient characteristics are shown in Table 1. The median follow-up of surviving patients was 30.5 months (IQR: 13-36.25 months). 83% of patients had squamous cell carcinoma histology and 61% had enlarged pelvic nodes. Parametrial score was equally distributed between those with a score less than or equal to 3 and more than 3. 13
Patient and treatment characteristics.
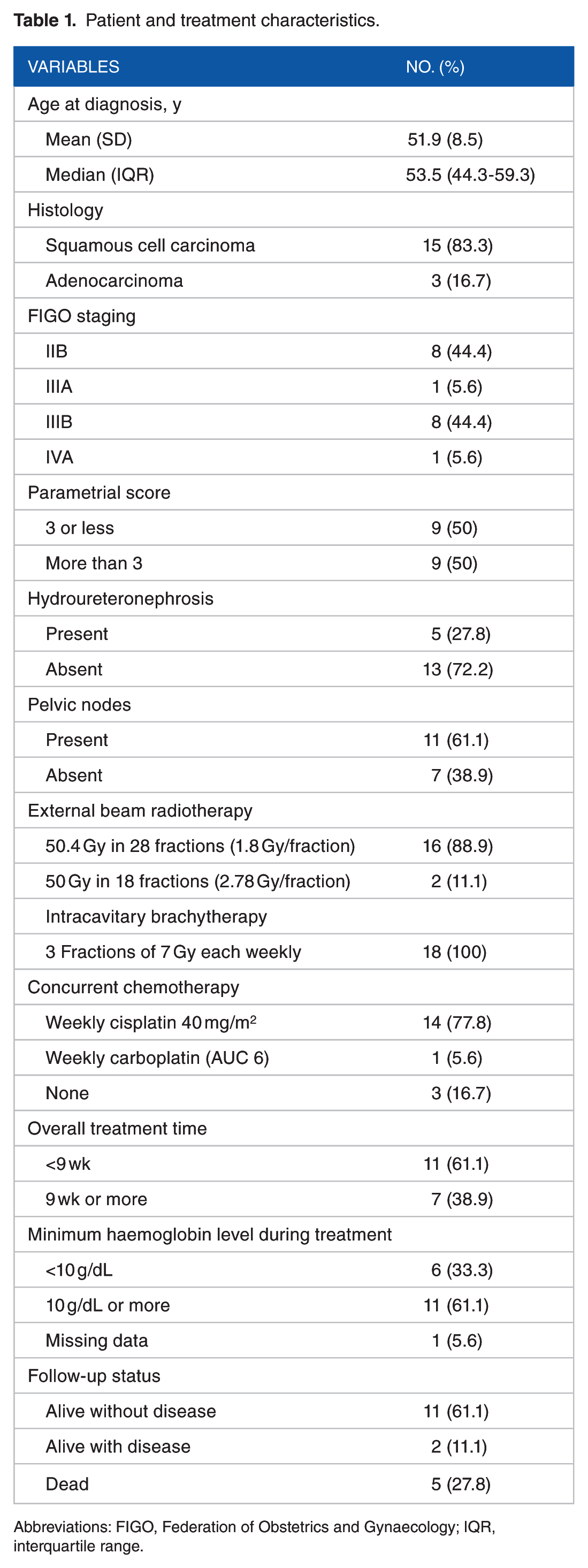
Abbreviations: FIGO, Federation of Obstetrics and Gynaecology; IQR, interquartile range.
Patterns of failure
The characteristics of patients with locoregional and distant failures are shown in Table 2. Out of 7 patients, 5 failed within the cervix (1 of whom also failed synchronously in the supraclavicular nodes and mediastinal nodes). One patient failed in the regional pelvic nodes, whereas 1 failed in the para-aortic and mediastinal nodes. One patient failed by developing peritoneal deposits. In total, there were 4 in-field failures, 2 out-of-field failures, and a single combined in-field/out-of-field failure.
Patterns of failure after treatment.

The histology for all patients was squamous cell carcinoma, except patient 1.
DFS, OS, haematologic toxicity, and results of univariate analysis
The 2-year DFS was 63.3% (95% confidence interval [CI]: 52.8%-72.4%) and OS was 72.2% (95% CI: 62.1%-80.5%), as shown in Figure 2. Mean duration of DFS and OS was 27.6 months (95% CI: 20.7-34.4 months) and 35.6 months (95% CI: 27.7-43.4 months), respectively. None of the variables tested were significantly associated with DFS and OS on univariate analysis (Supplementary File 1, which shows results of univariate analysis). Overall treatment time and minimum haemoglobin level during the course of treatment were also not significantly associated with outcomes. Worst acute haematologic toxicity during the treatment course stratified by RTOG grade is shown in Table 3. 58.8%, 17.7%, and 5.9% of patients experienced RTOG grade 2 toxicity for haemoglobin, total leucocyte count, and platelets count, respectively. None of the patients experienced grade 3 or higher toxicity.

Kaplan-Meier curves for overall survival and disease-free survival.
Acute haematologic toxicity experienced by patients during treatment, stratified by category, and RTOG grade.

Abbreviations: RTOG, Radiation Therapy Oncology Group; TLC, total leucocyte count.
Dosimetric analysis of VMAT plans
The dosimetric parameters of 16 of the 18 VMAT plans, which were prescribed a standard dose of 50.4 Gy in 28 fractions, were analysed as per ICRU-83 recommendations for level 2 reporting. 18 All plans achieved constraints for PTV, CTV, bladder minus PTV, and rectum minus PTV. Constraints for sigmoid colon were not achieved in 15/16 (93.75%) of plans. At least 14/16 (87.5%) plans achieved one constraint for bowel bag. At least 10/16 (62.5%) plans achieved the constraint for left femur head and 13/16 (81.25%) achieved the constraint for right femur head. Detailed graphical (Supplementary File 2, which shows graphical results of dosimetric analysis) and tabulated (Supplementary File 3, which shows tabulated results of dosimetric analysis) results of dosimetric analysis along with compiled dose-volume histograms (DVH) (Supplementary File 4, which shows compiled DVH of each analysed structure and mean ± 2 SD bands) of patients were also generated as per ICRU-83 recommendations. 18
Discussion
Results of several retrospective studies and a few prospective trials have established that IMRT results in equivalent treatment outcomes, reduced gastro-intestinal/genito-urinary (GI/GU) toxicity, and reduced haematologic toxicity, as shown in Table 4.9,11,12,22–24,26,27 Despite these results, controversy persists with routine use of IMRT in this clinical setting owing to concerns of patient movement, target movement, normal structure movement, and tumour shrinkage during treatment.10,28,29 The issue of intrafractional organ motion and consequent target displacement certainly has the potential to lead to insufficient target coverage, which is further amplified by longer delivery times associated with step-and-shoot or sliding window IMRT.10,30 Volumetric-modulated arc therapy treatment delivery has important differences compared with IMRT, namely, speed of treatment delivery with equivalent target coverage and OAR sparing. Faster treatment delivery improves comfort on the treatment couch resulting in less patient movement during treatment delivery and minimizes the impact of intrafraction organ motion (bladder and rectal filling over time) on target coverage, which could increase daily treatment quality. 10 Another potentially important implication of treatment delivery speed is that 2 Gy delivered over 20 minutes is 5% to 10% less biologically effective compared with the same dose delivered over 2 minutes due to the time-dependent recovery of radiation-induced DNA damage in tumour cells.31,32
Details of selected published experiences with IMRT in the treatment of unresected LACC.

3DCRT, 3-dimensional conformal radiation therapy; 5-FU, 5-flourouracil; AP-PA, antero-posterior-postero-anterior; cRT, conventional radiation therapy; CSS, cause-specific survival; CTCAE, Common Terminology Criteria for Adverse Events; CTV, clinical target volume; DFS, disease-free survival; FIGO, International Federation of Gynecology and Obstetrics; Fx, fraction; Gy, Gray; HDR, high dose rate; IG, image-guided; IMRT, intensity-modulated radiation therapy; ITV, internal target volume; LC, local control; LDR, low dose rate; LFFS, local failure-free survival; LRRFS, loco-regional recurrence-free survival; MRI, magnetic resonance imaging; NS, not significant; OS, overall survival; PET, positron emission tomography; PFS, progression-free survival; RTOG, Radiation Therapy Oncology Group; SIB, simultaneous integrated boost; VMAT, volumetric-modulated arc therapy; WP, whole pelvis.
Results from studies using VMAT exclusively for unresected LACC are only just emerging. Chakraborty et al have recently reported early treatment and toxicity outcomes of VMAT delivered with concurrent chemotherapy in an elderly Indian cohort. They found no difference in OS, DFS, and toxicity when comparing patients aged >65 years with those aged <65 years, despite a significant proportion of the elderly cohort not receiving any chemotherapy at all (35.8% vs 2.3%, P = .003). 11 A recent phase 2 multicentre trial by Mell et al allowed VMAT delivery in patients with intact and postoperative cases of cervical carcinoma, however, the proportion of patients receiving it was not specified. They reported significantly reduced rates of grade 3 or higher leucopenia in a preplanned subgroup analysis among patients receiving positron emission tomography–guided image-guided IMRT compared with those receiving IMRT alone (8.6% vs 27.1%, P = .035). 27 Mazzola et al have also reported early clinical outcomes in elderly patients with LACC, treated with simultaneous integrated boost VMAT up to 66 Gy without the use of brachytherapy. They reported 3-year OS and locoregional control of 91% and 80%, respectively, without any acute grade 2 or higher haematologic toxicities. 12
Our results of acute grade 2 haematologic toxicity with VMAT are concordant with those reported by other researchers, with one exception that our patients did not experience grade 3 haematologic toxicity.11,26,27 Also, the pattern of toxicity observed, with anaemia predominating, is similar to previous observations.11,26,33 It is important to emphasize that the haematologic toxicity patterns we observed in our study were reached without optimizing the VMAT plan to achieve a specific constraint for pelvic bone marrow. This finding could be explained by our use of a 3-cm shell optimization structure created around the PTV to improve high- and intermediate-dose conformity, leading to unintentional bone marrow sparing.34,35
There are limitations to this study, first and foremost being its retrospective nature and the inherent biases associated with such an analysis. Our sample size was modest and the small number of treatment failures precludes comparison with other studies. In addition, we were unable to report GI, GU, and skin toxicity. Our study can also be criticized for creating an internal target volume by including 5 mm of the bladder and rectum, as well as including the mesorectum posteriorly and not cropping the CTV from bowel loops. These modifications are the reason why we applied constraints to bladder minus PTV and rectum minus PTV, rather than the whole organ, as it would have been counterintuitive to optimize the whole organ with the internal target volume extending into them. These modifications also explain why sigmoid colon constraints were not achieved. The period of study represents a learning phase of VMAT use, and to assess the impact of our contouring modifications, we have implemented a policy change at our institution after the initial 2-year period that mandates standardized collection of toxicity data and we intend to analyse them along with an expanded cohort size. It is important to recognize that the literature on the use of IMRT in LACC is still evolving with different investigators using varying contouring protocols, dose prescriptions, and choice of concurrent chemotherapy, as highlighted in Table 4.
In conclusion, IG-VMAT is associated with low haematologic toxicity and favourable treatment outcomes in our experience, supporting its safety and efficacy in the treatment of patients with locally advanced cervical cancer. Issues pertaining to intra/interfraction organ motion, optimal contouring, and dose prescription protocols require further research.
Supplemental Material
Supplementary_Material – Supplemental material for Early Clinical Outcomes, Patterns of Failure, and Acute Haematologic Toxicity of Image-Guided Volumetric Modulated Arc Therapy (IG-VMAT) in the Definitive Treatment of Locally Advanced Carcinoma Cervix
Supplemental material, Supplementary_Material for Early Clinical Outcomes, Patterns of Failure, and Acute Haematologic Toxicity of Image-Guided Volumetric Modulated Arc Therapy (IG-VMAT) in the Definitive Treatment of Locally Advanced Carcinoma Cervix by Irfan Ahmad, Kundan Singh Chufal, Irfan Bashir, Chandi Prasad Bhatt, Ram Bajpai, Lalit Sharma and Sandeep Rathour in Clinical Medicine Insights: Oncology
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
IA is the treating junior consultant (radiotherapy), author of the paper, responsible for drafting the manuscript and revising it. He is the guarantor. KSC is the supervising treating senior consultant (radiotherapy) and participated in article formulation, editing and oversight. IB is the treating consultant (radiotherapy) and participated in article editing. CPB is the medical physicist, responsible for generating the radiation treatment plan, performing quality assurance of delivered plan and also participated in article editing. RB is the statistician and performed the analyses reported in this article. He also participated in drafting and revising the article. LS and SR are the radiation technologists, responsible for creating the treatment setup, ensuring reproducible setup and treatment delivery during the course of treatment. They also participated in article editing.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.