
Abstract
Background:
Metformin plays a major part in the treatment of polycystic ovarian syndrome .Trials are being conducted to compare the effectiveness of combination of metformin with cabergoline in the treatment of hyperprolactinemia and polycystic ovarian syndrome.
Objectives:
The purpose of this study is to compare the effectiveness of metformin monotherapy and combination therapy with cabergoline versus metformin for the management of polycystic ovarian syndrome with hyperprolactinemia.
Methodology:
An extensive search up until 31 May 2024 of electronic databases (PubMed, Registry of Controlled Clinical Trials, Web of Sciences, SCOPUS) to find pertinent studies. An analysis was conducted with both observational data and randomized clinical trials . To compute the standard mean difference, weighted mean difference, odds ratio, and 95% confidence interval, RevMan (v5.3) was utilized. Primary outcomes that were assessed included body-mass index, regular menstruation, weight change, prolactin, testosterone, and dehydroepiandrosterone-sulfate levels.
Results:
Three randomized controlled trials and 1 observational study, taking a total patient population of n = 535, were part of our final analysis. Prolactin (SMD = −3.23 95% CI: (−4.90, −1.55)) and dehydroepiandrosterone-sulfate levels (SMD = −0.27 95% CI: (−0.52, −0.01)) were significantly lower in the metformin and cabergoline combination therapy group; monthly regularity was also significantly higher (OR = 3.07 95% CI: (2.09, 4.51)). Statistically, there was no significant difference in weight, body-mass index, or testosterone levels.
Conclusions:
In the treatment of polycystic ovarian syndrome, the combination of metformin and cabergoline significantly lowers prolactin levels and encourages regular menstrual cycles. Although metformin has the potential to suppress testosterone levels, more investigation is required to determine how combination therapy affect dehydroepiandrosterone-sulfate and testosterone levels. It’s interesting to note that while neither intervention had a substantial impact on weight or body-mass index, metformin and cabergoline combination therapy outperformed metformin monotherapy in terms of supporting regular menstrual cycles. Customized therapy approaches are essential, and large-scale trials involving a variety of groups are required to comprehend the safety and effectiveness of treatments.
Plain language summary:
In this study, 2 therapies for women with high prolactin levels—a hormone associated with PCOS—were examined. Their goal was to determine which combination of metformin and cabergoline produced the best results.Observational data and randomized clinical trials were included while searching through several databases for pertinent studies. Researchers discovered that the combination of metformin and cabergoline was superior to using metformin alone in reducing prolactin and another hormone called DHEAS. The menstrual periods of women receiving the combined therapy were also more regular. However, there wasn’t much difference in weight, body mass index (BMI), or testosterone levels between the 2 groups. In summary, it appears that the combination of cabergoline and metformin is a more effective way to treat the symptoms of PCOS, which include irregular periods and elevated prolactin levels. To find out how it impacts other hormones and whether it’s long-term safe and effective, further research is still required.
Highlights
(1) Polycystic ovarian syndrome (PCOS), a prevalent endocrine disorder, affects 6% to 20% of fertile women. The diverse range of clinical symptoms associated with PCOS, such as hyperandrogenism, irregular menstruation, and infertility, makes treatment management difficult.
(2) No previous meta-analyses and systematic reviews comparing the efficacy of metformin and cabergoline combination therapy and metformin monotherapy for the management of PCOS with concomitant hyperprolactinemia.
(3) The findings of this study can help in counseling patients of PCOS with concomitant hyperprolactinemia. It may facilitate clinicians in designing future studies and improve clinical guidelines for the management of patients.
(4) In PCOS patients with hyperprolactinemia, our meta-analysis highlights the advantages of combination therapy with metformin and cabergoline for improving DHEAS, menstrual regularity, and prolactin levels. We found no appreciable difference in testosterone levels, body weight, or BMI between metformin alone and in combination with cabergoline.
Introduction
Among women who are fertile, 6% to 20% are affected by polycystic ovarian syndrome (PCOS), a common endocrine condition. 1 PCOS poses a challenging therapeutic management due to its varied clinical symptoms, which include hyperandrogenism, irregular menstruation, and infertility.2-4 About 30% of PCOS patients present with high prolactin levels, which complicates the clinical picture among its diverse presentations. 5 Anovulation and irregular uterine bleeding can result from hyperprolactinemia, which is defined by elevated serum prolactin levels that upset the delicate balance of the hypothalamic-pituitary-ovarian axis. 6
Because it makes insulin more sensitive, metformin, a mainstay in the treatment of Type 2 diabetes mellitus, has become a leading treatment for PCOS. 7 Metformin is a commonly given medication that treats diseases connected to steroids, improves menstrual regularity, and increases fertility in PCOS women. 8 On the other hand, the dopamine receptor agonist cabergoline has the potential to treat hyperprolactinemia. 9 Additionally, studies have shown that it is effective in helping PCOS patients with their irregular menstrual cycles and restoring normal androgen levels.10,11
Many approaches to treating PCOS have been investigated, such as probiotic medication and glycemic index reduction. Pro- and synbiotic supplements dramatically lowered blood sugar levels during fasting. According to the research, pro- and synbiotic supplementation may help PCOS-affected women’s glucose homeostasis metrics, hormone levels, and inflammatory indices. 12 There is evidence that women with PCOS who follow an Low glycemic index diet have improved cardiometabolic and reproductive profiles; however, further research is needed to fully understand the advantages of an Low glycemic index diet in general. It is challenging to separate the effect of the Low glycemic index diet on PCOS outcomes due to sources of uncertainty such as small sample sizes of distinct RCTs and variations in heterogeneity, attrition rate, compliance, metrics used, and attempts to accomplish weight loss among the trials. 13
Metformin, a widely used medication for type 2 diabetes, also demonstrates significant effects improving insulin sensitivity, metformin helps regulate hormonal imbalances commonly associated with PCOS, such as elevated androgen levels and irregular menstrual cycles. Its ability to lower insulin levels reduces the overproduction of androgens in the ovaries, consequently aiding in the restoration of ovulation and menstrual regularity. Additionally, metformin may contribute to weight loss, which is beneficial for many women with PCOS. While individual responses vary, metformin remains a valuable tool in the comprehensive management of PCOS, offering hope for improved fertility and metabolic health.
Prolactin production is inhibited and gonadotropin secretion is impacted by dopamine produced from the hypothalamus. Reduced dopamine’s inhibitory function may result in aberrant gonadotropin levels, especially luteinizing hormone (LH), which will raise prolactin secretion and cause anovulation. 14 In PCOS patients, cabergoline, a dopamine receptor agonist with a serum half-life of 43 hours and a greater affinity for dopamine D2 receptors, increased uterine perfusion and improved the ovulatory response. 11 Other researchers came to the conclusion that cabergoline administration could help women with PCOS with their irregular menstrual cycles and normalize their androgen levels 15
Although metformin and cabergoline have individual benefits, their combination usage in treating PCOS exacerbated by hyperprolactinemia is yet not well researched. In order to close this knowledge gap, we conducted a systematic review and meta-analysis of clinical trials comparing the effectiveness of this combo medication to metformin alone. This will help clinicians make more informed decisions, enhance patient care, and provide guidance for future clinical research in this field.
Methods
Data sources and search strategy
The Preferred Reporting Items for Systemic Reviews and Meta-Analysis (PRISMA) criteria were adhered to in this systemic review and meta-analysis. From the beginning until 31 May 2024, a thorough search of the PubMed, Web of Sciences, and Scopus literature was done by authors A.K and A.N. There were no language limitations. “((Metformin OR metformin HCl) AND Cabergoline) AND polycystic ovary syndrome OR PCOD OR PCOS OR polycystic ovary disease) AND (hyperprolactinemia)” was the search query, along with its corresponding MeSH terms. To find any relevant studies that might have gone unnoticed, the reference lists of the publications that were retrieved were examined.Additionaly, we performed a snowball search to add studies in our search. All the studies were assessed for eligibility by author M.M.
Study selection
After exporting all of the articles found through the methodical search to Rayyan software, duplicates were eliminated by M.M. After screening the remaining papers based on their abstract and title, the entire texts were carefully examined by N.K to determine their applicability. Three unbiased reviewers carried out the screening (M.M, N.K, P.K). Until a consensus was formed, any disagreements were settled by fourth author (D.K). Only articles that satisfied the following requirements were chosen for inclusion: (i) they had to compare cabergoline and metformin with placebo; (ii) they had to include female patients with hyperprolactinemia and PCOS; and (iii) they had to report the predetermined outcomes of interest. Kappa of +1 indicated perfect agreement between author observations and expectations.
Outcomes measures
This research examines the effectiveness of a combination of metformin and cabergoline versus metformin monotherapy in treating women with hyperprolactinemia-complicated PCOS. The analysis takes into account hormonal outcomes, including levels of prolactin, testosterone, and dehydroepiandrosterone sulfate (DHEAS), as well as the restoration of menstrual regularity and concurrent weight or BMI reduction.
Data extraction and quality assessment
Details on the intervention and control group, such as drug name, dosage, and duration, outcomes (hormonal levels, weight, menstrual irregularity), sample size, demographic characteristics (age, weight, BMI), and follow-up period were all retrieved by the authors (D.K, K.A, C.K.L).
A revised tool for assessing the risk of bias in randomized trials (RoB 2) 16 was used to evaluate the methodological quality of RCTs, while a tool for assessing the risk of bias in non-randomized studies of interventions (ROBINS-I) 17 was used to evaluate non-RCTs. The evaluation domains that make up RoB 2 are as follows 1 : bias resulting from the randomization process 2 ; bias resulting from deviations from the intended intervention 3 ; bias resulting from missing outcome data 4 ; bias resulting from the measurement of the outcome; and 5 bias resulting from the selection of the reported result. Based on the level of bias risk in each category, the assessments are labeled as “low,” “some concerns,” “high,” or, “no information” in situations where there isn’t enough data. In contrast, ROBINS-I is comprised of 7 domains 1 : confounding-related bias 2 ; participant selection-related bias 3 ; intervention classification-related bias 4 ; intervention deviations from the intended interventions 5 ; missing data-related bias 6 ; outcome measurement prejudice; and 7 reported result selection-related bias. Depending on the degree of bias risk, a domain is rated as “low,” “moderate,” “serious,” “critical,” or “no information.” For every included study, the total risk of bias was evaluated using either ROB 2 or ROBINS-I. Out of all the bias domains, the total risk of bias has the least favorable score. Quality assessment was performed by author R.I.
Statistical analysis
RevMan (version 5.3; Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration) was used for all statistical analyses. The total pooled effect measure as well as the effect measures of each individual experiment were displayed using forest plots. Weighted mean difference (WMD) was used for the analysis of weight and BMI due to uniform units of measurement across all included studies, while standard mean difference (SMD) was utilized for the results of hormone levels to account for the diversity in units across the included studies.Furthermore, the effect metric for the incidence of monthly irregularity with a 95% confidence interval (CI) was the odds ratio (OR). Using the previously indicated metrics, forest plots of pertinent results were created, and the random-effects model was used to pool the data. In order to compare the data and generate conclusions, we used at least 2 studies.
Sensitivity analysis was run on each set of data to look at the unique contribution of every study. We used the I² statistic to measure the heterogeneity of effects across trials; an I² value between 25 and 50% was deemed to be mild heterogeneity, and a value between 50 and 75% was deemed to be moderate heterogeneity. The publication bias was examined using a funnel plot. For every analysis, a P-value of less than .05 was deemed statistically significant.
Results
Study identification
Following the initial search of electronic databases, 321 articles were found. Following the removal of 20 duplicate entries, 266 more records were disqualified following an examination of the titles and abstracts. Fifteen out of the thirty-five articles that were left were inaccessible. Out of the twenty that were deemed worthy of a thorough reading, 4 studies—three randomized controlled trials18-20 and 1 case-control study—were selected for meta-analysis. 21 Figure 1 (Supplementary) provides more information on the specifics of study exclusion.
Study characteristics
Table 1 provides a summary of the baseline characteristics of the 4 studies that were chosen for this meta-analysis. Out of the total 535 enrolled individuals, 25 were deemed unfit for inclusion in this analysis due to their noncompliance with the requirement of receiving solely Cabergoline. 20 In 1 trial, 5 participants did not get the allotted interventions. 18
Baseline characteristics.

Abbreviations: cab, cabergoline; met, Metformin; N/A, not applicable; PCOS, polycystic ovarian syndrome; RCT, randomized control trial.
Consequently, 505 people were included in this meta-analysis. Women of reproductive age with PCOS and hyperprolactinemia were the only subjects selected for each research (Table 1) Using statistical techniques, the effectiveness of combination therapy (metformin + cabergoline) versus metformin monotherapy was evaluated based on improvements in the hormonal profile, weight and BMI, and regularity of the menstrual cycle. Table 1 provides an overview of each study’s medication dosage and duration of followup. Since the patient population was small, we performed Hartung-Knapp adjustment, the modified method for random effect meta analysis.
Quality assessment
According to RoB 2, all 3 of the evaluated RCTs had a generally low risk of bias. Ghaneei et al raised certain questions about how results are measured. Regarding bias resulting from deviating from the targeted intervention and bias in outcome measurement, Elsersy et al lacked information. Regarding bias resulting from deviating from the targeted intervention, Hamad et al lacked information. Regarding the non-RCT, the ROBBINS-I technique was used to evaluate 1 study (Matrood et al). The study’s overall risk of bias was minimal. It only exhibited significant bias with regard to missing data and severe bias with regard to measuring outcomes.In conclusion, there were differing levels of bias issues in each area for both RCTs and non-RCTs, but overall, the studies exhibited low bias. Tables 2 and 3 summaries the quality assessment results.
The Quality assessment of RCTs using the RoB2 tool.
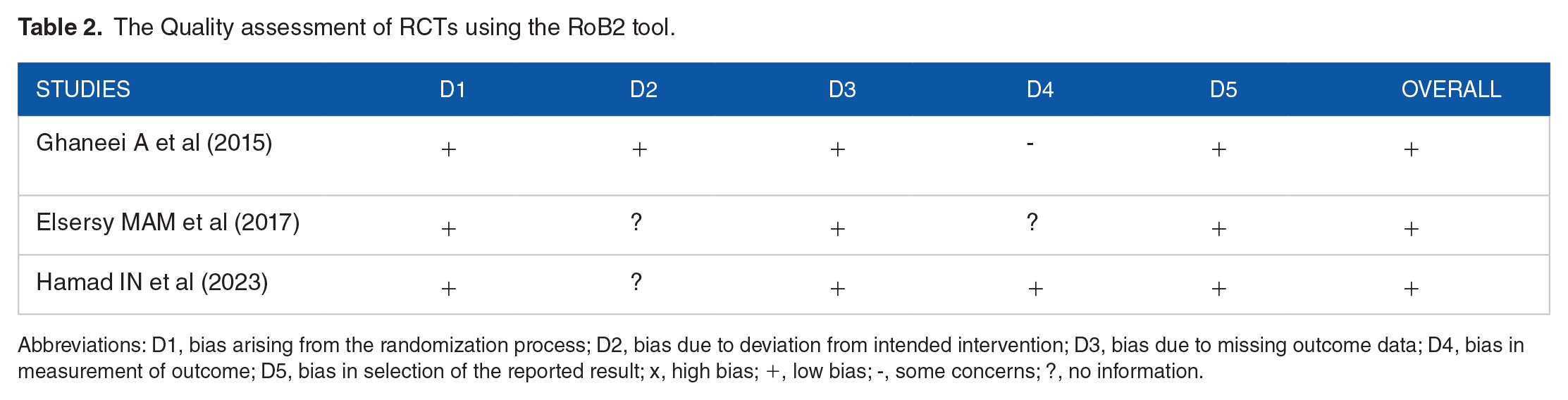
Abbreviations: D1, bias arising from the randomization process; D2, bias due to deviation from intended intervention; D3, bias due to missing outcome data; D4, bias in measurement of outcome; D5, bias in selection of the reported result; x, high bias; +, low bias; -, some concerns; ?, no information.
The quality assessment of non randomized study using the ROBINS-I tool.

D1, bias due to confounding; D2, bias due to selection of participants; D3, bias due to classification of interventions; D4, bias due to deviation from intended outcome; D5, bias due to missing data; D6, bias in measurement of outcomes; D7, bias in selection of the reported results; ×, serious bias; -, moderate bias; +, low bias.
Outcomes
Table 4 displays the results of patients with PCOS who received combined therapy of metformin and cabergoline versus metformin alone.
The table of outcomes.

Abbreviations: BMI, body mass index; CI, confidence interval; OR, odds ratio; SMD, standard mean difference; WMD, weighted mean difference.
P < .05 was considered statistically significant.
Testosterone level
Testosterone levels varied in all 4 investigations. With an SMD = −0.10 (−0.31, 0.11), no statistically significant difference was found between the 2 groups, and there was negligible heterogeneity throughout the investigations (Figure 2 in Supplemental Material).
Prolactin level
In all 4 trials, there was notable variation among the studies, but serum prolactin levels were similar among the groups. With an SMD = −3.23(−4.90, −1.55), the meta-analysis demonstrated that the combination of metformin and cabergoline was more effective in lowering prolactin levels than metformin alone. Matrood et al was found through sensitivity analysis to be a substantial contributor to the observed heterogeneity; however, upon elimination, its significance diminished. Crucially, sensitivity analysis did not affect the meta-analysis results (Figures 3 and 4 in Supplemental Material).
DHEAS level
Three of the 4 studies that made up this analysis18,19,21 assessed DHEAS levels. The 2 groups’ differences in the reduction of DHEAS levels were similar, with an SMD = −0.27 (−0.52, −0.01) (Figure 5 in Supplemental Material).
Body-mass index and weight
About 205 participants had their body weight changes assessed,18,21 while 300 participants had their BMI alterations assessed.19,20 In both groups, there was no statistically significant difference in BMI or weight loss (Figures 6 and 7 in Supplemental Material).
Menstrual regularity
There were reports of 455 participants’ menstrual regularity in response to treatments.18,19,21 Compared to metformin alone, cabergoline therapy along with metformin helped more women achieve regular periods. An OR = 3.07 (2.09, 4.51) indicated that the findings were statistically significant (Figure 8 in Supplemental Material). Every study had identical results (P = .67, I2 = 0%).
Discussion
Our meta-analysis and systematic review of the effects of PCOS with hyperprolactinemia revealed that combination therapy with metformin and cabergoline was superior to metformin monotherapy in terms of reducing prolactin and DHEAS levels and promoting menstrual regularity. However, neither metformin alone nor in combination with cabergoline substantially affected the analyzed participants’ BMI or reduction in body weight. An analysis of Total Testosterone levels between the 2 regimens revealed no discernible differences. These results demonstrate the possibility of cabergoline and metformin together as a useful therapeutic strategy for PCOS patients with hyperprolactinemia, contrasting pioglitazone and metformin combination treatment with metformin monotherapy. 22 In comparison to other test groups, a research trial showed that metformin alone was more effective in lowering testosterone levels in human ovarian theca-like tumor cells (HOTT). 23
Testosterone levels were shown to be lower in all experimental groups in an experiment using albino rats to evaluate the effects of metformin, resveratrol, and their combination on androgen levels. 24 Similarly, metformin was found to have a testosterone-lowering effect in PCOS patients by Wu et al. 25 However, combination therapy was more successful in raising total testosterone levels when compared to metformin monotherapy when a meta-analysis by Zhao et al 26 comparing the effectiveness of oral insulin sensitizers in combination therapy with metformin monotherapy showed that combination therapy was superior to metformin monotherapy in raising total testosterone levels.
Significant heterogeneity in prolactin levels (I2 = 98%) was found in our analysis; this heterogeneity was greatly reduced (I2 = 37%) when Matrood and Abdulhussain 21 was excluded from the sensitivity analysis. This reduction in heterogeneity may have resulted from the study’s small sample size. There might be more exogenous factors influencing the outcome, though, given that the heterogeneity—albeit slight—persisted. The combination of cabergoline and metformin was found to have a more significant effect on lowering prolactin levels than metformin alone. This finding is consistent with cabergoline’s pharmacological function as a dopamine agonist, which has an antagonistic effect on prolactin.27-29 The results of Pala et al, 30 who observed a substantial drop in prolactin levels after cabergoline treatment in their prolactinoma trial, support our findings. Similarly, Papaleo E et al 31 concluded that cabergoline effectively suppresses prolactin levels in PCOS patients. However, the evidence supporting the efficacy of cabergoline in combination with metformin was not sufficient, underscoring the need for further research in this area.
Three of the 4 studies that were analyzed—Ghaneei et al, 18 Elesry, 19 and Matrood and Abdulhussain 21 —examined DHEAS. For both therapy groups, we found negligible variability in our results. While the effect of cabergoline on DHEAS is still poorly understood, Paoletti et al 29 hypothesized that high prolactin levels in PCOS could interact with cabergoline to raise DHEAS levels sufficiently. The results of Moria Yet al 32 on DHEAS, its association with hyperprolactinemia, and its subsequent decline after cabergoline therapy corroborate this claim. In the meantime, DHEAS levels were found to have decreased in a trial comparing the effectiveness of metformin alone against metformin combination with finasteride therapy. 33 To assess the effect of cabergoline plus metformin therapy on this characteristic, more research is required.
Furthermore, despite the fact that metformin alone had a tendency to drop BMI and that the combination showed promise for lowering body weight, neither difference was statistically significant. Interestingly, BMI and weight loss varied slightly to not at all between the selected trials, indicating that the findings were consistent. Metformin may have an impact on weight loss through controlling appetite, which is crucial for PCOS-affected women because weight management is a big problem. Nevertheless, the use of metformin as a stand-alone therapy for weight loss in PCOS patients is not well-supported by research.34-37 Like excess prolactin, which has been shown to increase body weight, cabergoline also efficiently lowers prolactin levels. Despite being primarily used to treat hyperprolactinemia, some research suggests that cabergoline may also help with weight control.38-40
Menstrual cycle regularity is clearly promoted more by combination therapy with metformin and cabergoline than by metformin monotherapy, according to our analysis of menstrual regularity among study participants.Interestingly, this conclusion was consistent with homogenous results across all the studies that were part of the meta-analysis. The results highlight the efficaciousness of the combination of cabergoline and metformin as a treatment strategy to improve menstrual regularity in the intended group. Our results are in line with earlier research that showed how well metformin or cabergoline worked to treat PCOS or hyperprolactinemic amenorrhea-related abnormalities in women’s periods and infertility.9,41-44
More medication combinations, like as metformin plus sitagliptin or inositol, are being researched for the treatment of pcos. One study comparing the effects of metformin and inositol medication found that metformin was a better alternative for enhancing the outcomes of assisted reproductive technologies in women with PCOS. Nevertheless, there was insufficient data to support the benefits of inositol and metformin together. 15 In another work, co-administration of metformin and sitagliptin ameliorated reproductive hormone abnormalities, ovarian polycystic alterations, and insulin resistance in PCOS rats, while also attenuating the induced apoptosis and insulin resistance in PCOS model cells. 45 Nevertheless, since this was an animal study, a human study combining these two approaches is still in the planning stages.
Strengths and Limitations
This review’s extensive search and evaluation of 3 sizable databases are its strongest points. For the treatment of PCOS with hyperprolactinemia, this is the first systematic review and meta-analysis comparing the effectiveness of metformin with cabergoline versus metformin alone.No previous meta-analyses and systematic reviews was performed comparing the efficacy of metformin and cabergoline combination therapy and metformin monotherapy for the management of PCOS with concomitant hyperprolactinemia.
We are aware of our limitations, and the findings need to be interpreted cautiously. Our meta-analysis faced publication bias at the review level, which could skew results by eliminating negative studies, even if individual studies showed low bias risk. Furthermore, our review was limited in its scope and may have missed crucial therapeutic considerations because of time constraints and study methods that prevented us from reporting on all treatment effects in detail. The fact that our study only includes data from the Middle East limits the applicability of our conclusions because the uniformity of the people, medical practices, and healthcare systems in the area could not be representative of diversity around the world. Our study is restricted to short-to-medium-term outcomes due to the lack of long-term follow-up data, which therefore limits the scope of our findings to the time period for which the data are accessible. Our study has not been registered in a registry so this is an additional limitation for our meta analysis.
Conclusion
It is essential to conduct longitudinal studies with thorough long-term follow-up data encompassing all key outcomes of PCOS with hyperprolactinemia in order to adequately address the shortcomings that have been highlighted. Furthermore, broadening the scope of data collection to include a variety of people, geographic areas, and healthcare systems outside of the Middle Eastern countries would improve the findings’ generalizability and breadth.
The management of Polycystic Ovary Syndrome (PCOS) may benefit in the future from the combination therapy of metformin and cabergoline. The capacity of cabergoline to reduce prolactin levels is complemented by metformin’s proven effect in regulating menstrual cycles and enhancing insulin sensitivity, which addresses various elements of PCOS pathology. When combined with other medications, this synergistic strategy may improve ovulation induction and raise the chances of successful reproductive outcomes for PCOS-affected women. Additionally, the combined medication may lessen the negative metabolic consequences that are frequently linked to long-term usage of cabergoline alone. Future developments in the safety and efficacy of this dual treatment method may lead to more individualized and successful PCOS management techniques.
Finally, our meta-analysis and comprehensive review point to the benefits of combination therapy with metformin and cabergoline for enhancing DHEAS, menstrual regularity, and prolactin levels in PCOS patients with hyperprolactinemia. Nevertheless, there was no discernible difference in BMI, body weight, or testosterone levels between metformin by itself or in conjunction with cabergoline. The study has certain limitations, such as publication bias, regional focus, and short-to-medium-term outcome assessment. These underscore the necessity for further research to obtain a comprehensive understanding of the relative efficacy of combination therapy versus monotherapy, in order to improve the generalizability and reliability of these treatment approaches.
Supplemental Material
sj-docx-1-end-10.1177_11795514241280028 – Supplemental material for Efficacy of Metformin-Cabergoline Compared to Metformin Monotherapy for Management of PCOS With Hyperprolactinemia: A Systematic Review and Meta-analysis
Supplemental material, sj-docx-1-end-10.1177_11795514241280028 for Efficacy of Metformin-Cabergoline Compared to Metformin Monotherapy for Management of PCOS With Hyperprolactinemia: A Systematic Review and Meta-analysis by Aakash Kumar, Ahsan Nazim, Mahveer Maheshwari, Nisha Kumari, Purneet Kumar, Chandar Kanta Lohana, Deep Kala, Khansa Ali, Hem Raj, Hamza Islam, Rabia Islam and Monazza Riaz in Clinical Medicine Insights: Endocrinology and Diabetes
Supplemental Material
sj-docx-2-end-10.1177_11795514241280028 – Supplemental material for Efficacy of Metformin-Cabergoline Compared to Metformin Monotherapy for Management of PCOS With Hyperprolactinemia: A Systematic Review and Meta-analysis
Supplemental material, sj-docx-2-end-10.1177_11795514241280028 for Efficacy of Metformin-Cabergoline Compared to Metformin Monotherapy for Management of PCOS With Hyperprolactinemia: A Systematic Review and Meta-analysis by Aakash Kumar, Ahsan Nazim, Mahveer Maheshwari, Nisha Kumari, Purneet Kumar, Chandar Kanta Lohana, Deep Kala, Khansa Ali, Hem Raj, Hamza Islam, Rabia Islam and Monazza Riaz in Clinical Medicine Insights: Endocrinology and Diabetes
Footnotes
Acknowledgements
Authors Acknowledge the assistance of Monazza Riaz in all the tasks throughout the research. They appreciate her enthusiasm to participate extensively and give a boost to research progress. Authors acknowledge the assistance of Hira Riaz in Manuscript writing and in the final review of the paper.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.