
Abstract
Background:
Melanosis coli, a brown discoloration of colonic mucosa, is considered as a benign condition mainly observed in patients under chronic anthranoid laxatives. Recent data link this condition with an increased adenoma detection rate. Moreover, its tumorigenic potential and possible association with the development of colorectal cancer remains uncertain. We conducted this study to compare the polyp detection rate and colorectal cancer diagnosis in patients with melanosis against matched control group without melanosis.
Patients and methods:
A retrospective single-center study. Patients diagnosed with melanosis coli on colonoscopy over a 15-year period were included. Each melanosis coli patient was matched with three controls by age, gender, setting (inpatient/outpatient), and procedure’s indication. Polyp detection rate and diagnosis of colorectal cancer were recorded and compared between the groups before and after adjustment for bowel preparation.
Results:
A cohort of 718 patients with melanosis and 2154 controls were included. The polyp detection rates were 33.4% and 21.8% of melanosis and control groups, respectively (P < .001). Melanosis coli, however, was associated with less diagnosis of colorectal cancer than controls (0.3% vs 3.9%; P < .001). In multivariate analysis, melanosis diagnosis on endoscopy was significantly associated with higher polyp detection rate (odds ratio [OR] = 1.986, 95% confidence interval [CI]: 1.626-2.425; P value < .01).
Conclusions:
Melanosis coli is not associated with increased diagnosis of colorectal cancer. It is associated, however, with enhanced polyp detection likely due to chromo-endoscopy-like effect.
Background
Melanosis coli (MC) is a black or brownish discoloration of the colonic mucosa that results from accumulation of lipofuscin pigment in macrophages within the lamina propria.1–3 MC is generally diagnosed by inspection of colonic mucosa during colonoscopy. However, to rule out true melanosis, a microscopic examination is mandatory.4,5 MC may affect the entire colon or involve a single or short bowel segments. The association between MC and long-term use of anthraquinone laxatives was firmly established by previous studies.6–8 In developed countries, these laxatives are widely used and high rates of MC are identified. 9 MC, however, is not pathognomonic for anthraquinone use and has been reported in patients with chronic colitis.10,11
A concern about a possible link between MC and the development of colorectal cancer (CRC) has long been an issue of interest and controversy.12,13 Only few studies have reported a link between CRC and laxative use or MC.14,15 Nonetheless, few recent studies have shown no association with CRC.4,16–18
MC is usually reported to spare adenomas and carcinomas.19–21 Some, but not all, hyperplastic polyps were spared in one report, 20 whereas there is no published data regarding serrated adenomas. This effect permits enhanced visibility and improved observation of polyps in the dark background mucosa, probably linking MC with increased polyp detection rate (PDR). Whether this association signifies also a causal relationship due to an oncogenic effect of MC is still unknown.
This study compares patients with MC with appropriately matched controls to aid on clarifying and better understanding the possible association between MC, PDR, and CRC.
Methods and Settings
In this retrospective study, we included a large cohort of patients who underwent colonoscopy over a 15-year period at the gastroenterology department at the Hillel Yaffe Medical Center, a university-affiliated hospital in Israel. All patients’ data were collected from our department’s computerized record system. MC was defined as a gross appearance of brown or black discoloration of the colonic mucosa during colonoscopy. We conducted a search on endoscopy electronic reports and identified all patients with a diagnosis of MC (MC group). Another group of control patients (at a 1:3 ratio), based on age, sex, setting, and procedure indication matching, were included for final analysis. We determined the adequacy of bowel preparation according to endoscopy reports (adequate/inadequate). Cecal intubation rate, PDR, and diagnosis of CRC were compared between groups. We performed subgroup analysis and compared these parameters in both groups among patients with adequate bowel preparation only. Multivariate analysis was used to determine the effect of the independent parameters on PDR. The study was approved by our center’s local ethics committee.
Statistical analysis
This statistical analysis is dealing with cohort of large data of patients who underwent colonoscopy in a 15-year interval at our institution; of them, 718 patients are with melanosis (study group). We used the Propensity Score Matching in R program version 3.3 to divide the total cohort to 1:3 ratios (study: control group). From this matching, we created 3 control groups. Each of the control groups includes 718 patients who did not have Melanosis. Differences between the 4 groups in the categorical parameters were presented by Pearson Chi-square and Fisher exact test. One-way analysis of variance (ANOVA) was used for the quantitative parameter (age).
As the 3 control groups were statistically similar to the independent parameters, we unite them into one group of control group.
Multivariate logistic regression model was used to determine the effect of the independent parameters associated with PDR. SPSS version 25 was also used for statistical analysis. P < .05 was considered as significant.
Results
We included a large cohort of 50 128 patients who underwent colonoscopy at our hospital. We searched endoscopy reports and identified 718 patients (1.4%) with MC diagnosed during the study period. A matched group of 2154 control patients (at 1:3 ratio) were included for final analysis. Baseline characteristics of both groups were similar and are provided in Table 1. The overall mean age was 64.8 years (range: 18-102 years), and subjects were predominately females (74.4%). The vast majority of the procedures (85.8%) were performed in the outpatient setting. The most common indications for colonoscopy were constipation (23.5%), abdominal pain and diarrhea (20%), rectal bleeding (14.5%) and anemia (9.8%). Procedures’ indications did not differ significantly between groups.
Baseline characteristics of melanosis and control patients.

Abbreviations: CRC, colorectal cancer; FOBT, faecal occult blood test; IBD, inflammatory bowel disease.
The PDRs were 33.4% and 21.8% of melanosis and control groups, respectively (P < .001). MC, however, was associated with less diagnosis of CRC than matched control group (0.3% vs 3.9%; P < .001). A subgroup analysis of patients with adequate bowel preparation only revealed similar results with increased PDR (34.1% vs 21.3%, P < .001), but a reduced diagnosis of CRC (0% vs 4%; P < .001) in MC patients was compared with controls (Table 2). To eliminate the effect of past colonoscopy on PDR and CRC diagnosis, and for accurately estimating the CRC diagnosis, we excluded all repeated colonoscopies in the melanosis group and included 589 patients (82%) with first-time colonoscopy only. We created a new, fully matched, first-time colonoscopy control group (1767 patients, at a 1:3 ratio). No prominent changes in trends or results for PDR (32.1% vs 22.1%; P < .001) and CRC diagnosis (0.3% vs 3.7%; P < .001) were recorded in the melanosis and control groups, respectively.
Endoscopic findings: complete examination rate, polyp detection rate, and cancer diagnosis in both groups.

In multivariate analysis, older age (odds ratio [OR] = 1.039, 95% confidence interval [CI]: 1.030-1.048; P value < .001), female sex (OR 1.438, 95% CI: 1.171-1.766; P value =.01), inpatient setting (OR = 1.487, 95% CI: 1.099-2.012), positive fecal occult blood test or personal polyp history as indication for colonoscopy (OR = 1.825, 95% CI: 1.276-2.611; P value = .01 and OR = 5.464, 95% CI: 3.865-7.723; P value < .01, respectively), and melanosis diagnosis on endoscopy (OR = 1.986, 95% CI: 1.626-2.425; P value < .01) were significantly associated with PDR (Table 3).
Effect of the independent parameters associated with polyp detection rate (PDR); a multivariate analysis.
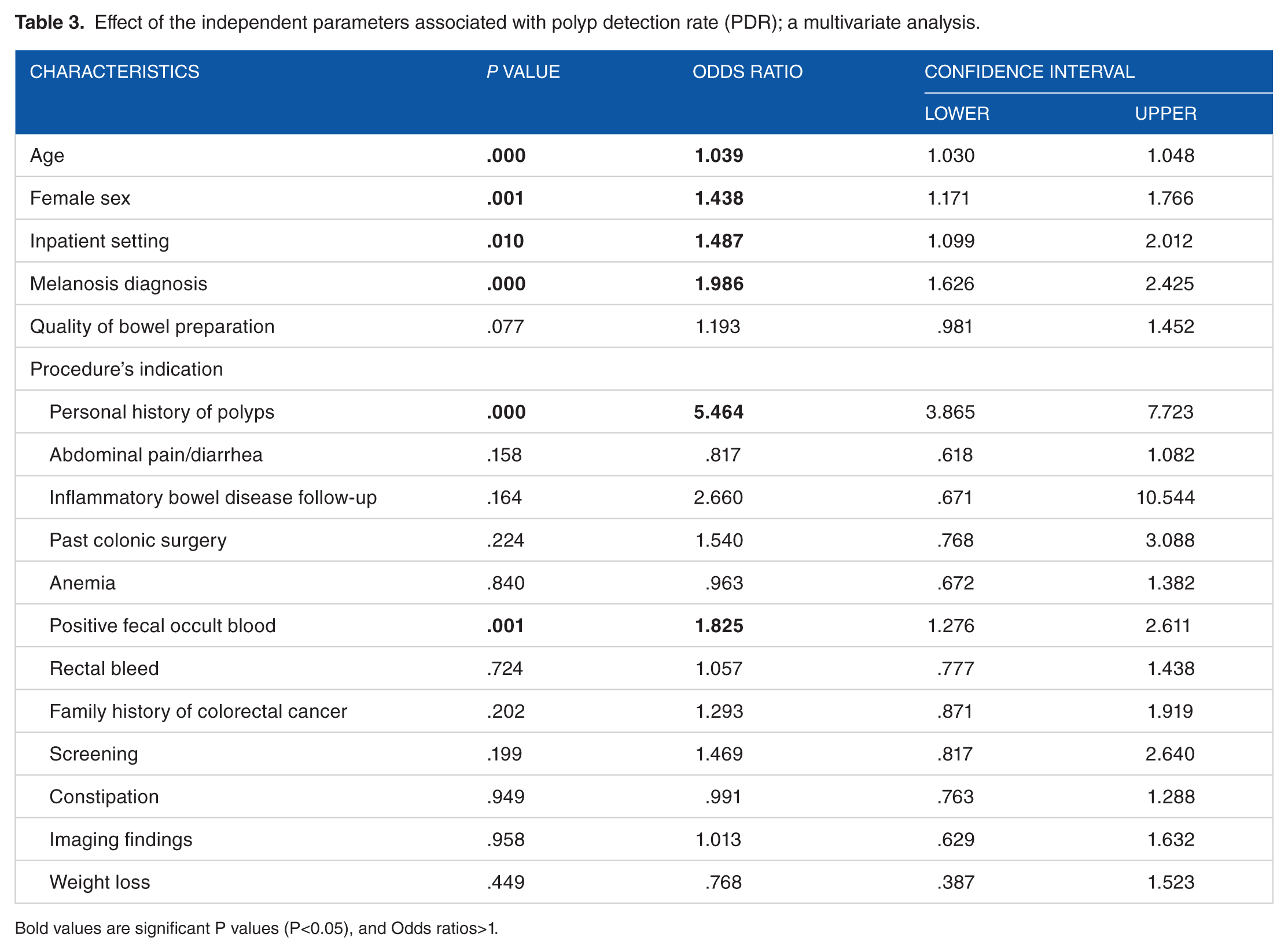
Bold values are significant P values (P<0.05), and Odds ratios>1.
In regard to bowel preparation, MC patients were less adequately prepared compared with controls (58.5% vs 65.7%; P < .001). Complete examination rate, presented by cecal intubation rate, was greater in melanosis patients (92.8% vs 85.9%; P < .001), but did not differ between groups in a subgroup analysis of patients with adequate bowel preparation only (95.7% vs 93.7%; P = .15).
Discussion
MC has long been considered as a harmless pigmentation of the colonic mucosa associated with, but not confined to, a long-term use of anthraquinone laxatives like senna or cascara. Several clinical and experimental studies, however, have provided some evidence of a possible relationship between long-term laxative use or MC and CRC risk. 22 This is particularly important as anthranoid laxatives are popular medications for constipation and one of the most widely abused, self-administered group of laxatives. Essentially, most of these studies did not include matched controls and may be widely affected by confounders.
Only few studies addressed the association between MC and polyps and reported an increased rate of polyp detection in MC patients. Nusko et al 17 demonstrated that colorectal adenomas were found significantly more frequently in patients with MC than in those without melanosis in a retrospective study of 2229 patients with MC or under chronic laxatives. Contrast effect induced by discoloration of mucosa in MC is believed to enhance polyp inspection and improve detection, as these lesions are spared in MC. Whether MC per se is associated with increased oncogenicity and actual increased risk of polyps has not been completely settled.
In our study, we included an enormous cohort of patients undergoing colonoscopy over a 15-year period and identified MC endoscopically in 718 patients (1.4%). This relatively large population of MC patients was included in the final analysis along with appropriately matched group to clarify the association between MC, PDR, and risk for CRC development. In this regard, PDR is considered as an easily utilized and practical parameter that was shown to correlate with adenoma detection rate (ADR).23,24 PDR is readily available from colonoscopy reports and does not mandate incorporation of endoscopy and pathology reports. Polyp prevalence and detection may be affected by several factors including patient demographics, bowel preparation quality, and procedure’s timing (inpatient/outpatient), and in non-screening setting, it may be influenced by procedure’s indication.25,26 Thus, we used age, gender, setting, and procedure indication for matching and included bowel preparation adequacy in subgroup analysis to neutralize their possible effect as confounders.
We demonstrated a significant increase in PDR among MC patients compared with matched controls (33.4% vs 21.8%; P value < .001). This trend of increased PDR remained unchanged in subgroup analysis of patients with adequate bowel preparation (34.1% vs 21.3%; P value < .001). In multivariate analyses, a melanosis diagnosis on endoscopy was associated with a doubled risk for polyp detection (OR = 1.986, 95% CI: 1.626-2.425; P value < .01). These findings are in concordance with findings from other recent studies. In the study by Blackett et al, 27 adenoma was detected in 34.7% of MC patients and 26.5% of controls (OR = 1.52; 95% CI: 1.04-2.24; P = .03). Our study demonstrated that MC did not confer an increased risk of malignancy and was even associated with less frequent diagnosis of CRC compared with controls (0.3% vs 3.9%; P < .001).
The increased PDR along with a reduced diagnosis of CRC is attention-grabbing and mandates further explanation. First, despite our efforts to maximize matching between groups, other confounders such as body mass index or smoking history were unavailable and may have affected PDR or CRC diagnosis. Second, we assumed that increased PDR may have contributed to reduced CRC risk, as removing pre-cancerous lesions in previous colonoscopies is associated with reduced overall and interval cancers. To better understand these findings, however, we eliminated all repeated procedures and performed a subgroup analysis on MC patients and matched controls that underwent first time colonoscopies. This subpopulation analysis yielded no change in CRC diagnosis. Taken together, these findings may indicate that most of the detected polyps were of a low dysplastic progression potential, such as diminutive and hyperplastic polyps, thus explaining a low CRC diagnosis albeit the high PDR. This may be supported by findings of a recent study by Liu et al 28 who retrospectively studied 219 patients with MC and found that although MC patients had significantly more colorectal polyps than did matched controls (1.05 ± 2.05 vs 0.54 ± 0.96, P = .001), MC was associated mainly with a higher incidence and number of colonic non-adenoma polyps and low-grade adenomas. Likewise, in the study by Blackett et al, 27 melanosis patients were more likely to have an adenoma <5 mm (OR = 1.62; 95% CI: 1.04-2.51; P = .03), but not adenomas greater than 6 mm. However, as we did not incorporate pathologic data in our study, further research on the histologic nature of these polyps is warranted.
In this study, we examined the influence of various independent parameters on PDR. In addition to the known effect of age, sex, and bowel preparation on polyp prevalence and PDR, our study showed that inpatient setting (OR = 1.487, 95% CI: 1.099-2.012), positive fecal occult blood test or personal polyp history as indication for colonoscopy (OR = 1.825, 95% CI: 1.276-2.611; P value = .01 and OR = 5.464, 95% CI: 3.865-7.723; P value < .01, respectively) were significantly associated with increased polyp detection. The impact of these parameters should be taken into account when assessing PDR, and further studies on the impact of procedure’s indication on PDR are warranted.
Our study reveals as well that MC is associated with a more inadequate bowel preparation, in the context of bowel hypomotility, and a need for repeated exams. We suggest providing an intensified regimen for bowel preparation for patients with known MC or chronic laxative use. Despite our impression of difficult colonoscopy in MC patients, cecal intubation rate did not differ between groups in patients with adequate bowel preparation.
Our study has limits inherent in its retrospective nature. Moreover, characteristics of polyps such as size, general appearance, and location, as well as histologic data were not available in our study, and thus, we were unable to determine the subtype group of detected polyps.
Other possible factors that may have impacted PDR such as variable endoscopist experience and withdrawal time could not be obtained and were not included. As there were no major changes of our department personnel during study period, as well as the usual practice mandating performance of colonoscopies under close supervision and the presence of experienced endoscopist, we assumed these factors have little impact on final results.
On conclusion, we demonstrated that MC is not associated with greater risk for CRC. Rather, there is an increase in PDR, apparently due to chromo-endoscopy-like helpful effect of MC, with detected lesions likely consisting of low progression-risk potential polyps.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Hillel Yaffe Medical Center Ethics Committee (approval no. 0124-17-HYMC). The Ethics Committee waived the need for ethics approval and the need to obtain consent for the collection, analysis, and publication of the retrospectively obtained and anonymized data for this non-interventional study
Author Contributions
FAB, AM, DF, MS, OG and YK contributed to the conception, and design of the study. FAB and AM wrote the first draft of the study. FAB, AM, DF, MS and OG performed data collection, and analysis. OG and YK performed the first critical revision of the paper and improved all contents. All authors critically revised the article and agreed with the final version to be published.