
Abstract
Background:
New-onset type 2 diabetes mellitus (T2DM) is a common clinical scenario in the hospital settings. However, data on the baseline characteristics of these patients at diagnosis in Spain remain limited.
Objectives:
This study aims to describe the characteristics of 165 patients admitted to a Spanish tertiary hospital with new-onset T2DM. We analysed the use of different treatment regimens at discharge and metabolic control during follow-up.
Methods:
A retrospective, single-centre cohort study was conducted at General University Gregorio Marañón Hospital, between January 2018 and April 2021.
Results:
A total of 165 patients participated, with a mean age of 56.4 years, 62.4% of whom were men. Diabetes-related complications were observed in 24.8% of patients at diagnosis. Combined antidiabetic treatment was required in 87% of cases. The mean baseline HbA1c was 10.8%, which decreased by 4.9% after 8 months of follow-up.
Conclusion:
The clinical heterogeneity and severity of hyperglycaemia in this cohort presented management challenges, in contrast to outpatient settings. Monotherapy was rarely used, with higher adoption of SGLT-2 inhibitors and GLP-1 receptor agonists compared to other studies. Additional research is needed to refine treatment strategies and optimize care for patients with newly diagnosed T2DM.
Plain language summary
Type 2 diabetes (T2DM) can be diagnosed during hospital stays, but there is limited information about these patients in Spain. This study looked at 165 patients diagnosed with new-onset T2DM at Gregorio Marañón Hospital between 2018 and 2021. The goal was to understand their characteristics, treatment at discharge, and blood sugar control during follow-up. The average age of the patients was 56, with most being men. A quarter had diabetes-related complications at diagnosis. Most patients (87%) needed combined treatments, and two-thirds required insulin. Thanks to these treatments, most achieved good blood sugar control during follow-up. The study highlights the challenges faced by clinicians in the management of new-onset T2DM patients in a real-world clinical scenario. Many patients needed intensive treatments from the start, and more heart and kidney-protecting drugs were prescribed than previously reported. However, some patients who could benefit from these treatments did not receive them. The findings suggest that more research is needed to refine treatment approaches and improve care for people with newly diagnosed T2DM.
Introduction
Diabetes mellitus (DM) is one of the most prevalent chronic diseases, with significant public health implications. 1 Patients with DM comprise 30% to 40% of those attending Emergency Services, and approximately 25% of hospitalized patients in both medical and surgical departments. Among these patients, 50% are unaware of their diabetic condition, and in the majority of cases, the reason for hospital admission is not directly related to diabetes but to another intercurrent illness. 2
Hyperglycaemia in hospitalized patients is a significant medical problem. In hospitalized patients with type 2 diabetes (T2DM), proper glucose management can reduce length of hospital stay, postoperative complication risks, and associated costs diabetes. Clinical guidelines recommend insulin therapy during hospitalization; however, practice varies widely internationally and findings from several randomized controlled trials have shown that non-insulin drugs can have a role in the management of inpatients with T2DM.3,4
T2DM is a diagnosis of exclusion, covering a broad range of patient characteristics. This highlights the need to phenotype patients and choose the most appropriate treatment at discharge based on initial clinical suspicion. The natural evolution of the disease often aids in the final classification of DM, but this is not possible at the onset. This has significant implications for treatment choices, as uncertainty often leads to the use of insulin, given the risks associated with discharging insulin-deficient patients without this treatment.5,6
In recent years, the therapeutic arsenal for T2DM has expanded significantly. Individualization of treatment and metabolic control targets has become increasingly important. The initial HbA1c is a fundamental parameter for determining the number of drugs to use at onset, as recommended by guidelines such as the ADA Standards of Care. Understanding the potency of individual drugs is crucial for designing effective pharmacological combinations to achieve personalized HbA1c targets. 7
Although glycaemic control remains a key aspect in the management of this disease, the results of cardiovascular safety studies conducted with sodium-glucose cotransporter 2 inhibitors (SGLT-2 inhibitors) and some glucagon-like peptide-1 receptor agonists (GLP-1 agonists) have brought about a paradigm shift in treatment. The use of these molecules is prioritized due to their cardio and nephroprotective effects, independent of glycaemic control. Nevertheless, during hospital admission, the routine inpatient use of these drugs are not broadly recommended in clinical guidelines and further research is needed. 3
The strategy of intensive therapy from the start is more proactive and is based on the early use of a combination of drugs to improve glycaemic control in a faster and more efficient way. There is broad evidence that this strategy can significantly reduce DM-related complications.8,9
Large-scale observational studies have substantiated the benefits of early intervention, leading to the concept of metabolic memory or legacy effect. Available evidence suggests that early and stringent glycaemic control can improve mortality and prevent or delay long-term complications associated with this disease.8 -10
Unfortunately, a significant proportion of patients do not achieve adequate metabolic control in real-world studies.11,12 There are limited data in Spain on the characteristics of patients with T2DM at disease onset, as most studies are population-based and conducted in Primary Care settings, without exclusively focussing on newly diagnosed patients. 13 Moreover, few epidemiological studies specifically address chronic complications at the time of diagnosis. 14
Therapeutic inertia represents a significant barrier to achieving optimal metabolic control in diabetes and outcomes during the first year are critical for preventing future complications and reducing mortality. 15
This study aims to describe the clinical, epidemiological, and analytical characteristics of hospitalized patients presenting with new-onset T2DM, the antihyperglycaemic treatment strategies employed upon discharge, as well as the metabolic control achieved during 1 year of follow-up. The study is conducted in a contemporary clinical setting and aligns with emerging evidence highlighting the importance of early intensive intervention, considering the legacy effect of T2DM and the cardiovascular benefits associated with newer therapeutic agents.
Methods
Study design and population
A retrospective observational cohort study was conducted. We reviewed the medical records of patients during hospital admission between January 2018 and April 2021 in Gregorio Marañón Hospital, a Spanish tertiary hospital. Inclusion criteria included adults over 18 years of age under the care of the Endocrinology Department during hospitalization diagnosed with newly diagnosed T2DM, defined according to the 2022 American Diabetes Association criteria. 6 Exclusion criteria included patients under 18 years of age, stablished T2DM, other types of diabetes and stress-induced hyperglycaemia. Eligible patients were identified using the hospital discharge database and all consecutive patients were included in the study. The protection of participants’ personal data was ensured through the use of pseudonymized data. Follow-up extended until 12 months after hospital discharge. Retrospective data may introduce bias, limit control over variables, and weaken causal inferences.
Variables and data collection
Sociodemographic, clinical and biochemical variables reflected in clinical history during hospital admission and follow-up consultation were collected. Pseudonymized data were used.
Primary and secondary endpoints
The primary endpoint was to evaluate the epidemiological, clinical, and laboratory characteristics of patients presenting with new-onset T2DM admitted to the General University Gregorio Marañón Hospital between 2018 and 2021. The secondary endpoints were to establish the prevalence and types of diabetes-related complications presented at diagnosis, the antihyperglycaemic treatment selected at discharge and the metabolic control achieved during 1 year of follow-up assessed by HbA1c.
Statistical analysis
Quantitative variables were represented as mean and standard deviation (SD) or median and p25 to p75, as appropriate. Qualitative variables were expressed as absolute and relative frequencies.
Correlations were estimated with Spearman’s Rho coefficient. Repeated-measures hypothesis contrasts were performed with McNemar’s or Friedman’s tests, as appropriate. P-values <.05 were considered statistically significant.
The statistical analysis of the data was performed using the SPSS version 22 statistical package.
Results
Study population
A total of 209 patients with new-onset DM were identified during the study period; 165 had a definitive diagnosis of T2DM registered in their medical history and were included in the study. Table 1 summarizes the demographic data of the sample.
Characteristics of new-onset T2DM patients.

Percentages of those with diabetes-related complications.
Laboratory analysis
Some biochemical results at diagnosis are summarized in Table 2.
Analytical features of patients with new-onset T2DM during hospitalization.

About 45.6% of the patients had LDL-c < 100 mg/dl (2.58 mmol/l) and 20.2% had LDL-c < 70 mg/dl (1.81 mmol/l). A total of 89.3% of women and 69.8% of men had low HDL-c levels. Sixty-one percent of patients had elevated triglyceride levels (>150 mg/dl [1.69 mmol/l]). 19.4% were already on statin treatment.
C-peptide levels were requested in 40.0% (n = 66) of patients with 68,2% (n = 45) showing normal values, 28.8% (n = 19) showing low values, and 3,0% (n = 2) showing high values.
For suspicion of other types of diabetes, pancreatic autoimmunity (anti-GAD, anti-IA2 and anti-insulin antibodies) was tested in 48 patients, all of whom tested negative.
Discharge antidiabetic treatment
The majority of patients with T2DM (87.6%) received combination therapy at onset (Table 3). The number of antidiabetic drugs prescribed at discharge was: 1 drug in 20 patients (12.35%), 2 drugs in 58 patients (35.80%), 3 drugs in 66 patients (40.74%), 4 drugs in 17 patients (11.11%). The most frequently prescribed drug at discharge was metformin, followed by basal insulin. Oral semaglutide was not available at the time of the study.
Antidiabetic treatment selected at discharge.

No significant differences were found by sex in number of medications prescribed at discharge (P = .084) or in the initial use of SGLT2 inhibitors (P = 0257) and GLP-1 receptor agonists (P = .285). However, patients under 70 years were more likely to receive SGLT2 inhibitors (P = .003).
Patients were discharged with different treatment regimens based on the clinician’s criteria and the clinical guidelines available at the time, within the context of routine hospital practice.
There were 161 patients with an anti-hyperglycaemic treatment regimen available at discharge, identified with up to 12 different regimens. Table 4 illustrates the relationship between the initial therapeutic regimen prescribed at hospital discharge (determined at the discretion of the prescribing physician) and the mean baseline HbA1c levels.
Type of antidiabetic treatment regimen at discharge and baseline HbA1c.
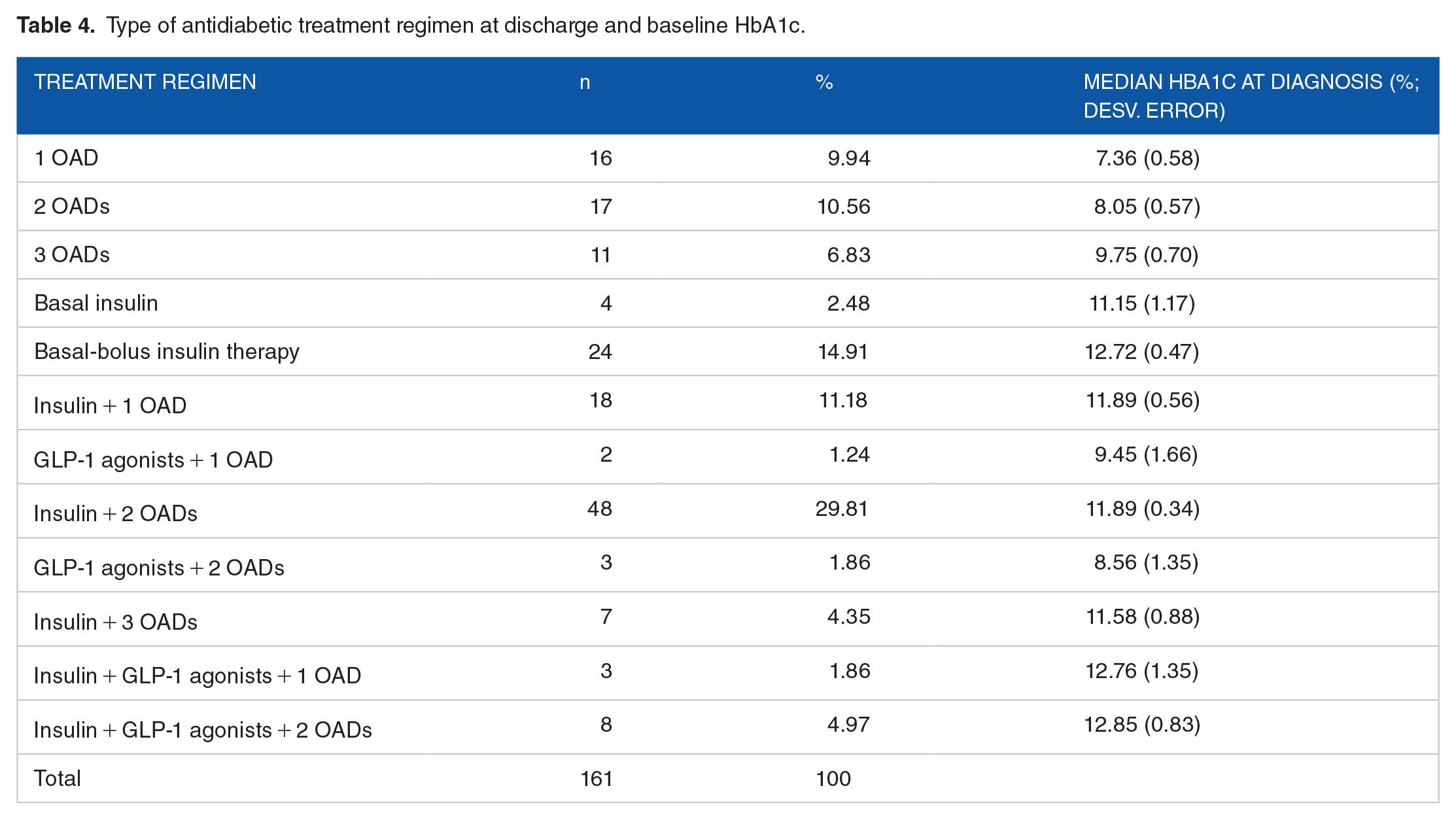
The most prescribed treatment regimen at discharge was insulin + 2 OADs, followed by basal-bolus insulin therapy.
The linear correlation coefficient between the number of prescribed drugs and the HbA1c at diagnosis is positive (r = .27), indicating that although the association is weak, a higher HbA1c corresponds to a greater number of drugs.
Follow-up data
Among those who continued with follow-up consultations, 58.1% attended the Endocrinology clinic at the same centre, 30.0% received follow-up care exclusively in Primary Care, and 11.9% attended Endocrinology clinics at another centre.
Regarding the degree of metabolic control during follow-up consultations (n = 108), patients achieved an HbA1c of 6.45 ± 1.86% within less than 1 year (mean 8.4 months). The mean HbA1c difference between baseline and less than 1 year was −4.9 (−5.6 to −4.3), P < .001 (Figure 1). No significant differences were found in mean HbA1c achieved at 1 year based on sex (P = .695) or age (<70 vs ⩾70 years; P = .906). A total of 87% of patients achieved a HbA1c < 7% and 70.5% achieved a HbA1c < 6,5% during follow-up.

Mean baseline HbA1c levels during the hospital stay (new-onset) and at follow-up consultations within 1 year (mean 8.4 months).
During the first year of follow-up, 62% of patients experienced modifications to their antidiabetic treatment. The distribution of changes was as follows: 26 patients (41.9%) had 1 change, 16 patients (25.8%) had 2 changes, 17 patients (27.4%) had 3 changes, 2 patients (3.2%) had 4 changes, and 1 patient (1.6%) had 5 changes.
The most frequent therapeutic modifications made in consultation during the first year of follow-up were: initiation of metformin in 15 patients, discontinuation of basal insulin in 17 patients and rapid-acting insulin in 11 patients. Additionally, 18 patients received SGLT2 inhibitors and 7 patients were started on GLP-1 agonists. No basal or prandial insulin was initiated in any case.
Regarding adverse effects, 4 patients reported gastrointestinal issues with metformin, leading to its discontinuation. One patient reported gastrointestinal discomfort with GLP-1 agonists, which was resolved with a dose adjustment. Three patients experienced genitourinary infections with SGLT2 inhibitors, necessitating their discontinuation. No cases of ketoacidosis were observed in patients treated with SGLT2 inhibitors.
Discussion
In this study, nearly one-third of patients (32.7%) were aged 50 or younger, reflecting recent trends indicating that the onset of T2DM is occurring at increasingly younger ages, a pattern closely linked to the obesity epidemic. 16
Simple hyperglycaemia remains predominant in T2DM; however, 14% of patients presented with acute complications such as DKA or HHS.
Admissions to Endocrinology were generally brief, as the primary reason for admission was the new-onset diabetes. The Emergency Department was the second most significant in terms of admissions. This is not coincidental, given that much of the study period coincided with the early waves of COVID-19, necessitating a swift and efficient response to facilitate prompt patient discharge. 17
Patients were admitted for various reasons, including complications related to T2DM. The development of these complications may be influenced by the fact that more than half of the cases had additional cardiovascular risk factors, and over one-third of these patients met prediabetes criteria prior to their diagnosis. Inflammation and vasoconstriction, which promote atherosclerosis, are observed in the prediabetic state. Numerous studies suggest that prediabetes can lead to both micro and macrovascular complications even before the clinical onset of DM. 18
In this study, 24% of patients had DM-related complications at the time of diagnosis. This study did not systematically screen for all potential complications but recorded those documented in the clinical history during admission.
These patients exhibited high complexity due to severe initial hyperglycaemia, with a mean HbA1c exceeding 10% (86 mmol/mol), alongside a high frequency of acute decompensations and the presence of osmotic symptoms. These characteristics differ from those of the general population with diabetes managed in Primary Care, where patients are treated in a more stable outpatient settings.19,20
At the time of hospital discharge, it is essential to provide a personalized care and treatment plan, along with appropriate follow-up, to achieve optimal metabolic control as safely and quickly as possible. 7 This underscores the need for intensive and combined treatment at discharge, which was required for 87% of the patients. Clinicians managing the patients during hospitalization made discharge treatment decisions based on their preferences and the available clinical evidence, leading to considerable variability in therapeutic choices. Consequently, patients with similar HbA1c levels received different treatments.
The utilization of these drugs with cardiovascular benefits was notably higher compared to other studies20 -22 reflecting updates in practice guidelines, 6 as most of these patients presented high or very high cardiovascular risk.
The use of GLP-1 receptor agonists is recommended as first-line drugs in patients with T2DM and established atherosclerotic cardiovascular disease, while SGLT2 inhibitors are currently the glucose-lowering drugs of choice for patients with T2DM and heart failure or diabetic kidney disease.3,7,23 The concomitant use of these pharmacological groups even appears to provide additional cardiovascular benefits compared to their use individually. 24
Nonetheless, the prescription of GLP-1 agonists at the onset of the disease remains limited, primarily due to the need for medical inspection authorization and higher costs. The initiation of SGLT2 inhibitors is sometimes delayed until confirmation of the patient’s insulin reserve and the diagnosis of T2DM over time, as there is a risk of euglycaemic ketoacidosis in the presence of insulin deficiency.
Metformin remains the most prescribed oral antidiabetic medication, used in over 70% of cases, often combined with another antidiabetic drug in a single tablet to simplify treatment and enhance adherence. 25 Notably, sulphonylureas, intermediate-acting insulins, and premixed insulins were used infrequently compared to other studies.21,26 Alpha-glucosidase inhibitors and pioglitazone were not utilized.
The high prescription of DPP-4 inhibitors seems to be linked to their excellent safety profile (particularly in elderly populations and at diagnosis, when there may be uncertainty about the type of diabetes), oral administration, and suitability for use in renal insufficiency. However, with emerging evidence supporting other drugs with cardiovascular benefits, their use appears to be increasingly less justified, particularly due to their incompatibility with GLP-1 agonists and their limited antihyperglycaemic efficacy.
Insulin use at the onset of T2DM, despite not being recommended as first-line treatment, 7 is necessary in many cases due to elevated glucose and HbA1c levels, suspicion of another type of diabetes (pending C-peptide and autoimmunity results), or osmotic symptoms. In some instances, patients are discharged before a thorough evaluation of carbohydrate metabolism is completed, and insulin treatment ensures safety in these cases. Additionally, some patients had impaired renal function, limiting the use of certain oral antidiabetic drugs.
The percentage of patients on monotherapy with a single OAD at hospital discharge was less than 10%. This percentage is significantly lower compared to the higher rates of monotherapy reported in other observational studies.19,27
To counteract therapeutic inertia, therapeutic changes were made in 62% of T2DM patients during the first year. The aim was to add medications if metabolic targets were not achieved, and for those who did achieve good control, medications with cardiorenal benefits were added if not already being prescribed.
The rate of adverse effects from antidiabetic medications was low, primarily gastrointestinal issues with metformin and GLP-1 agonists, and candidiasis with SGLT2 inhibitors, consistent with prior reports. 7 No serious adverse effects were observed, and treatment adjustments were made during the first year of follow-up.
Strengths and limitations
This study provides new real-world evidence on the characteristics of newly diagnosed T2DM patients at the hospital setting. The implementation of updated diabetes guidelines in clinical practice has led to improved metabolic control outcomes, with greater use of novel therapies with cardiovascular benefits and a reduced reliance on monotherapy compared to previously reported data.
This is a retrospective, single-centre study, which may have certain limitations. Data collection relied on previous records, which could be incomplete or biased. The lack of a formal sample size calculation or power analysis and the modest sample size could impact the generalizability and robustness of the findings. Additionally, the results may not be generalizable to other populations or centres due to the influence of site-specific factors, such as resources and demographic characteristics and the exclusion of other T2DM patients not evaluated by the Endocrinology service, who may have had more easily managed diabetes. Finally, due to the observational nature of the study design, accounting for confounding factors or establishing causality is challenging. Future longitudinal studies comparing different antidiabetic regimens should incorporate a formal power analysis to ensure an adequate sample size.
Conclusions
The new-onset of T2DM presents a significant clinical challenge during hospital admission, primarily due to uncertainty regarding the correct diagnosis of diabetes type and the appropriate response to the selected treatment at discharge. However, the disease’s onset during hospitalization offers a chance to optimize treatment and prevent complications and readmissions.
This observational real-world study, conducted in a modern clinical environment, highlights the early adoption of intensive and combined therapies from the outset, which were required in 87% of cases. The complexity of the treatment is reflected in the high number of different therapeutic regimens (up to 12), with two-thirds of patients requiring insulin therapy at discharge.
Although the prescription of SGLT-2 inhibitors and GLP-1 agonists is progressively expanding to include more patients, it does not yet reach all those who could theoretically benefit from their use. Therefore, comparative studies with different combination regimens, as well as cost-effectiveness analyses considering potential cardiorenal benefits, are needed.