
Abstract
Background:
Effective and reliable venous access is one of the cornerstones of modern medical therapy in oncology.
Materials and methods:
This is a prospective observational study, which collected data of patients who require “PORT” catheter insertion for any cancer, at a tertiary care oncology hospital in Ahmadabad, Gujarat, India, during a 2-year period.
Aims and objectives:
The main objective of this study was to study the various complications and outcomes related to “PORT” catheters.
Results:
“PORT” catheter was inserted in 100 patients and was most commonly used in solid malignancies (n = 86, 86%), followed by hematologic malignancies (n = 14, 14%). Among the solid malignancies, breast cancer (38, 38%) was the most common underlying disease, whereas among the hematologic malignancies, acute lymphoblastic leukemia (6, 6%) was the most common underlying disease for “PORT” catheter insertion. Chemotherapy was started on the first day of “PORT” catheter in 74% of patients in the “PORT” study group. The various complications developed in the “PORT” study group in the descending order are as follows: 4 patients (4%) developed early infection (⩽30 days after “PORT” placement), 4 (4%) late infection (⩾30 days after “PORT” placement), 4 (4%) bloodstream infection, 2 (2%) local skin infection at the “PORT” insertion site, 2 (2%) dislodgment of the “PORT” catheter, 2 (2%) fracture of the “PORT” catheter, and 1 recurrent pleural effusion. One patient (1%) developed thrombosis as the complication of “PORT” catheter insertion.
Conclusions:
The most disturbing aspect of treatment for a patient with cancer is multiple painful venipunctures made for administration of cytotoxic agents, antibiotics, blood products, and nutritional supplements. The focus of this prospective observational research is to study the various underlying diseases for which “PORT” catheter is needed in different solid and hematologic malignancies and the various complications and outcomes in pediatric and adult patients with cancer.
Introduction
Effective and reliable venous access is one of the cornerstones of modern medical therapy in oncology. 27 The management of a patient with cancer demands stable venous access that is used for a wide range of underlying diseases, including chemotherapy, blood product and antibiotic administration, and fluid resuscitation. The use of long-term venous access devices (LTVADs) or central venous catheters (CVCs) can also decrease patient anxiety associated with repeated venipunctures. The number and variety of LTVADs used in oncology practices are as follows:
Peripherally inserted central catheters (PICC);
Hickman line (cuffed or noncuffed tunneled) CVCs;
Subcutaneous implanted “PORT” catheters. 1
Peripherally inserted central catheters, Hickman, and “PORT” devices provide reliable and safe intravenous access to a variety of underlying diseases in oncology. 2 Peripherally inserted central catheters, Hickman, and “PORT” devices are frequently used in oncology patients to deliver chemotherapy as well as other intravenous medications, fluids, and total parenteral nutrition. 3
The implantable “PORT” consists of a catheter attached to a reservoir that is implanted into a surgically created pocket on the chest wall or upper arm. Some patients require fluoroscopic guidance for “PORT” insertion. 25 A needle is inserted through the septum of the “PORT” to access the reservoir.
Advantages include less interference with daily activities, less frequent flushing, and reduced risk of infection. Disadvantages include the need for needle insertion, increased discomfort, and risk of extravasation. These devices are expensive and are more difficult and time-consuming to insert and remove.
Although the initial cost of central venous access port devices (CVAPD) is high, a case-control study comparing durability and cost of CVAPD and external catheters demonstrated long-term economic benefit for CVAPD for use beyond 6 months due to lower ongoing maintenance costs. 4 Implanted venous access devices can be inserted either peripherally near the antecubital fossa (Passport) or centrally into the subclavian or jugular vein (CVAPD). Peripheral “PORT” has a lower risk of infection than CVAPD, and their insertion involves a minimal risk of pneumothorax and hemothorax. However, they have a shorter useful lifetime than CVAPD, and there is an increased risk of venous sclerosis following the use of cytotoxic agents, which makes them unsuitable for cancer patients receiving long-term chemotherapy.5,27 Increasing age, male gender, and open-ended catheter use were significant risk factors reducing survival of totally implantable venous access devices as determined by univariate and multivariate analyses. 28
The intravascular segment of “PORT” catheter is made of similar material to Hickman and Groshong catheters. The thick injection membrane of the system is housed in a titanium or plastic case, which is surgically implanted under the skin’s subcutaneous tissue, usually on the patient’s chest wall or upper arm. It is then accessed with a special noncoring Huber-type needle. This provides a more acceptable cosmetic option and allows the patient to swim or bathe, which are restricted practices with externally exiting catheters. “PORT” kits are expensive, time-consuming to insert, and the accessing needles have a fine bore (6F or 7F) that restricts flows for blood transfusion or venesection. The novelty of this research is that this is the first Indian study with a maximum number of patients with most number of cancer patients from a tertiary oncocare unit from the developing countries.
Aims and Objectives
To study the various complications and outcomes related to “PORT” catheters;
To study the various underlying diseases of “PORT” catheters in different solid and hematologic malignancies in the pediatric and adult patients with cancer attending to the Department of Medical & Pediatric Oncology.
Materials and Methods
This is a prospective observational study, which collected data of patients diagnosed with any cancer, at a tertiary care oncology hospital in Ahmadabad, Gujarat, India, during a 2-year period (August 2013 to August 2015). Patients of all age and sex, presenting to Department of Medical & Pediatric Oncology and hematology at Gujarat Cancer & Research Institute (GCRI), were included.
The data were collected from the Department of Anesthesia, Department of Surgical Oncology, and institutional (GCRI) websites, from patients admitted in the Department of Medical & Pediatric Oncology. Patients were interviewed using a detailed questionnaire regarding their age, sex, clinical symptoms, and treatment received outside GCRI. A particular note was made of a history of any thromboembolic disease, bleeding disorders, and whether the patient was ever treated for that.
The data were collected for underlying diseases of “PORT” catheter in various malignancies. The data were collected from the patient, for the complications related to “PORT” catheter, directly through clinical symptoms, examination findings, and specific investigations, such as blood culture and differential time to positivity, Doppler of the affected part, and outcomes of treatment.
In our center, “PORT” catheter insertion was performed under anesthesia, in the operation theater.
The study was approved by the Ethics Committee of GCRI, Ahmadabad, Gujarat, India. Written informed consent was obtained from the patients or the parent/guardian for publication of the clinical details in this report.
Inclusion criteria
All patients with cancer presenting to medical and pediatric oncology and hematology;
All histopathologically confirmed patients with cancer;
All the stages and performance status.
Exclusion criteria
Abnormal coagulation profile (bleeding diathesis);
Platelet count <15 000/mm3;
Did not consent.
Definitions
Catheter-related infection
Central line–associated bloodstream infection (BSI) refers to a BSI that appears in the presence of a CVC or within 48 hours of removal of a CVC and which cannot be attributed to an infection unrelated to the catheter; it is defined by the National Healthcare Safety Network for the purpose of surveillance of health care–associated infection.
Catheter-related thrombosis
Catheter-associated thrombosis is defined as a mural thrombus extending from the catheter into the lumen of a vessel and leading to partial or total catheter occlusion with or without clinical symptoms.
Results and Observations
In this prospective observational study, patients of all age and sex, presenting to Department of Medical & Pediatric Oncology, were included, with a diagnosis of any cancer, at GCRI, a tertiary care oncology hospital in Ahmadabad, Gujarat, India, during a 2-year period (August 2013 to August 2015). The data were collected for the underlying diseases, complications, and outcomes of “PORT” catheter in various malignancies, from the patients admitted at the Department of Medical & Pediatric Oncology, bone marrow transplantation unit, surgical oncology, and Department of Anesthesia. Patients were interviewed using a detailed questionnaire regarding their age, sex, clinical symptoms, and treatment received outside GCRI.
Distribution of the study population
A total of 652 patients were enrolled as the study population for the LTVADs study, of which 352 (53.98%) required PICC insertion, 200 (30.67%) required Hickman catheter insertion, and 100 (15.33%) required “PORT” catheter insertion as part of their comprehensive management strategy in our cancer center.
Age and sex distribution of the study group
Of the 100 patients in the “PORT” study group, 17 (17%) were in the less than 14 years age group (pediatric population), 81 were in the adult (14-65 years) age group (81%), and 2 were in the geriatric age group (2%); 41 were men (41%) and 59 were women (59%).
Diagnosis and various underlying diseases of the “PORT” catheter in patients with cancer
In our study group, “PORT” catheter insertion was most commonly used in patients with solid malignancies (n = 86 [86%]), followed by (n = 14 [14%]) hematologic malignancies. Among the solid malignancies, breast cancer (n = 38 [38%]) was the most common underlying disease, whereas among the hematologic malignancies, acute lymphoblastic leukemia (ALL) (n = 6 [6%]) was the most common underlying disease for “PORT” catheter insertion (Figure 1 and Table 1).

Various underlying diseases of the “PORT” catheter in hematologic and solid malignancy groups. ALL indicates acute lymphoblastic leukemia; GCT, germ cell tumor; NB, neuroblastoma; OS, osteosarcoma; RMS, rhabdomyosarcoma; STS, soft tissue sarcoma.
Various underlying diseases of the “PORT” catheter in solid and hematologic malignancies.
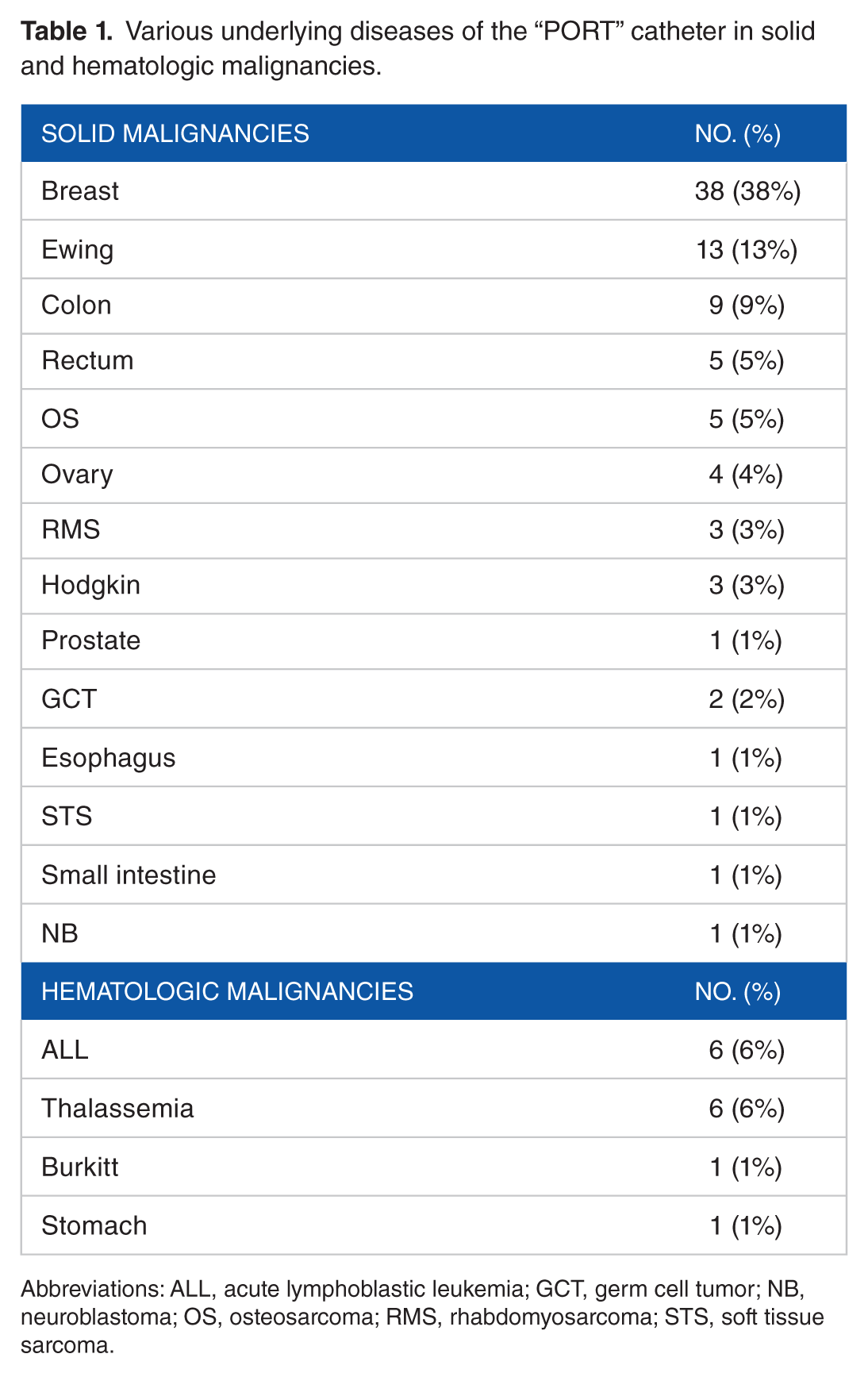
Abbreviations: ALL, acute lymphoblastic leukemia; GCT, germ cell tumor; NB, neuroblastoma; OS, osteosarcoma; RMS, rhabdomyosarcoma; STS, soft tissue sarcoma.
Antibiotic prophylaxis
All the 100 patients in the “PORT” study group received prophylactic antibiotics in the form of single-dose ceftriaxone 1 g intravenously, 1 hour before the insertion of “PORT” catheter.
Day of start of chemotherapy
Of the 100 patients in the “PORT” study group, 74 (74%) were started on chemotherapy on the first day of catheter insertion, 12 (12%) on second day of catheter insertion, 6 (6%) on third day of catheter insertion, and 4 (4%) each on fourth and fifth days of catheter insertion (Figure 2).

Day of start of chemotherapy in the “PORT” study group.
Distribution of infection, catheter displacement, catheter fracture, recurrent pleural effusion, and thrombosis in the “PORT” study group
Of the 100 patients, 4 (4%) developed early infection (⩽30 days after “PORT” placement) and another 4 (4%) developed late infection (⩾30 days after “PORT” placement), 4 (4%) developed BSI, and 2 (2%) developed local skin infection at the “PORT” insertion site. Of the 100 patients, 2 (2%) developed displacement of the “PORT” catheter, 2 (2%) developed fracture of the “PORT” catheter, 1 patient developed recurrent pleural effusion because of direct catheter tip in pleural cavity, and 1 (1%) developed thrombosis as the complication of catheter insertion in the “PORT” study group (Table 2).
Distribution of cases of infection, catheter displacement, catheter fracture, recurrent pleural effusion, and thrombosis in the “PORT” study group.

Discussion
The most disturbing aspect of treatment of a patient with cancer is multiple painful venipunctures made for administration of cytotoxic agents, antibiotics, blood products, and nutritional supplements. To overcome the problems of arteriovenous fistulae, peripherally inserted silicone catheters and implantable “PORTs” have been tried with varying success. The introduction of CVCs in the 1980s significantly improved the quality of life (QOL) of oncology patients.6-9
The focus of this prospective observational research is to study the various underlying diseases of “PORT” catheter in different solid and hematologic malignancies and the various complications and outcomes in pediatric and adult patients with cancer attending the Department of Medical & Pediatric Oncology, over a 24-month period (August 2013 to August 2015), in a tertiary oncocare center situated in Western India.
Following an extensive search of the literature, it became evident that there were very few research studies from the Indian and Asian subcontinents focusing specifically on “PORT” lines within oncology cohorts, and to the best of our knowledge, this may be the largest prospective study in the Indian literature.
In this study, an attempt is made to compare the study results with the previous studies from the published literature, with specific findings of the particular group from our study. Most of the studies in the literature are retrospective in nature, and this study with robust number of patients and data may be helpful for future comparative studies.
This study results reported similar demographics to those of other published studies. Of the studies that reported gender, all studies showed their cohort as having a slight predominance of men over women, and that most were older than 50 years. A study by Kumar et al 10 shows that there is male predominance for the indication of LTVADs.
A study by Patel et al 11 shows that the median age for “PORT” catheter insertion is 24 years, but in our study, the median age for “PORT” catheter was 36 years. The discordance may be due to the differences in the selection of the patients.
This study’s cohort was positioned in an oncology department; thus, chemotherapy was the primary reason for “PORT” catheter insertion, and this was reflected in the studies by Yap et al 3 and Cheong et al. 12 Most of the patients have PICC, Hickman, and “PORT” catheter insertion for intravenous (IV) chemotherapy, antibiotics, pain management, total parenteral nutrition, hydration, apheresis and life support treatments, or IV access.3,12-14
“PORT” catheter was inserted in 100 patients and most commonly used in solid malignancies (n = 86 [86%]), followed by hematologic malignancies (n = 14 [14%]). Among the solid malignancies, breast cancer (38 [38%]) was the most common underlying disease, whereas among the hematologic malignancies, ALL (6 [6%]) was the most common underlying disease for “PORT” catheter insertion. All the 100 patients in the “PORT” study group received prophylactic antibiotics before the insertion of “PORT” catheter. Chemotherapy was started on the first day of “PORT” catheter in 74% of patients in the “PORT” study group. The various complications in our study as compared with other studies 31 in the “PORT” study group in descending order are as follows: 4 patients (4%) developed early infection, 4 (4%) developed late infection,22,23,26,30 4 (4%) developed BSI, 2 (2%) developed local skin infection at the “PORT” insertion site, 2 (2%) developed dislodgment of the “PORT” catheter, 2 (2%) developed fracture of the “PORT” catheter, 1 (1%) developed thrombosis, 24 and 1 developed recurrent pleural effusion. 29
Most of the literature is retrospective in nature, and the largest of this type is the study by Aparna et al in the pediatric population, and our results are comparable with this study and other smaller Indian studies. We compared our results with some of the important Indian studies, which are shown in Table 3.
Comparison of “PORT” study results with the various Indian studies.

The present “PORT” study results are also comparable with the following 2 international studies: one is the study from Memorial Sloan Kettering Cancer Center on 680 patients between June 1987 and May 1989, and another is a prospective study by Vardy et al 19 on 110 consecutive patients who had insertion of 111 subclavian CVAPD; the “PORT” study results were comparable (Table 4).
Comparison of “PORT” study results with international studies.
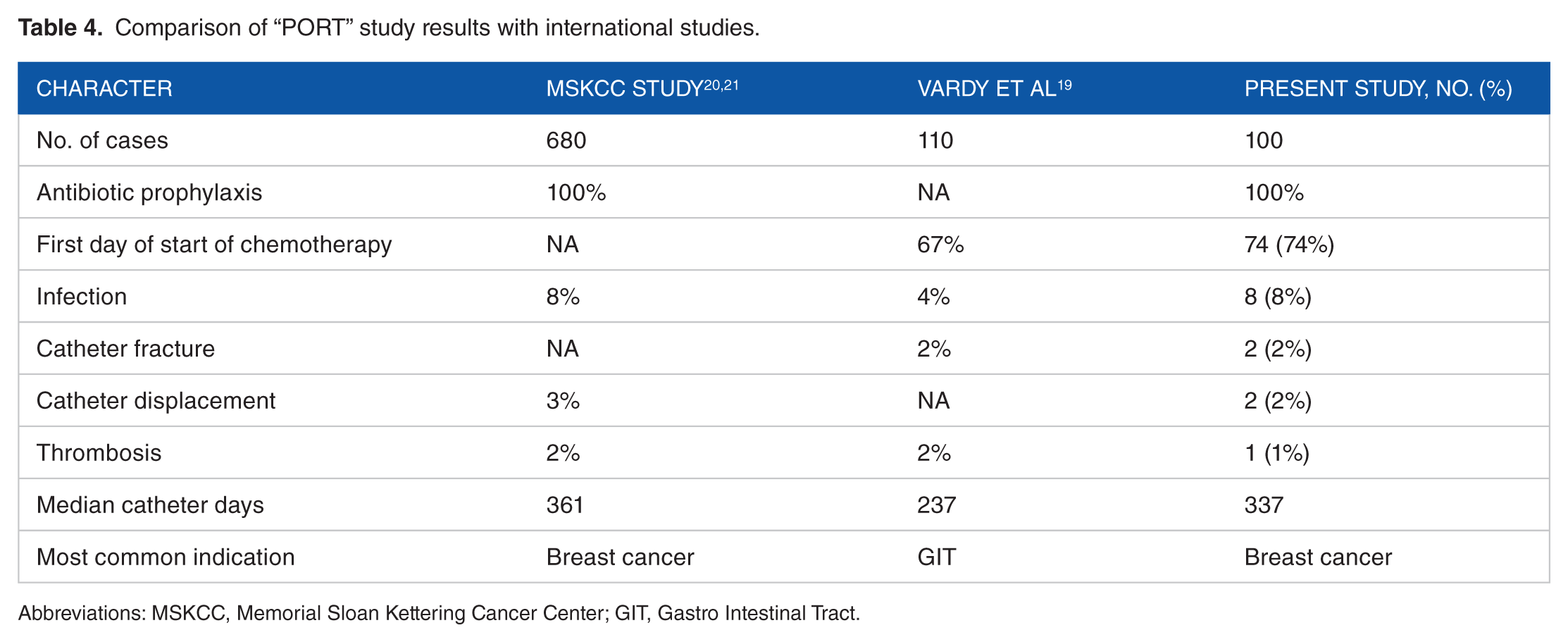
Abbreviations: MSKCC, Memorial Sloan Kettering Cancer Center; GIT, Gastro Intestinal Tract.
Future Perspectives
As this study stands out to be one of the major prospective observational study and most of the data at present in Indian setup are retrospective in nature, this study can be used for future prospective observational studies. It provides suggestions for future medical researchers to incorporate QOL measures, details of different infections, drug sensitivity, and advanced technological methods, such as Groshong catheters with different designs and materials with proper methods of education, to the patient and his or her relative for catheter care.
Footnotes
Acknowledgements
The authors are thankful to Departments of Surgical Oncology and Anesthesia staff of GCRI, Ahmadabad, for their constant support during the study tenure of this research work.
Peer review:
Four peer reviewers contributed to the peer review report. Reviewers’ reports totaled 1510 words, excluding any confidential comments to the academic editor.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
IM conceived and designed the experiment, made critical revisions, and approved the final version. IM and AP analyzed the data and wrote the first draft of the manuscript. IM, AP, MS, AA, HP, and SP contributed to the writing of the manuscript. MS, AA, HP, and SP agree with the manuscript results and conclusions. IM, MS, HP, and SP jointly developed the structure and arguments for the paper. All authors reviewed and approved the final manuscript.
Ethics
Written informed consent was obtained from all the patients for the publication of this original research and accompanying images. The ethics committee of the GCRI approved the study.