
Abstract
Introduction:
The identification of BCR-ABL expression as the defining leukemogenic event in chronic myeloid leukemia (CML) and the introduction of BCR-ABL tyrosine kinase inhibitors in 2001 have revolutionized disease management, leading to a reduction in mortality rates and accordingly an increase in the estimated prevalence of CML.
Case report:
Based on medical records and clinical follow-up, the authors present the case of a Philadelphia chromosome–positive CML patient who developed resistance to imatinib. Quantitative reverse transcription-polymerase chain reaction testing revealed a V280G BCR-ABL mutation.
Discussion and conclusions:
This is the first report describing a new BCR-ABL kinase domain mutation—V280G—that might be associated with resistance to imatinib. Approximately 15% to 30% of patients treated with imatinib discontinue treatment due to resistance or intolerance. More than 90 BCR-ABL mutations were detected so far, conferring variable degrees of drug resistance, with consequent clinical, therapeutic, and prognostic impact.
Introduction
The identification of BCR-ABL expression as the defining leukemogenic event in chronic myeloid leukemia (CML) and the introduction of BCR-ABL tyrosine kinase inhibitors (TKIs) in 2001 have marked a paradigm shift in the management of the disease, leading to a reduction in mortality rates and accordingly an increase in the estimated prevalence of CML.1,2
Imatinib was initially the standard of care for the first-line treatment of CML patients in chronic phase, due to its high long-term response rates and favorable tolerability profile compared with previous standard therapies.2–4
Approximately 15% to 30% (2%-4% annually) of patients treated with imatinib discontinue treatment after 6 years due to resistance or intolerance, particularly in the accelerated and blast phase.1,3–5
Inadequate response to TKI therapy is associated with poor long-term outcome. More than 90 BCR-ABL mutations were detected so far, most frequently the T315I and E255K mutations, conferring variable degrees of drug resistance.5,6
Below, we report the case of a CML patient who developed resistance to imatinib, presenting a new kinase domain mutation—V280G—that has never been described in the literature.
The patient’s anonymity and consent were guaranteed, in agreement with the Declaration of Helsinki. The institutional ethic board approved this report.
Case Report
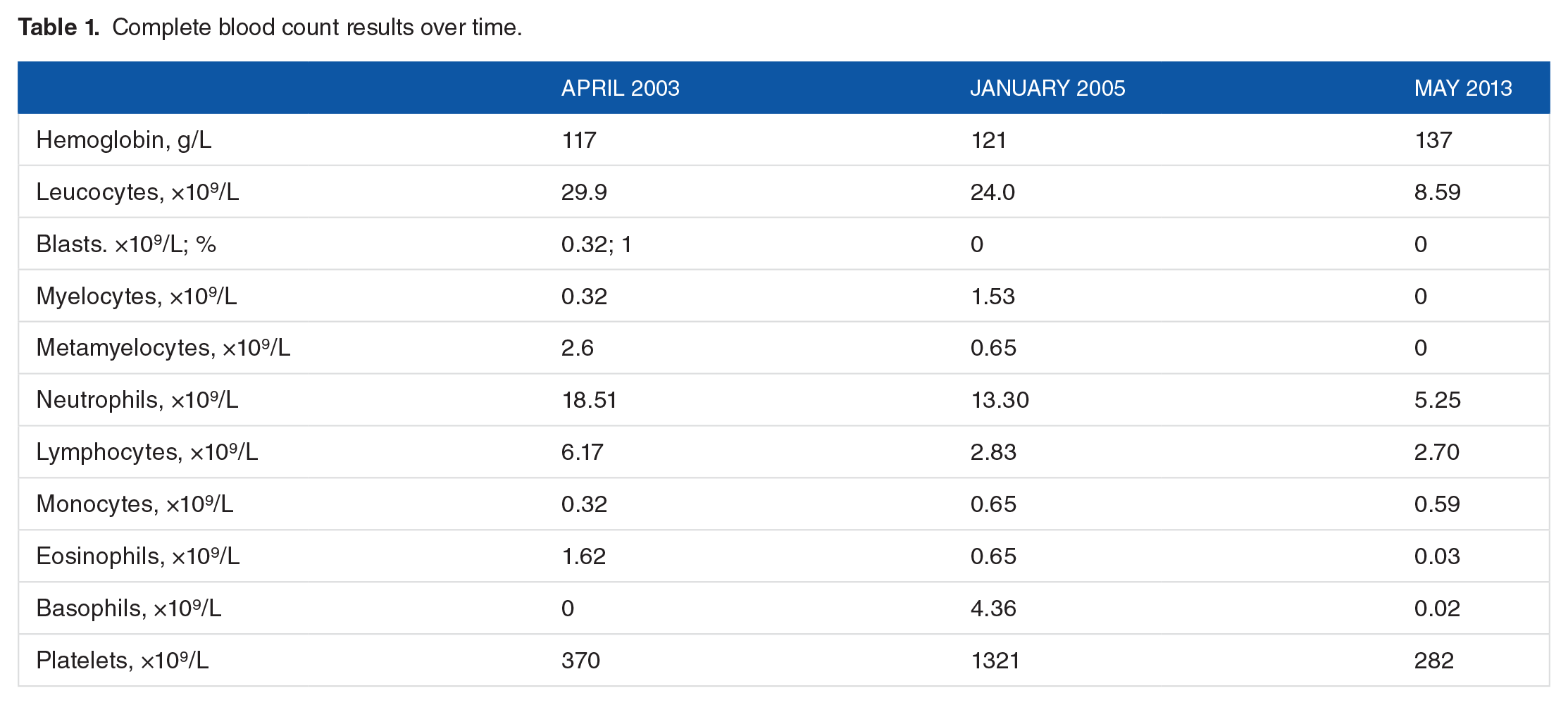
A 75 year-old female patient, leucodermic, referred to oncology consultation, was diagnosed with chronic-phase CML in April 2003 after routine tests, compatible bone marrow study, and cytogenetics with a classic Philadelphia chromosome involving the reciprocal translocation of chromosomes 9 and 22 (BCR-ABL transcripts not evaluated). Complete blood count results, BCR-ABL transcript level evaluation, and treatment options over time are presented in Tables 1 and 2. Medical history was not relevant and physical examination did not reveal splenomegaly or constitutional symptoms. Abdominal ultrasound showed a spleen with 10.0 × 5.9 cm. She was given an intermediate-risk Sokal score 7 (0.84) and Hasford score 8 (931.5), but low-risk EUTOS (European Treatment and Outcomes Study) score 9 (40). At that time, she was started on hydroxyurea 500 mg/day and interferon alpha interferon 3 million units/5 times per week, with a complete hematologic response (CHR) 3 months later. Repetition of the bone marrow study in December 2003 showed a complete cytogenetic response (CCyR), and 1 year after diagnosis BCR-ABL was positive (not quantified).
Complete blood count results over time.
BCR-ABL transcript level evaluation and treatment prescription over time.

Abbreviations: alpha-IFN, interferon alfa; HU, hydroxyurea.
The patient continued initial therapy until January 2005 when she revealed signs of disease progression and therapeutic failure. Abdominal ultrasound did not reveal splenomegaly. She was started on imatinib at a dose of 300 mg/day, obtaining a partial cytogenetic response (BCR-ABL p210—4.3% on the International Scale [IS]) in June 2007. A marrow study revealed some degree of fibrosis, with no disease infiltration.
In January 2010, BCR-ABL p210 was positive (maximum 0.98%) and an increase (maximum 2.07%) was detected by December 2010, which motivated her referral to our hematology consultation by February 2011. Although the bone marrow was maintained in remission, the BCR-ABL p210 transcript number was persistently increased (maximum 2.63%), which led us to increase the imatinib dose from 300 to 400 mg/day.
After 6 months of imatinib dose increase, the number of BCR-ABL p210 transcripts decreased (0.53%) and, given the good hematologic and molecular responses, the imatinib dose was maintained.
By October 2012, although the patient maintained a CHR, a major molecular response was never achieved, with a progressive increase in the BCR-ABL transcripts (2.74%). As a result of the failure to obtain an adequate molecular response, resistance to imatinib was investigated. We performed a nested quantitative reverse transcription-polymerase chain reaction (qRT-PCR) and bidirectional sequencing (as previously described 10 ) to perform a BCR-ABL kinase domain mutational analysis. This study showed a mutation on amino acid 280, resulting in the substitution of valine (V) by glycine (G), present in all transcripts (c.839T>G V280G mutation) (Figure 1), and negative in DNA samples from the gum mucosa.

BCR-ABL tyrosine kinase domain mutation analysis in peripheral blood revealed c.839T>G (V280G mutation), in which GTG→GGG (valine to glycine).
On February 2013, BCR-ABL p210 was positive (8.0%). imatinib was discontinued due to resistance and the patient was started on nilotinib 400 mg/twice a day.
In May 2013, the patient revealed a good clinical and laboratorial response to therapy, with CCyR and CMR.
Currently, the patient maintains the same nilotinib dose, without evidence of loss of hematologic or molecular responses and with a good tolerability.
Discussion and Conclusions
Tyrosine kinase inhibitor therapy with imatinib, dasatinib, or nilotinib has resulted in a remarkable improvement in clinical outcomes for CML patients diagnosed in chronic phase. The optimization of monitoring methods and the identification of factors associated with response and long-term outcomes have thus been a major clinical research focus, contributing to recent updates to clinical practice guidelines. 2
In the case presented here, the patient had been previously diagnosed and followed in another hospital center, and there was no registry in the process file about the reason why it was decided to start treatment with a subtherapeutic imatinib dose. Although not consensual in the literature,11–16 this probably contributed to a worse molecular response and to imatinib treatment failure, even after increase of the dose in 2011, when the patient was referred to our consultation. At the moment, it is not specified which of the 3 TKIs currently approved for the first-line treatment of chronic-phase CML is preferred, and although no evidence from clinical trials is available to support the superiority of second-generation TKIs over imatinib with respect to survival outcomes, they induce the achievement of faster and deeper molecular responses, associated with better long-term outcomes, less progression to advanced phases, and possibility of treatment discontinuation.17–20
International Randomized Study of Interferon versus STI571 (IRIS) trial has demonstrated that imatinib induces high durable responses and improves survival in a large proportion of patients with newly diagnosed chronic phase compared with interferon.17,21 However, DASISION (DASatinib versus Imatinib Study In treatment-Naive CML patients) and ENESTnd (Evaluating Nilotinib Efficacy and Safety in Clinical Trials–Newly Diagnosed Patients) studies showed that dasatinib and nilotinib induce superior cytogenetic and molecular responses and lower rates of progression to accelerated or blast phase compared with imatinib.19,20
Although imatinib is still recommended as a reasonable first-line option for patients with newly diagnosed chronic phase, the selection of first-line TKI depends on the risk score (Sokal and Hasford), physician’s experience, toxicity profile, patient’s age, tolerance and adherence to therapy, as well as comorbidities. 17
Allogeneic hematopoietic cell transplant, which was the treatment of choice for CML before the advent of TKI therapy, is now generally reserved for patients in chronic phase resistant to multiple or unable to tolerate TKIs, those who have the T315I mutation and who are not suitable for prolonged ponatinib therapy, or for those progressing to the accelerated or blast phase. 17
Because most CML patients treated with imatinib achieve CCyR (CCyR roughly corresponds to a BCR-ABL level of <1% IS), both the National Comprehensive Cancer Network (NCCN) and the European Leukemia Net (ELN) guidelines emphasize adequate monitoring and measurement of residual disease through sensitive molecular methods, such as quantification of BCR-ABL transcript levels and qRT-PCR, to ensure that patients are meeting the treatment milestones.20,22–25
Although most of these patients respond to first-line TKI therapy, the use of TKIs is hindered by the development of resistance or intolerance in some patients, resulting in a loss of response or discontinuation of treatment. This is most commonly associated with the acquisition of resistance-conferring kinase domain point mutations within BCR-ABL, which prevent the binding of imatinib to the kinase domain, additional chromosome abnormalities to the Philadelphia chromosome, and/or mutations in genes such as ASXL1, TET2, RUNX1, DNMT3A, EZH2, and TP53, among others.1,22,26 According to ELN 2013 criteria, it is recommended to perform a mutational analysis in these cases.20,27 The recommended methodology is direct sequencing, although it may be preceded by screening with other techniques, such as denaturing high performance liquid chromatography.25,26
Next-generation deep sequencing, complemented with bioinformatics support, mass spectrometry, and digital PCR are emerging as promising techniques to ensure reliable detection of BCR-ABL mutations, allowing early therapy switch and selection of the most appropriate therapy.27,28
Current data support that for CML patients who fail treatment goals, with primary resistance or intolerance to imatinib, hematologic disease recurrence, or emergent BCR-ABL kinase domain mutations, imatinib dose escalation may not be sufficient to control the disease, and substitution with another TKI will be necessary.3,17,24,26,27,29 Patients should be carefully evaluated for alternative treatment options, including dasatinib, nilotinib, bosutinib, and ponatinib, as well as the non-TKI salvage agent omacetaxine mepesuccinate. Treatment selection is based on factors such as the patient’s disease state, prior therapies, type of mutation, comorbidities, treatment toxicity, and therapy goals.1,3
A literature review shows that pre-existing mutations at baseline confer a more aggressive disease phenotype and patients with advanced stages of the disease often do not respond to therapy or relapse.5,6,17
There is no reference in the literature on the association between CML/other pathology and the c.839T>G V280G mutation, as detected in this case. Gruber et al 30 have used the V280G variant in their study about the biological significance of aberrant activation -induced cytidine deaminase expression in a murine model of BCR-ABL1–driven B-cell lineage acute lymphoblastic leukemia, but this was based on the results presented in a previous publication of Soverini et al. 6 However, Soverini et al 26 described in 2011 a mutation in the same codon position, involving different amino acids, associated with imatinib resistance in CML patients. The mutation presented in this case report causes a substitution of a valine by a glycine at amino acid 280, in the kinase active domain, being the only alteration found in this patient after BCR-ABL mutation analysis. A DNA sample of gum mucosa was negative for this type of mutation, which allowed us to conclude that acquired V280G variant was indeed a characteristic of the leukemic clone, rather than a polymorphism. This finding led us to hypothesize that this mutation might be associated with de novo resistance to treatment with imatinib. The favorable clinical and hematologic parameters to nilotinib also support this statement. However, studies in a larger population and of functional character should be performed to evaluate the prevalence of this mutation and its association with imatinib resistance and to determine whether this mutation can be grouped with other similar mutations to better indicate nilotinib as a first-choice treatment. It will also be useful to have functional analyses to better characterize this mutation and show whether it affects the ability of imatinib to bind or inhibit BCR-ABL.
Regular monitoring of BCR-ABL levels, effective management of toxicities, and patient education on adherence to TKI therapy are essential to provide optimal treatment.
The possibility of resistance to treatment should promote a rational development of alternative, synergistic, and potentially curative strategies.
The more complete knowledge about the disease and its mutational characterization will allow us to control the disease course.
Footnotes
Acknowledgements
The authors would like to thank Prof Susana Silva and Prof Ana Gírio for intellectual input and advice.
Peer review:
Seven peer reviewers contributed to the peer review report. Reviewers’ reports totaled 1503 words, excluding any confidential comments to the academic editor.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
APA performed laboratorial and data analysis and wrote the manuscript; AR followed the patient, performed data analysis, and reviewed the manuscript; CA followed the patient and reviewed the manuscript; MDA reviewed the manuscript; PT performed the laboratory analysis; and FL reviewed the manuscript.