
Abstract
Aim:
To investigate the effect of video aid on quality of bowel preparation.
Study:
A retrospective study was done on patients undergoing outpatient screening colonoscopy. All subjects received educational video prior to colonoscopy in addition to the standard counseling. Patient charts were reviewed to collect data regarding quality of bowel preparation (adequate or inadequate). The study population was stratified into four groups according to viewing status: Group I 0% (control group), Group II <50%, Group III >50% to <75%, and Group IV watched ⩾75% of the video.
Results:
A total of 338 patients with an average age of 59.1 years and 60.3% females were included in the final study cohort. Of the patients in Groups I, II, III, and IV, 94.3%, 90.9%, 100%, and 91.7%, respectively, had adequate preparation (P value = .827). Adenoma detection rate (ADR) for Groups I, II, III, and IV was 28.8%, 50%, 50%, and 22.6%, respectively (P value = .305). The mean cecal intubation time was 20.7, 16.4, 16.57, and 17 minutes for Groups I, II, III, and IV, respectively (P value = .041).
Conclusions:
Video aid use for patients undergoing screening colonoscopy lacked a statistically significant impact on the quality of bowel preparation, ADR, and advanced adenoma detection rate when compared with standard practice.
Background
Colorectal cancer is one of the leading causes of cancer death in the United States. 1 Colonoscopy is the preferred modality for screening of colon cancer. Approximately 14 million colonoscopies are performed each year. 2 The diagnostic yield of colonoscopy and the ability to visualize lesions depend on adequate bowel preparation. A large fraction of patients is found to have unsatisfactory or inadequate bowel preparation at time of colonoscopy. A meta-analysis of trials on split dose polyethylene glycol bowel preparation found that 23% of the patients had poor bowel preparation. 3 Observational studies have shown varying estimates, with 17% to 33% of the patients having poor quality of bowel preparation.4–6
Bowel preparation is a complicated process, and many factors affect its quality, including both provider- and patient-related factors. Factors that predict inadequate bowel preparation include a later starting time of colonoscopy, noncompliance to bowel preparation, inpatient status, tricyclic antidepressants, male gender, history of cirrhosis, constipation, stroke or dementia, 7 low socioeconomic statuses, 8 obesity, 9 and opioid use. 10 Inadequate bowel preparation can lead to repeated colonoscopy at earlier intervals, missed pathologic lesions7,8 as well as prolonged duration of procedure, increased complications, and excessive costs. 11 Many factors affecting quality of bowel preparation cannot be altered; nevertheless, patient compliance is one factor that can be improved by enhanced patient education.
There have been multiple studies evaluating the efficacy of various educational resources to improve adequacy of colonic bowel preparation. The different resources reported in literature include illustrated brochures, videos, and education phone calls. In one study that investigated the effect of visual aids as compared with standard instructions, bowel preparation was better in the group that received instruction through visual aid prior to colonoscopy. In the experimental group (visual aid), 7% of the patients had poor preparation, compared with 18% in the control group (standard instruction; P = .02). 12 Conversely, a randomized controlled trial of 969 patients that aimed to investigate the effect of visual aid on bowel preparation found no statistically significant impact of visual aid on quality of bowel preparation; a 91% rate of adequate bowel preparation was noted in the experimental group and 89% adequate bowel preparation rate in the control group (P = .43). 13 A study done on 2530 patients undergoing screening colonoscopy found that educational video improves bowel preparation quality and reduced the need for an earlier repeat colonoscopy at 3 years. 14 A randomized case control study involving 111 African-American patients demonstrated a significant improvement in the quality of bowel preparation in the entire colon and particularly in the right side of the colon with the use of comprehensive multimedia education. 15 Another study done by Veldhuijzen et al compared computer-assisted instruction using video and three-dimensional (3D) animations with traditional nurse counseling in 385 patients and found no different in bowel preparation between the groups. 16 A randomized trial on ~500 patients showed that patients in video group demonstrated better bowel preparation than the standard instructions group. 17 The effect of patient education on bowel preparation has shown inconsistent results. Hence, there is no consensus on the best method to educate the patient.
The aim of our study is to assess quality of bowel preparation in a cohort of patients who underwent screening colonoscopy and were shown an interactive video by Emmi Solutions before colonoscopy and assess its correlation with the adequacy of bowel preparation, adenoma detection rate, and cecum intubation time.
Methodology
Study objective
The objective of this study was to investigate the effect of video aid on quality of bowel preparation, adenoma detection rate (ADR), and advanced adenoma detection rate (AADR) among patients undergoing outpatient screening colonoscopy.
Study location
We performed a retrospective study at an inner city teaching hospital. The study was approved by the Institutional Review Board.
Inclusion criteria
We included patients who underwent outpatient screening colonoscopy over a time span of 6 months. Screening colonoscopy was defined as colonoscopy performed in patients 45 years of age or older in the absence of any gastrointestinal signs or symptoms and the absence of any personal history of colon cancer or polyps or inflammatory bowel disease (IBD).
Exclusion criteria
We excluded patients with a past medical history of familial adenomatous polyposis (FAP), hereditary nonpolyposis colorectal cancer (HNPCC), IBD, and colectomy. Furthermore, patients with incomplete colonoscopy (lack of cecum intubation) and patients undergoing surveillance or diagnostic colonoscopy were also excluded.
Study method
We conducted a retrospective chart review of patients who had undergone outpatient screening colonoscopy at our center over 6 months. A list of eligible patients with their names and medical record numbers was obtained from the medical records department. A study identifier was then given to each subject. The master list of eligible patients was deleted after data were collected and checked.
We reviewed each patient’s chart to extract relevant data (age; gender; race; the presence of co-morbidities such as dementia, stroke, diabetes, cirrhosis, and thyroid disorders; and use of opioids, tricyclic antidepressants, ferrous sulfate, and antispasmodics). Colonoscopy report of each subject was reviewed to collect data related to bowel preparation, indication for colonoscopy, cecum intubation, and number and size of detected polyps. All study subjects received instructions regarding the video aid prior to colonoscopy in addition to the standard counseling. The information regarding the percentage of video watched by each subject was obtained from EMMIPrep company representative. The study population was then stratified into four groups according to viewing status: Group I 0% (control group), Group II <50%, Group III ⩾50% to <75%, and Group IV watched ⩾75% of the video.
We reviewed the pathologic findings to determine the histology. Advanced adenoma was defined as adenomatous polyp greater or equal than 1 cm in size, villous or high-grade dysplasia on histology, or the presence of three or more adenomatous polyps on colonoscopy. Adenoma detection rate was defined as percentage of patients who have one or more adenomatous polyps detected during colonoscopy. Advanced adenoma detection rate was defined as percentage of patients who have one or more advanced adenomatous polyps detected during colonoscopy. Both ADR and AADR were calculated for each group.
Video aid
All patients undergoing outpatient colonoscopy at Albert Einstein Medical Center, Philadelphia received instructions about how to view the Emmi Solutions educational video via email/telephone. The Internet-based standardized educational video, accessible via the Internet, entails details on the importance of detecting colonic polyps and appropriate steps for achieving adequate bowel cleansing. This video is a product of Emmi Solutions, which is a health care communications company. The video comprised seven sections lasting a total of 20 minutes. The video entailed the indications of procedure, preparation for the procedure (with use of different laxative regimen as per physician prescription to achieve bowel cleansing for optimum results), preprocedure steps on the day of procedure, the procedure details itself and postprocedure discharge steps. A unique code was linked to each patient’s medical record to document whether or not the Emmi program was viewed. Data, including initiation and completion of the video linking to each medical record, were provided by Emmi Solutions. Emmi Solutions was not involved in any other aspect of data collection, study design, or manuscript writing.
Emmi Solutions, LLC designs technology-based solutions to deliver patient engagement aspects for hospitals and health systems, health care payers, and ambulatory care settings. It is based in Chicago, Illinois.
Statistical analysis
Prism 7-GraphPad and SPSS were used to analyze data. Chi square was used to determine statistically significant differences between four groups for quality of bowel preparation, ADR, and AADR. One-way analysis of variance (ANOVA) was used to determine statistically significant difference among four groups for mean cecal intubation time (CIT). P value of less than .05 was used to determine statistical significance.
Results
We included 338 subjects in the final data analysis. The mean age of the study population was 59.1 years. The female to male ratio was 1:1.5. Groups I, II, III, and IV were composed of 265 (78.4%), 11 (3.25%), 2 (0.59%), and 60 (17.75%) subjects, respectively. There was no statistical significant difference in the baseline characteristics of the groups as shown in Table 1. There was no statistically significant association between quality of bowel preparation and viewing status (P value = .827) as shown in Table 2, ADR (P value = .305) and AADR (P value = .791; Figure 1). However, mean CIT and viewing status had a statistically significant correlation on one-way ANOVA testing (P value = .041; Figure 2). On further application of Tukey’s multiple comparison test to compare the four groups by viewing status, there was no statistically significant difference between the groups: Group I vs Group II (P value = .472), Group I vs Group III (P value = .923), Group I vs Group IV (P value = .053), Group II vs Group III (P value = .999), Group II vs Group IV (P value = .997), and Group III vs IV (P value = .999). The difference between Groups I and IV was noted to be marginally significant (P value = .053).
Baseline population characteristics across Groups I, II, III, and IV.
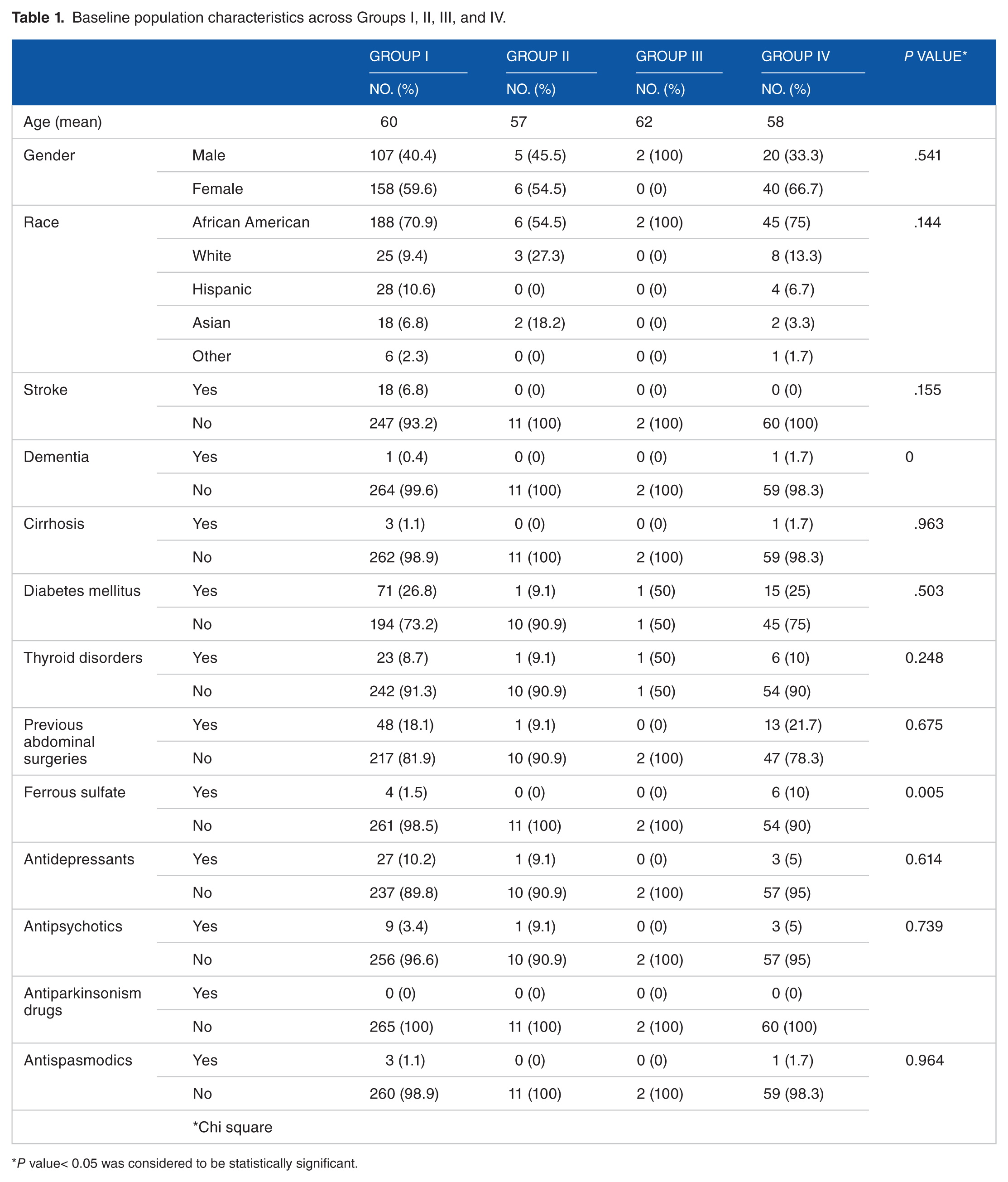
P value< 0.05 was considered to be statistically significant.
Comparison of quality of bowel preparation and use of video aid.

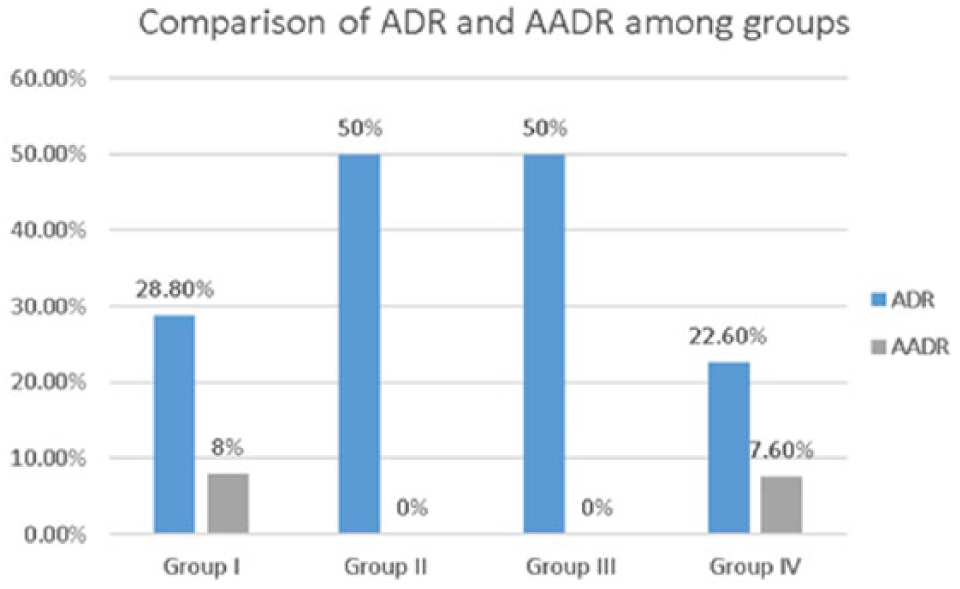
ADR and AADR across Groups I, II, III, and IV.

Mean cecum intubation time across Groups I, II, III, and IV.
Discussion
High-quality colonoscopy is dependent on optimal bowel cleansing as it has been shown to influence cecum intubation rates, procedure duration, and ADRs. There are studies with conflicting outcomes as described above. There is no consensus, if video aid really is a cost-effective strategy to improve bowel preparation outcome among patients undergoing colonoscopy. Our study adds valuable information to the current literature.
In our study, lack of any statistically significant difference among the multiple known risk factors for poor bowel preparation across four groups allows for accurate interpretation of our results. Use of iron supplements was the only risk factor with statistical significant difference across the four groups, but it was too small (3% patients on iron pills) to have any major impact on the study findings. Overall, we observed a lack of significance for effect of video aid on quality of bowel preparation (P value = .827); 94.3% (n = 250) in Group I, 90.9% (n = 10) in Group II, 100% (n = 2) in Group III, and 91.7% (n = 55) of the patients in Group IV had adequate quality of bowel preparation. Adenoma detection rate of 28.8% in Group I, 50% in Group II, 50% in Group III, and 22.6% in Group IV also failed to reach statistical significance (P value = .305). Similarly, AADR of 8% in Group I and 7.5% in Group IV was also not statistically significant (P value = .791). The mean cecum intubation time showed a decreasing trend from Group I (20.7 minutes) to Group IV (17 minutes; P value = .041). This trend could be attributed to the use of video aid, but the lack of control over the endoscopist’s experience and concomitant involvement of fellows in training add bias to this conclusion. Also, the lack of any statistically significant effect of video aid on the quality of bowel preparation further questions the cause effect association between video aid and the cecum intubation time.
There are few pitfalls to our study design. Our video aid was a composite video showing the process of preparation for colonoscopy, preprocedure steps, the procedure itself, and postprocedure steps with only a part of it focusing on the dietary restrictions and the bowel preparation agent itself. The long nature of the video and the lack of concentration on the bowel preparation could have played the role in above noted study results. In addition, lack of effect of video aid on bowel preparation quality in addition to standard practice in our population could be the result of selection bias as majority of the outpatient screening population is in good health status and shows good understanding of the instructions by the end of the office visit.
We conclude that addition of video aid to standard counseling practice by physicians regarding bowel preparation before outpatient screening colonoscopy fails to change clinical outcomes. We also believe that it will be premature to say that video aids cannot be useful in this setting in future. Video aids are an additional cost to health systems, and to justify their clinical use, we need to better define the population that will benefit from it. Development of shorter and more precise videos specific for bowel preparation agents may be useful, as well as targeting patients who demonstrate a lack of clear understanding of the instructions by the end of office visit or who have a history of poor bowel preparation.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
SF designed the study, collected data, analyzed data results, and wrote the manuscript. DJ designed the study, performed statistical analysis, reviewed, and edited the manuscript. CH reviewed and edited the manuscript. DJ, is the guarantor of the article.