
Abstract
Background:
Hammertoes is one if not the most common deformity that afflicts the diabetic foot and leads to increased risk of diabetic foot ulcers. Flexor tendon tenotomy treatment of the diabetic hammertoe has gained increased interest and is now recommended in international guidelines as a treatment of hammertoes to prevent diabetic foot ulcers. There is however no published data on the long term outcomes following tenotomy treatment.
Introduction:
The objectives of this study was to describe the demographics and long-term outcomes following tenotomy treatment of individuals with diabetes who had flexor tendon tenotomies of hammertoes performed between 2006 and 2009.
Methods:
This was an observational study of a cohort from a prior study. The study was performed at Steno Diabetes Center Copenhagen between 1st of January 2020 and 31st of June 2020. Participants from the prior study were invited to join the study, consisting of one visit where foot examination was performed by orthopedic surgeon. Information on medical history was obtained from medical records.
Results:
Of the original 38 operated participants, 21 (55.3%) had died during the follow-up period, one (2.6%) had moved away, and one (2.6%) had incorrect procedure performed originally. At follow-up (mean 149.7 months (±17)), age of the remaining 15 participants (86.7% male) was 66.6 years (±11.4), diabetes duration was 32.2 years (±13.3), all had neuropathy and 14 (93.3%) had palpable foot pulses. The 15 Included participants had 22 toes tenotomized in the original study, of which five toes (22.7%) in four participants (26.7%) had recurrent hammertoe deformities. Of the 15 participants, 14 (93.3%) had incurred at least one ulcer during the observation period, and eight (53.3%) had incurred an amputation.
Conclusion:
This study reports an undescribed risk of recurrence of deformities after tenotomies and supports that this population is at high risk of new ulcers, amputations, and have a high mortality rate.
Plain language summary
One of the complications that afflict individuals with diabetes is the diabetic foot complication. The term diabetic foot covers several ailments that may afflict the foot like ulcers, infections and in the worst-case amputations. The diabetic foot has a close connection to several other complications of diabetes like reduced sensation and blood supply. Reduced sensation effectively shuts of the alarm that informs of increased pressure on the feet and reduced blood pressure cuts of the supply lines that would help repair the damaged tissue. In addition, there is a close connection between foot deformities and risk of diabetic foot ulcers. This is compounded by deformities being more common in individuals with diabetes. The most common deformity is a hammer toe, where the toe is drawn into a flexed position resembling the form of a hammer. This leads to increased pressure at the tip of the toe that is now driven into the ground and on the dorsal side of the toe, that now is elevated and rubs against the roof of the footwear. We recently published a study showing that a simple procedure, with low risk of complications, where the flexors of the toes are severed can correct this deformity and the procedure is now recommended by international guidelines. Unfortunately, we do not know what happens in the years after the procedure has been performed, and that is what is reported in this study. We found that there is a risk of reforming of the flexor tendons over time following the surgery. This can easily be addressed by performing the procedure again. More concerning is a high risk of new ulcers and amputations for the individual who had the procedure performed. This is not linked to the procedure in itself, but rather shows that this group of people are vulnerable and should be followed closely by a team of health care professionals, that can address the risk factors that may lead to complications.
Introduction
Hammer, mallet and claw toe deformities (from here on referred to as hammertoe deformities) have been shown to be risk factors for development of diabetic foot ulcers (DFUs)1,2 and to be some of the most common foot deformities incurred by individuals with diabetes.3,4 The development of the diabetic hammertoe deformity has been and still is a discussed topic, with more than one school of thought. 5 A Dutch study showed that even the classification and description of the hammertoe deformity is challenging with little agreement across clinicians. 6 Finally, it is still debated what surgical approach should be taken to treat diabetic hammertoe deformities on the basis of both underlying pathology and clinical presentation. 7 Regardless of what pathophysiology or clinical presentation lies at the root of these deformities, it has been shown that they increase pressure at the plantar aspect of the foot, which is one of the main predictors of DFU development.8,9
At the same time it has become evident that the risk of amputations and mortality for people with diabetes is closely linked to the incidence of DFUs. 10 The challenge of the DFU is evident when considering that up to one in three of all people with diabetes incur a DFU in their lifetime. 11 In addition, there is a large risk of infections complicating the course of a DFU, 12 that close to 8 in 10 of all amputations in the population with diabetes is preceded by a DFU 13 and the mortality of people incurring a DFU is comparable to most common cancers, with a steep rise if the DFU results in an amputation. 10 At the same time the cost of treating DFUs is rising and it is now one of the most expensive complications to diabetes. 14 These facts highlight the need for not only solid treatment options for people with DFUs, but also the need for improved strategies to prevent new and recurrent DFUs. 15
The first-line treatment of increased pressure on toes associated with hammertoe deformities of the diabetic population is offloading in the form of footwear with rocker bottom, individually adjusted inlays and offloading devices, that is, splints and pads. Several factors influence the success rate of offloading devices including patient adherence, degree of deformity and patient factors, that is, neuropathy and atherosclerosis. If offloading devices fail, surgical correction is the next step. Surgical correction of hammertoe deformities is one of the most common foot and ankle procedures performed worldwide, both for people with and without diabetes. 16 Supported by several studies,1,17 -25 flexor tendon tenotomy treatment of individuals with diabetes and hammertoe deformities has become one of the preferred surgical procedures used when treating individuals with diabetes and hammertoe deformities at many institutes. We recently published the first randomized clinical trial supporting the use of flexor tendon tenotomies by needle in preventing and treating DFUs on hammertoes. 26 This has led to a recommendation for performing tenotomies for individuals with diabetes and hammertoes in the most recent guidelines from the International Working Group of the Diabetic Foot 27 Despite the increased use of flexor tendon tenotomy treatment and the multiple studies investigating the effects of the procedure, no studies have investigated the long-term effects following flexor tendon tenotomy.
Over the past years, we have experienced recurrence of hammertoe deformities 5 to 15 years after primary surgery in the form of flexor tendon tenotomies. Until now, recurrence of deformities after flexor tendon tenotomies has not been described. However, healing of tendons after tenotomy of other muscles have been described in animal 28 and human studies.29,30
This study was driven by a clinical observation of a, hereto, undescribed observation that flexor tendons may regenerate over time, leading to a possible recurrence of hammertoe deformities for the individuals treated by tenotomy previously. This may in turn lead to new ulcers which could lead to infections and amputations over time. This led us to invite a cohort treated with tenotomies from a previous study conducted at our institute to participate in a follow-up study. The aim of the study was to evaluate the risk of recurrence of hammertoe deformities after flexor tendon tenotomy and to describe the long term outcomes following flexor tendon tenotomies in a cohort of individuals with diabetes and hammertoes who had tenotomies performed between 2006 and 2009. 1
Materials and Methods
This study was performed as an observational cohort study conducted in accordance with the Helsinki declaration on ‘Ethical Principles for Medical Research Involving Human Subjects’ 31 after approval by the Danish Patient Safety Authorities (P-2019-840, 19th of December 2019) and Danish Data Protection Agency.
All participants from the study ‘Percutaneous flexor tenotomy for preventing and treating toe ulcers in people with diabetes mellitus’ 1 were identified from the identification log from the original study. All participants from the original study were included in the study. There were no other inclusion criteria than inclusion in the original study applied. No specific exclusion criteria were applied, despite this, one participant was excluded due to incorrect procedure performed in the original study.
In the following a brief introduction to the methods of the original study is outlined. For the full details please refer to the original article. 1 The original study was designed as a retrospective cohort study of individuals treated with tenotomies in a four-year period (January 2006 to December 2009). Included participants had diabetes (of any type), hammertoes, mobile metatarsophalangeal joint(s) and ulcers or impending ulcers on the tip of the toe. Participants were treated with a flexor tendon tenotomy of both flexor digitorum longus and brevis. The procedure was performed by scalpel through a plantar approach in local anesthetics. Participants were hospitalized for 2 to 3 days following procedure.
The current study was performed between 1st of January 2020 and 31st of June 2020 at Steno Diabetes Center Copenhagen. Participants from the original study who were not lost to follow-up were invited for a one-hour foot examination by an orthopedic surgeon. After written informed consent was acquired, the examination was performed, and patient electronic health records were accessed, and relevant data was extracted for longitudinal analysis.
The examination was performed by the same orthopedic surgeon. The examiner accessed the electronic health records of participants prior to examination to identify treated toes and described effects on hammertoe deformities and ulcer healing. Thereby the examiner was not blinded to participants original procedure or outcomes. Findings like hammertoe recurrence, skin changes, that is, ulcers, calluses, nail changes and other signs of pressure, deformities of the feet and ankles and status of pulses in the feet were noted. Recurrence of hammertoe deformity and recurrence of ability to flex treated toes was assessed by comparing notes on deformity and changes in deformity following tenotomy from electronic health records regarding procedure and outcomes during the follow-up in the original study, to findings during examination in this study. Feet and ankles of participants were assessed sitting and standing. If the participant was not able to stand, the feet of the participant were only assessed sitting. Active flexion was defined as participants ability to activate flexor digitorum longus and/or brevis with resulting flexion in one or more of the metatarsophalangeal, proximal/distal interphalangeal or in case of the hallux interphalangeal joint.
From the patient electronic health records, data pertinent to baseline characteristics and longitudinal outcomes were extracted from electronic health records.
A DFU was defined as a lesion of the skin on the foot of a person who has diabetes. 32
Impending ulcer was defined as callosities or nail changes in spots equal to the anatomical placement of ulcers associated with deformities. 25
Peripheral neuropathy was defined as vibration sensation over 25 V, measured by biothesiometri.
After approval by Danish Patient Safety Authority and Danish Data Protection Agency, data used for comparison of participants who died with participants who were still alive were extracted from patient electronic health records using date of original operation or date closest to the date of original operation as reference (Figure 1).

Consort diagram.
Data extracted included the following were available and relevant; date of original operation, date of death, gender, age, diabetes duration, diabetes type, history of smoking, alcohol intake, body weight, height, systolic and diastolic blood pressure, HbA1c, eGFR, plasma Lipoproteins, plasma triglycerides, biothesiometri, monofilament examination, toe blood pressure and prior history of ulcers, amputations and Charcot’s neuropathy.
Data was subsequently registered in an electronic data capture system REDCap® (Vanderbilt University, Nashville, TN, USA) and statistical analysis was performed using SAS® Studio 3.7 (SAS Institute, Cary, NC, USA). Demographics were calculated using simple summary statistics. Non-paired t-test was used for continuous variables and chi-squared for categorical variables when comparing data between participants who died and those who did not, and participants who had recurrence of hammertoes with those who did not. Correlation between death and relevant clinical parameters as well as correlations between recurrence and relevant clinical parameters were examined using logistic regression.
All continuous variables are presented as mean ± standard deviation. Non-normally distributed continuous variables are presented as median followed by (25% and 75% percentile) and log transformed before further calculations. Categorical and ordinal variables are presented as percentages of total.
Statistical significance was defined as P < .05.
Results
Of the original 38 participants, 15 accepted the invitation to participate in the study. A total of 21 (55.3%) participants had died since the original operation, one (2.6%) had moved and one (2.6%) was excluded due to having extensor tendon tenotomy rather than flexor tendon tenotomy performed originally.
There was a mean follow-up of 149.7 months (±17.0) for the 15 included participants who had a mean age of 66.6 years (±11.4) with 13 male participants (86.7%). Of the 15 included, nine had type two diabetes (60.0%) and the remaining six had type one diabetes (40.0%) with a mean diabetes duration of 32.2 years (±13.3). All participants had neuropathy. As noted in Table 1, only 13 participants had biothesiometri and monofilament examination performed, which was due to two participants incurring above ankle amputations bilaterally since the original operation. Similarly, data on specialized footwear is only given for the 13 participants who had not experienced an above ankle amputation and all 13 participants wore specialized footwear (Table 1).
Baseline characteristics at date of follow-up examination.
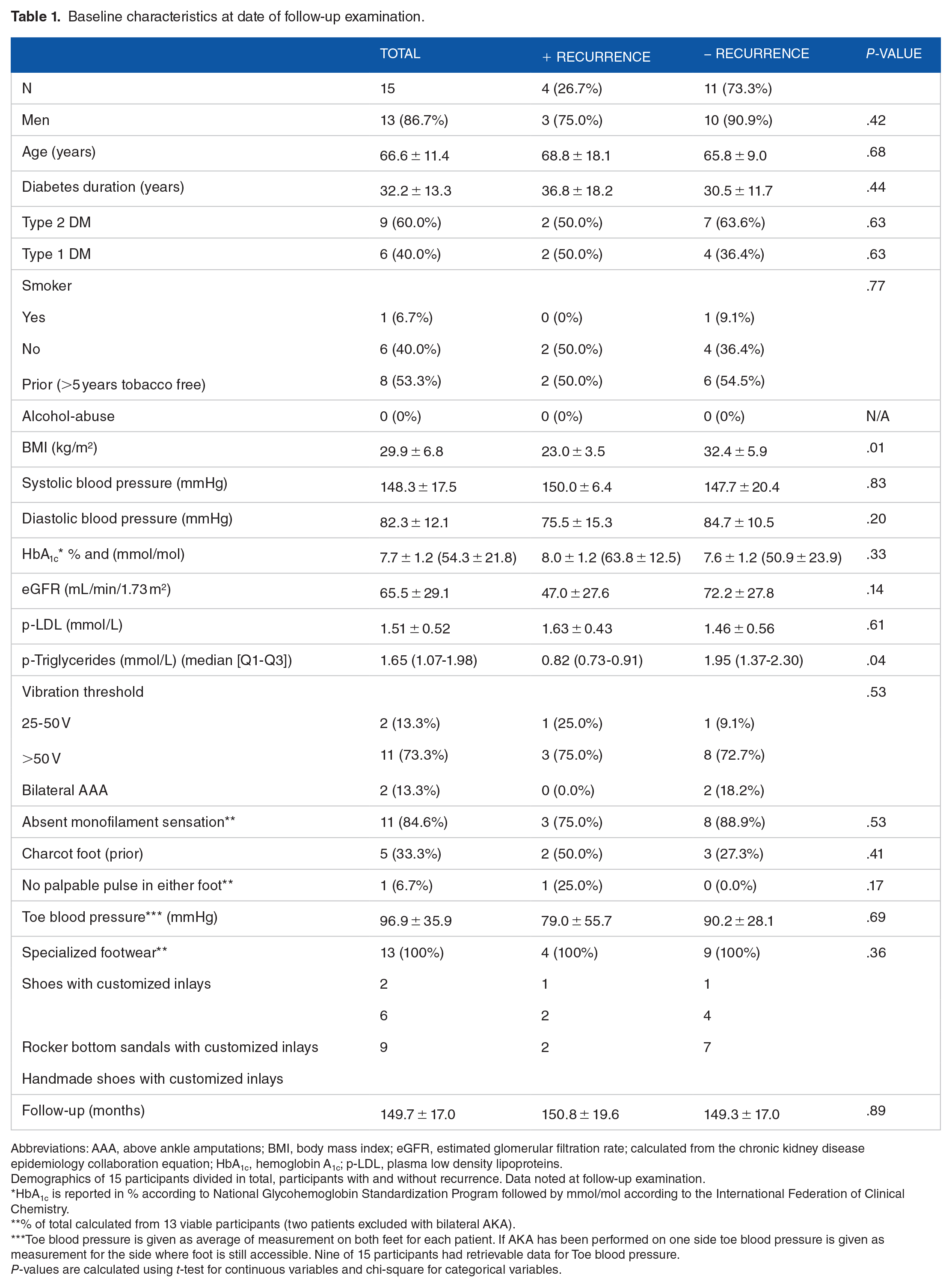
Abbreviations: AAA, above ankle amputations; BMI, body mass index; eGFR, estimated glomerular filtration rate; calculated from the chronic kidney disease epidemiology collaboration equation; HbA1c, hemoglobin A1c; p-LDL, plasma low density lipoproteins.
Demographics of 15 participants divided in total, participants with and without recurrence. Data noted at follow-up examination.
HbA1c is reported in % according to National Glycohemoglobin Standardization Program followed by mmol/mol according to the International Federation of Clinical Chemistry.
% of total calculated from 13 viable participants (two patients excluded with bilateral AKA).
Toe blood pressure is given as average of measurement on both feet for each patient. If AKA has been performed on one side toe blood pressure is given as measurement for the side where foot is still accessible. Nine of 15 participants had retrievable data for Toe blood pressure.
P-values are calculated using t-test for continuous variables and chi-square for categorical variables.
A total of 22 toes were originally operated, of these five toes (22.7%) had recurrent hammertoe deformities. The five recurrent hammertoe deformities were divided on four participants (26.7%).
Triglycerides and BMI were significantly lower (P < .05) for the participants who experienced recurrence of hammertoes compared to those who did not experience recurrence. No other baseline characteristics showed significant difference between the two groups (Table 1).
Using logistic regression, no significant association was found between risk of hammertoe recurrence and clinical characteristics (gender, age at follow-up visit, diabetes type, tobacco use, BMI, blood pressure, HbA1c, p-LDL, p-triglycerides, vibration sensation, monofilament sensation, prior history of Charcot arthropathy, palpable foot pulses, toe blood pressure or use of offloading devices).
All the toes with recurrent hammertoe deformities had either impending ulcers or active ulcers on the operated toes. Active flexion was seen in three of the five toes with recurrent hammertoe deformities.
Of the 15 participants, 14 incurred at least one DFU on the same foot as the operated toe(s) or the ipsilateral foot in the follow-up period and these 14 participants incurred a mean of 15.0 DFUs (6.3-18.8, Q1-Q3) per participant. During the follow-up period eight participants incurred a least one amputation; Six below ankle and seven above ankle amputations (Table 2).
Foot related outcomes.

Divided in operated toes and participants operated, and variables are given related to relevant category. Categorical data is given as percentage of total, continuous data is given as mean with Q1 to Q3.
Foot ulcer refers to ulcer below ankle on either side, with or without connection to the hammertoe deformity.
At time of the original operation the 21 individuals, that died during follow-up, had a mean age of 68.9 years (±9.9) which was significantly (P < .05) higher compared to the age at time of original operation for the 15 participants who were still alive (54.6 years (±11.2)). No other differences in clinical parameters were observed (at time of original operation or date closest to date of original operation) between individuals who died and those who were still alive (Table 3).
Baseline characteristics at date of original examination.
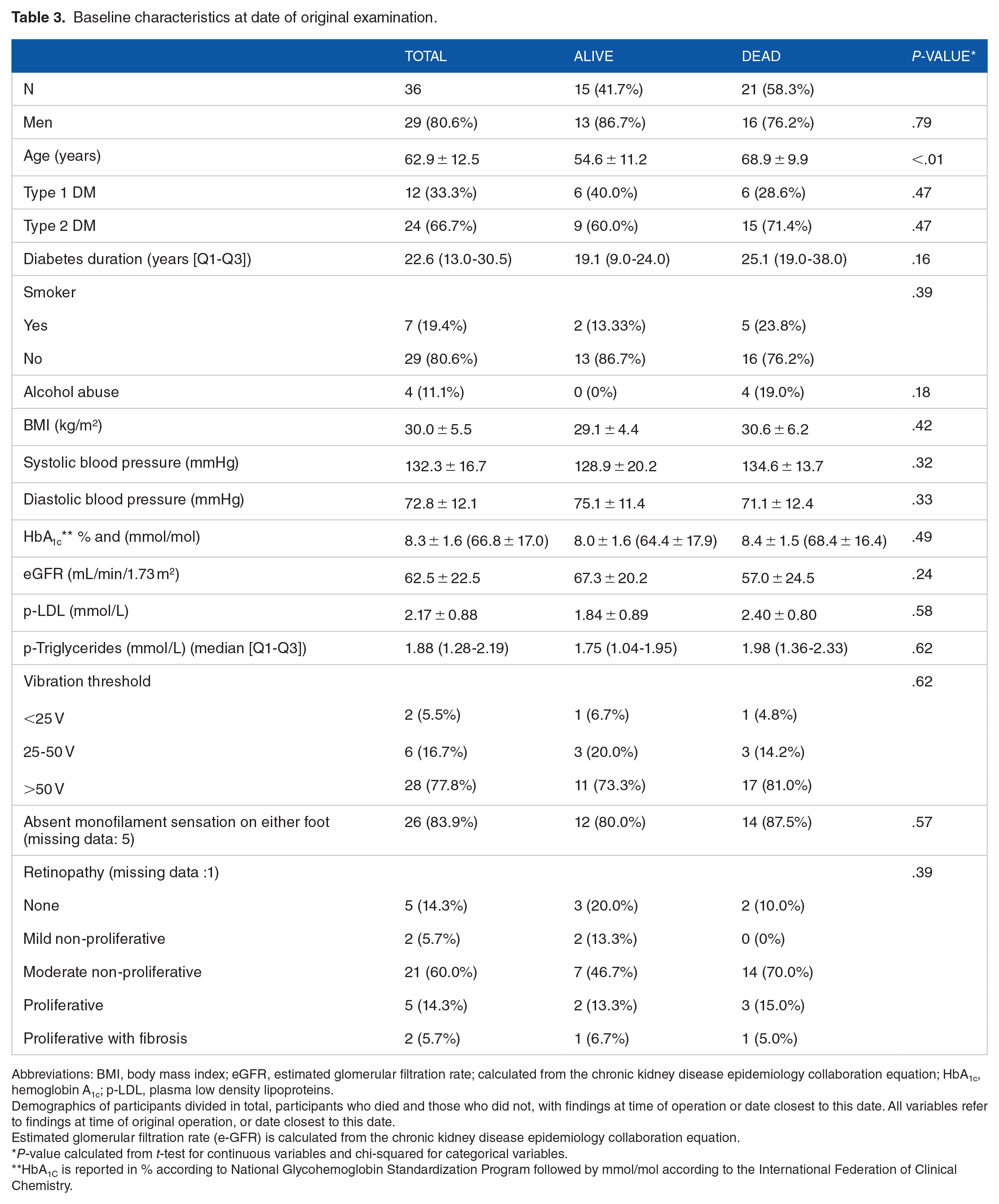
Abbreviations: BMI, body mass index; eGFR, estimated glomerular filtration rate; calculated from the chronic kidney disease epidemiology collaboration equation; HbA1c, hemoglobin A1c; p-LDL, plasma low density lipoproteins.
Demographics of participants divided in total, participants who died and those who did not, with findings at time of operation or date closest to this date. All variables refer to findings at time of original operation, or date closest to this date.
Estimated glomerular filtration rate (e-GFR) is calculated from the chronic kidney disease epidemiology collaboration equation.
P-value calculated from t-test for continuous variables and chi-squared for categorical variables.
HbA1C is reported in % according to National Glycohemoglobin Standardization Program followed by mmol/mol according to the International Federation of Clinical Chemistry.
Using logistic regression, age at date of original operation was associated with risk of death during follow up (P < .05) with an odds risk ratio of 1.17 (95% CI 1.04-1.31). No other association between risk of death and other clinical parameters at time of original operation (ie, gender, diabetes type, diabetes duration, vibration sensation, monofilament sensation, retinopathy grade, tobacco use, alcohol abuse, BMI, HbA1c, eGFR, hemoglobin, p-LDL, p-HDL, systolic and diastolic blood pressure) was found using logistic regression.
Discussion
As diabetes has become more prevalent around the world and the lifetime expectancy has risen for persons with diabetes so has the prevalence of late stage complications associated with diabetes including diabetic foot ulcers. 33
Even though there are signs of a decline in the yearly incidence of DFUs, 34 the lifetime risk of developing a DFU for people with diabetes is still estimated as 19%-34%. 35 With this in mind, it is essential to find effective measures of treating and preventing DFUs.
One of the surgical tools for treating and preventing DFUs with the highest level of support in the published literature is flexor tendon tenotomy of the diabetic hammertoe deformity. 27 Despite tenotomy treatment gaining traction as a treatment option for individuals with diabetes and hammertoes, no one has, to our knowledge looked at the long-term effects or demographics for individuals who have tenotomies performed. In this study, we observed that approximately one in four toes had recurrent hammertoes deformities after flexor tendon tenotomy and more than half of the recurrent hammertoes had regained active flexion. It should be mentioned that following conclusion of the study, individuals with toes that had regained active flexion were offered and accepted re-tenotomi, with subsequent straightening of the toe and abolished flexion of the toe. The reason underlying recurrence of hammertoe deformity and regained flexion could be multiple. It could be speculated that the flexor tendons where not severed completely at the primary intervention. However, looking through the patient electronic health records in all cases a straightening of the tenotomized toe with abolished flexion was described. In addition, the procedures performed in the original study by Rasmussen et al was done using a scalpel which will allow you visual confirmation of the severed tendons making it unlikely that a less than completely severed tendon would be missed. 1 A more likely explanation is healing of the tendons over time.
The healing of tenotomized tendons has been described and hypothesized since 1800s 36 and it has been shown in larger tendons in human studies.29,30 It therefore might seem obvious that the flexor tendons of the toes could heal over time. However, this is counterintuitive when considering traumatically severed tendons of the fingers or toes where there is a strong indication of surgery to prevent loss of function from the severed tendon.37,38 On the other hand whether or not to surgically treat the traumatic Achilles tendon rupture is still hotly debated. 39 Regardless of the underlying path to healing of tendons after rupture, whether traumatic or iatrogenic, the simple fact that hammertoe deformities are a risk factor for DFUs and thus amputations, makes it essential to be aware that flexor tendons can reform over time following tenotomy. As a curiosity we found a significantly higher BMI and a significantly lower plasma triglyceride level in the group that incurred recurrence of hammertoe deformities. We can not propose a causal connection between higher BMI and lower plasma triglycerides and thus suggest that this is a random finding.
More than half of all included individuals with diabetes and hammertoes who were treated with tenotomies had passed away during the follow-up period. Not surprising age at time of original operation was associated with risk of death during follow-up. However, none of the other examined clinical parameters were found to be associated with mortality. The pressing question is if the high mortality in the population was related to the tenotomy procedure, which there was no signs of. It is well known that individuals with diabetes who incur ulcers and amputations have a high 5 year mortality 10 and the results from this study showed that there was a high prevalence of new DFUs and amputations in the population that were treated with tenotomies. More than 90% of the individuals that attended follow-up visit had incurred one or more DFUs and more than half had incurred an amputation below or above ankle during the follow-up period. This leads us to conclude that tenotomies have no direct effect on mortality for treated individuals, but rather that the population where tenotomy is indicated have several competing challenges, that is, complications of diabetes, diabetic foot ulcers and amputations, that affect their mortality rates. With a median age of 62.8 years at time of inclusion in the original study, performed more than 10 years ago, natural aging is, at least part of the explanation for the high mortality seen in the study. Finally, we did not include a control group in this study and the study was neither designed nor powered to observe mortality in the cohort.
There are limitations to this study, the largest being the limited number of participants which impacts the ability to detect relevant factors related to outcome, and the lack of a control group in the study which limits the studies translation to a generalizable conclusion for individuals with diabetes. The nature of retrospective study limits the conclusions we can draw from this study. Despite finding a hereto undescribed risk of recurrence of hammertoe deformities following tenotomy treatment, we can not explain the underlying pathophysiology. We did not have the opportunity to perform imaging of the flexor tendons to support the claim of healing of the previously tenotomized tendons. A future study including ultrasound assessment of tenotomized tendons is being planned at our institute to address this gap in knowledge.
Conclusion
In conclusion, we report a new complication to flexor tendon tenotomy treatment of hammertoe deformities namely healing of the tendons over time with a risk of recurrence of hammertoe deformities. The risk of recurrence of hammertoe deformity after a flexor tendon tenotomy needs further research to uncover pathophysiology and risk. In addition, the high mortality and morbidity found for the population in need of tenotomies supports the need for close follow-up in a multidisciplinary team to optimize the treatment and prevention of risk factors including recurrence of hammertoe deformities following tenotomies.