
Abstract
Objectives:
(1) Describe the clinical spectrum, imaging features, management, and outcome of brown tumors (BT) of the jaws. (2) Determine via a literature review the facts and controversies around the characteristics and management of this lesion.
Materials and methods:
Our study was approved by the institutional committee of Sahloul University Hospital in accordance with the ethical standards of the Declaration of Helsinki. Sixteen patients with BT in the context of a primary, secondary, and tertiary hyperparathyroidism were treated and followed up during their recovery.
Results:
This study reports 16 patients with a mean age of 48 years old. Brown tumor lesions were associated with primary hyperparathyroidism in 6 cases (38%), secondary hyperparathyroidism to chronic kidney failure in 5 cases (31%), and tertiary hyperparathyroidism in the context of a long lasting CRI in 5 cases. Their location was maxillary in 7 cases, mandibular in 5 cases, and bimaxillary in 4 cases. The treatment consisted of parathyroidectomy in 13 patients, maxillary resection in 3 cases, and vitamin D treatment in 2 cases. Favorable outcomes, characterized by tumor regression, were reported in 9 cases, whereas unfavorable evolution was observed among 7 patients.
Conclusion:
Parathyroidectomy is the gold standard treatment for primary hyperparathyroidism. It resulted in a total regression in all our cases. Regarding secondary hyperparathyroidism, blood screening and chronic renal insufficiency follow-up are critically valuable to detect this condition at an early stage, hence increasing the success rate of brown tumor regression. Our secondary and tertiary hyperparathyroidism results were miscellaneous; although it is important to emphasize the importance of the chronic renal insufficiency management to ensure a success.
Clinical relevance:
Brown tumors should be included in the differential diagnosis of giant cell lesions. Parathyroidectomy is usually sufficient to induce the total regression of the lesion in primary hyperparathyroidism cases. A more delicate approach is needed regarding secondary hyperparathyroidism. Meticulous control of chronic renal insufficiency is mandatory in addition to parathyroidectomy.
Introduction
One of the earliest complete descriptions of a hyperparathyroidism (HPTH) case was reported in 1705 by the French surgeon Courtial. 1 Afterward, it took almost 200 years for the scientific committee to display a description of the condition. It was in 1891 that Von Recklinghausen described for the first time HPTH as a bone condition.1,2
HPTH is an endocrinal disturbance characterized by an overproduction of the parathyroid hormone (PTH), which is responsible in the regulation of calcium and phosphorus. In the most common type of HPTH known as the primary HPTH, high level of PTH will induce hypercalcemia by promoting the release of calcium from bones though an increased osteoclast activity. Consequently, we observe widespread bone resorption.2,3
Depending on the cause of PTH overproduction, BTs can be consequent to 1 of the 4 subtypes of HPTH: primary hyperparathyroidism (PHPTH, caused by a primary disease of the parathyroid glands), secondary hyperparathyroidism (SHPTH, appearing usually in a chronic renal insufficiency context), tertiary hyperparathyroidism (THPTH due to the autonomization of an enlarged parathyroid gland in patients with long-lasting secondary hyperparathyroidism), or quaternary hyperparathyroidism (QHPTH due to an ectopic PTH secretion).2,4
Usually at its last stage, within areas of bone resorption, PHPTH and SHPTH-THPTH cause respectively in 4.5% and 1.5 to 1.7% of the time Brown Tumors; also called osteitis fibrosa cystica.2,5
In addition to a difference in prevalence, BT developed in the setting of SHPTH or THPTH is more severe and difficult to manage compared to a PHPTH context. Indeed, in PHPTH, the endocrinal gland being the source of the disturbance, when treated it induces the regulation of the PTH level and the healing of the lesion. However, in SHPTH the disturbance of the gland is a consequence of primary pathology (frequently a chronic renal failure) that has cause a hypocalcemia. It is in fact in response to this low level of calcium that the parathyroid produce high level of PTH as an attempt to regulate calcium level. Hence the treatment requires a delicate management of the primary pathology which response is not always predictable, especially in long-lasting ones. It is in such context that we observe a THPTH during which the parathyroid glands were stimulated for a too long period which provoke their autonomization.3,11,12
BTs are rare non-neoplastic focal osseous lesions marked by bone cortex thinning and substitution of bone marrow with fibrous tissues. 2 Commonly, BTs touch long bones such as the ribs, clavicle, and femur,3,6 although in 4.5% of the cases bones of the face such as the maxilla and mandible are affected. 4 They appear either as a single located lesion or as multiple ones, disseminating into several bone sites. 3
Specifically in the maxilla, BTs usually arise as exophytic, slowly enlarging brown masses, varying from totally asymptomatic to painful lesions.2,3 Their brown clinical aspect is characterized by large areas of hypervascularity with hemorrhage and hemosiderin deposits, as well as being responsible for BT’s appellation.2,5 The diagnosis of BTs is challenging since they can be radiologically confused with several conditions that develop multiple osseous lesions or with malignancy. Besides, BTs are histologically indistinguishable from central giant cell granuloma (CGCG), peripheral giant cell granuloma, aneurysmal bone, cyst, and the initial stage of cherubism. 3 , 7 Thus, an accurate diagnosis is mandatory to ensure appropriate treatment and stabilize the PTH level. The latter is established when pathology reveals a giant cell tumor and blood screening reports an HTPH.3,5
Therefore, we will describe herein 16 cases presenting primary or secondary hyperparathyroidism accompanied with maxillary and/or mandibular lesions. Their characteristics, diagnosis, and therapeutic approach will be discussed and compared with the literature.
Patients and methods
Our study was approved by the institutional committee of Sahloul University Hospital in accordance with the ethical standards of the Declaration of Helsinki. 8
We conducted a single-site, retrospective study over 19 years from January 2003 to February 2022. Our study lasted 14 months in total, from January 2022 to February 2023. Cases were sorted from the database of the maxillofacial surgery and dental medicine departments of Sahloul Hospital where patients used to be followed.
The inclusion criteria were:
patients presenting with a unique or multiple maxillary lesion(s) histologically diagnosed as “giant cell tumor(s)” or as “central giant cell granuloma” (displaying the characteristic aspect of a dense fibrous stroma with fibroblast, mononuclear cells with a possible monocytic nature, focal areas of osteoid tissue, cystic degeneration, hemorrhage macrophage with osteoclasts as giant multinucleated cells)2,9,10; and simultaneously
patients whose biological tests (mainly PTH and calcium blood levels) reported hyperparathyroidism.11,12
We did not include patients whose medical file was lost or patients with incomplete medical records that could jeopardize the diagnosis.
For each participant, the following information was collected from their standard hospitalization documentation and medical records:
Patient’s descriptive status: origin, age, gender, complaint during their first consultation, medical history;
Clinical data: circumstances of BT detection, date of the first symptoms, date of the first consultation, extraoral and intraoral examination;
Radiological examination of the lesion including panoramic radiography (for 14 patients), paranasal sinuses radiograph (for 2 patients), and computed tomography scan (CT scan) of the facial area (for 12 patients);
Parathyroid gland examination consisting of cervical echography (for 14 patients), parathyroid scintigraphy (for 12 patients), and computed tomography (CT) (asked as a second-line examination for 5 patients);
Extension assessment through CT of the facial mass, standard radiographs of the hand and foot, and Ti-99 bone scintigraphy;
Biological screening: PTH dosage and calcium level (for every patient), phosphorus concentration (13 patients), alkaline phosphatase level (5 patients), renal function through creatinine level (14 patients), and vitamin D dosage (2 patient);
Therapeutic management: etiological treatment (cervical surgery along with medical treatment) and/or a maxillary surgery;
Pathology examinations of the maxillary and parathyroid tumors;
Evolution: clinical, radiological, biological, and therapeutic.
A data collection sheet was used to gather and study the different variables.
Statistical analysis
Excel Microsoft 365 was used to measure the ranges and means of our values.
Results
Baseline characteristics of patients
The main epidemiological features of the selected patients with BT are summarized in Table 3. We reviewed the archives of the maxilla facial department and dental department of the 19 previous years (from 2003 to 2022). The population of 16 patients was 9 women (56%) and 7 men (44%).The ratio of female/male of our population was approximately 1, and the mean age was 48 years old (range 21-80 years old).
The appearance of a swelling accompanied by discomfort was the major complaint that prompted 15 patients to consult. Only 1 patient was consulted for the recurrence of his secondary hyperparathyroidism.
Etiopathogenesis
Etiopathogenesis of brown tumors is summarized in Table 1.
Distribution of the medical disorders behind HPTH types present in the studied population (n = 16).

All patients suffering from PHPTH presented disturbance of their parathyroid glands that was responsible for the HPTH.
Regarding SHPTH patients, 2 patients out of 5 were first diagnosed with HPTH through their BT before their exploration revealed a chronic renal insufficiency (CRI). In these 2 cases, BT led to the renal function test that concluded a CRI diagnosis.
The 3 remained SHPTH cases as well as all THPTH cases (5 patients) were already diagnosed with chronic renal insufficiency (CRI) by the time their HPTH diagnosis was confirmed (and 5 THPTH and 1 SHPTH patients were already treated with hemodialysis).
Clinical features
On the extraoral examination, deforming swelling of the face was the main symptom, except for a single patient with a palatal location. The covering skin was normal and mostly non-painful (81%). No mouth opening limitation was noted, although a labial-chin hypoesthesia was retained in 1 case presenting primary hyperparathyroidism with a bimaxillary vestibular swelling.
Intraoral examination revealed maxillary (7 cases = 44%), mandibular (5 cases = 31%), and bimaxillary (4 cases = 25%) sites to BTs. Premolar and molar sectors were the most involved (14 patients) while the anterior sector was only affected in 2 cases. A higher tendency to extend toward the vestibular region than the lingual region was observed (14 patients against 8 patients).
Dental examination revealed: displacement with multiple diastemas (4 cases), occlusion disorders (1 case), dental mobility (6 cases), dental loss (2 cases), edentulous patients (2 cases), and 5 patients were free of any dental complaints.
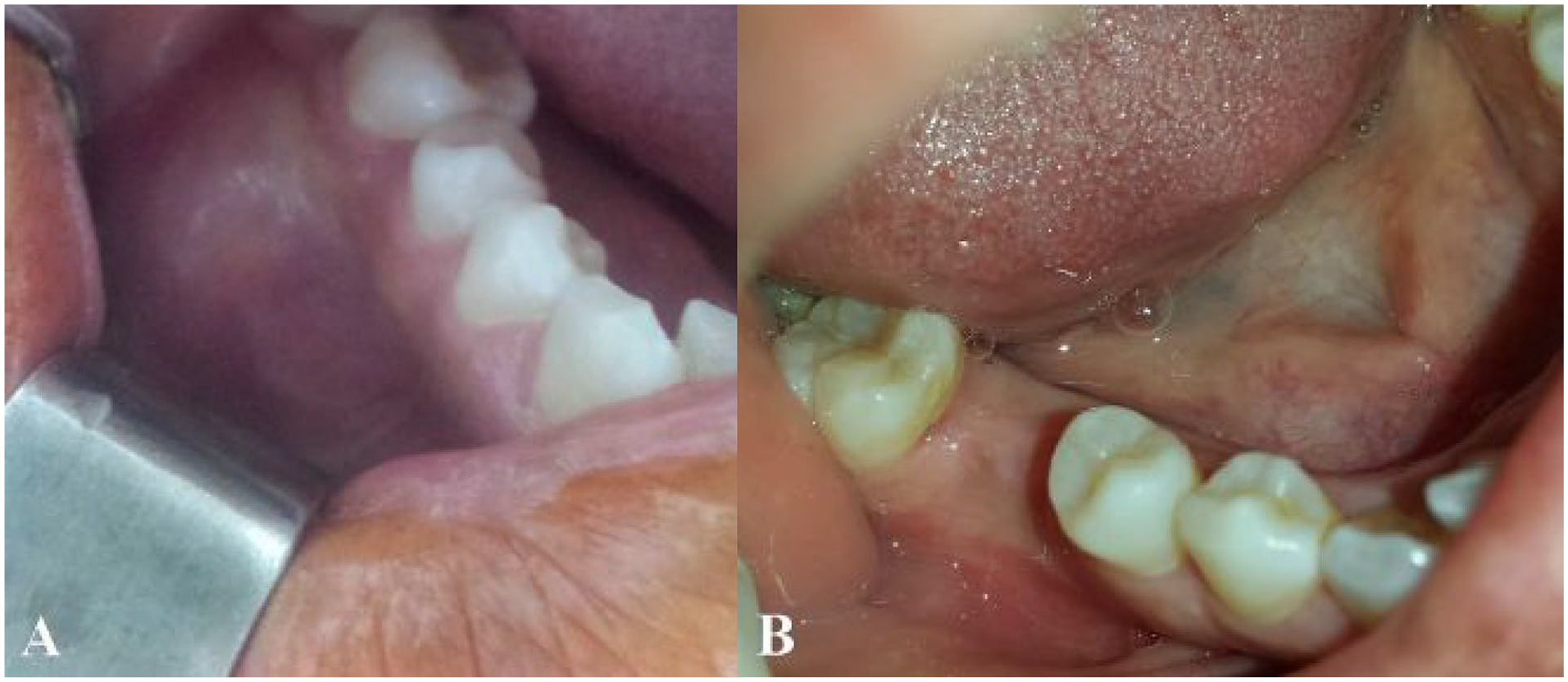
Concretely, the lesion was mostly an asymptomatic tumefaction (for 13 patients), presenting a maximal diameter ranging from 2 to 8 cm (mainly of 5 cm) with a firm consistency to palpation. The overlying mucosa was either normal (for 6 patients) (Figure 1), purplish (for 4 patients), or ulcerated with bleeding to the contact (for 6 patients) (Figure 2).

Intraoral view of a mandible swelling initially (a) and after etiological treamtent (b) showing a total regression of the lesion.

Extraoral profile view (a) and intraoral view (b) of a symphyseal swelling covered by ulcerated mucosa before treatment. Extraoral profile view (c) and intraoral view (d) 3 months following the etiological treatment showing a total regression (Case Nº 4).
Axial view of a mandibular CT scan in parenchymal window showing a substantial, well limited and homogeneous osteolytic lesion of the symphysis, presenting a tissue density and swelling the cortical area.
Radiological features of the brown tumor lesions
Radiological results are summarized in Table 2. On one hand, in the maxilla, most of the images were multiple (73%) and osteolytic (82%). On the other hand, in the mandible, almost the same proportion of multiple images and unique images (56% against 44%) were reported, as well as osteolytic and mixed images. Swelling in the cortical area was noted in every case, with a localized rupture among 5 maxillary locations and 1 mandibular location.
Radiological features of brown tumor images observed among the population studied (n = 16).


Axial view of a CT scan showing a frosted glass image in the mandible.

Parenchymal window of a facial mass’s CT scan in a frontal (a) and axial (b) views showing the multilocular aspect of a mandibular lesion.

Extraoral view showing the widest lesion of our study (8 cm diameter) presenting a bilateral maxillary location.
After the injection of contrast materials, a strong enhancement in the tone of the tumors was observed.
Parathyroid gland examination
The radiological examination of the parathyroid revealed parathyroid nodules (8 cases), hyperplasia (4 case), fixation sites that were either unique (8 cases) or multiple (4 cases), and hyperdense nodules found either under (3 cases) or behind (2 cases) the thyroid gland.
Extension assessment
The local and regional extension were positively diagnosed among 8 patients reaching the homolateral maxillary sinus (4 cases), the nasal fossa (3 cases), and the infra-temporal fossa (1 case).
Regarding hand and foot examination, distant lesions on metacarpals and phalanges (3 cases) were observed in addition to femur site (1 case).
Ti-99 bone scintigraphy revealed other distant locations among 6 patients (eg, in the sacroiliac bone, the skull).
Biology examination
Biology examination for each patient is outlined in Table 3.
Characteristics of the studied population, treatments, and outcomes.

Abbreviations: ♀, Female; ♂, Male; Ø, absence; =, equal to; ↗, increased compared to normal value; ↗↗, increased remarkably compared to normal value; ↘, decreased compared to normal value; PTH, parathyroid hormone blood level in pg/mL; Ca, Calcium blood concentration in mmoL/L; Ph, phosphorus concentration in mmoL/L; PAL, Alkaline phosphatase blood level in UI/L; Vit D, 25-hydroxyvitamin D in ng/mL.
PTH value was high in every patient, with the lowest value being 81.5 (pg/mL) (showed by the 15th case whose HPTH was masked by a vitamin D deficiency). When PHPTH was related to a parathyroid adenoma, each case showed a hypercalcemia. Although for the 2 PHPTH cases that presented a vit D deficiency, their calcium level was normal. However, after vit D supplementation and the regulation of their vit D level, a hypercalcemia was observed for both patients.
Two SHPTH patients out of 5 presented a calcium value close to the inferior limit and 2 patients had a hypocalcemia.
Regarding THPTH cases, they were all suffering from a long lasting CRI. Therefore, they either presented a normal calcium level that tended to increase toward a hypercalcemia or a hypercalcemia.
Biopsy examination
Incisional biopsy was performed on 12 patients because of a brown tumor suspicion (11 patients) and as we were confronted with the eventuality of malignancy (1 patient).
The 4 remaining patients received either an excisional biopsy (case Nº 15) or a biopsy on the excised lump (case Nº 10;11;13).
Histology examination
Pathology examination of the removed sample or entire lump reported the aspect of giant cell lesions. A widely vascularized fibroblastic tissue with giant osteoclast-like cells distributed around the hemorrhagic foci was observed. Hemosiderin deposition was observed in only 9 samples. No signs of malignancy were noted. The diagnosis of a central giant cell granuloma (CGCG) was rendered in 11 cases, and 5 cases were displayed as giant cell tumors (GCT). Among them, case Nº 11 presented two histological diagnoses: the initial lesion was displayed as CGCG, although following the treatment that consisted of a conservative cervicotomy, a second lesion appeared, diagnosed as GCT.
Pathology examination of the parathyroid excision samples rendered with certitude the diagnosis of an HPTH for 13 patients. The histological appearance was in favor of an adenoma in 9 cases and of hyperplasia in 4 cases.
Treatment
Cervical surgery was performed on 14 patients, including a single parathyroidectomy (paraX) in 11 cases and multiple paraX (iterative cervicotomy) in 3 cases.
Regarding SHPTH cases, regulation of the frequency of hemodialysis for the 6 patients already under treatment was set, and hemodialysis was indicated for the 3 remaining patients (1 patient was lost to follow-up).
Medical treatment was prescribed for 9 patients and was based on:
✓ a hypocalcemic agent (calcitonin) in 2 cases of hypercalcemia;
✓ vitamin D supplementation in 2 cases (of PHPTH masked by a vitamin D deficiency);
✓ calcium in 2 cases (one of which was prescribed as part of a vitamin-calcium treatment); and
✓ rehydration with saline serum in 2 hypercalcemia cases.
A maxillary surgery as the initial treatment in order to excise the tumor was performed on 4 patients in total.
Three of them were in response to their personal request, as the lesion was a source of food discomfort, anesthetic and in the wait of the delayed parathyroid scintigraphy (after the biology results were rendered). The fourth patient received an excision-biopsy because of the small size (2 cm) of the lesion (case Nº 15).
Outcomes
The outcome was favorable for 11 patients after an average period of 8 months (Table 3): 5 patients presented a total regression of the lesion post treatment (Figures 1 and 2), 2 patients presented a partial regression of the tumor, and 4 patients presented no recurrence after the excision of their lesion. Signs of radiological re-ossification and normalization of PTH values were noted.
It is important to note that 3 of these patients had to receive an iterative treatment before showing a real improvement (patients Nº 1, 11, and 8).
After treatment, clinically and biologically, unfavorable outcomes were only reported among SHPTH and THPTH patients:
Clinically: an absence of tumor regression was noted among 3 patients after an average period of 3 months before they were lost to follow-up.
Biologically: 1 patient (whose CRI got worse presented an ascension of his PTH that stayed high even after the iterative treatment, 1 patient had an increase of his PTH although it showed a decrease after the second treatment. Finally, 5 patients’ PTH level decreased, although it stayed above normal value. Calcium levels were found to be normal in half of the population and under normal value in the other half. Regarding phosphorus, it was measured for 6 patients and found to be normal for each one.
Unfortunately, 4 patients (Nº 2, 12, 13, 14) were lost to follow-up before we could respond to their outcomes. In average their period of follow-up was 2.25 months.
Discussion
With the minor prevalence of 0.1%, BTs remain lesions in favor of deeper examination and understanding. 13 They actually appear in 3 to 4% of primary HPTH and in 1.5% of secondary HPTH cases, 7 usually indicating the final stage of the endocrinal condition. 14
To this day, 4 types of HPTH have been identified:
Primary HPTH is caused by a primary disease of the parathyroid glands such as parathyroid adenoma (80%), gland hyperplasia (15-20%) or rarely carcinoma (less than 0.5%).2 -4 In this context, brown tumors are a consequence of the direct effect of PTH overproduction on bones. This leads to the transformation of potentially osteogenic cells from osteoblasts to osteoclasts. When bone resorption surpasses new osseous tissue formation, we find the development of osteoid within a vascular fibroblastic tissue unable to elaborate bony trabecula. At that point, vascularity, hemorrhage, and deposits of hemosiderin give the lesion its characteristic brown color. 15
Secondary HPTH occurs in the setting of a chronic renal insufficiency in which low serum levels of calcium, vitamin D, calcitriol, or hyperphosphatemia behave as a stimulant for PTH production;3,6 However, the pathogenesis of BT in the context of CRI remains unclear. 14 They are likely to be a consequence of bone microfractures with subsequent bleeding that cause a localized inflow of osteoclasts, osteolysis, and subsequent reactional medullar fibrosis leading to the formation of BT as a result of hemosiderin deposits. 14
Tertiary type affects patients with long-lasting secondary hyperparathyroidism who have developed autonomous functioning of the parathyroid (with PTH hypersecretion) because of renal insufficiency. 3
Quaternary type is due to an ectopic PTH secretion mostly consequent to a malignant source. 2 This type was not diagnosed among our population.
BT can actually occur in any bone surface with high remodeling activity, such as the ribs or clavicle, but rarely among jaw bones (4.5%), which was the primary location in this study. 7 When jaw bones are affected, BTs arise more frequently in the mandible than in the maxilla.4,7 This survey showed the opposite (44% of our patients had a maxillary location), although for 25% of them, the location was bimaxillary.
Since BTs may be painless (81% of our cases), slow and silent evolution can occur for years. However, they can be locally destructive, and facial deformity, dysphagia, respiratory distress or labial paresthesia are common signs of facial BTs that prompt patients to consult.7,16 In this study, it was precisely the appearing swelling that led 15 patients to consult after an average evolution period of 7 years. This confirms the common silent evolution of the lesion that usually leads to delayed medical management. Our patients were addressed by a dentist in 12 cases or by a nephrologist in 4 hemodialysis cases, emphasizing the key role of dentists in the early detection of systemic conditions through their oral manifestations. 3
On one hand, BTs can be included in a generalized process, with a global decrease in bone density (detected through alkaline phosphatase screening in 19% of our cases), osteoporosis, or suppression of lamina dura (81% of our population). Or, on the other hand, they are included in a localized process. Regarding the latter process, BT are more difficult to diagnose since they appear clinically and radiologically as expansile multilocular masses, guiding the investigation toward the condition responsible for multiple bone injuries such as multiple myeloma, ossifying fibroma, Paget’s disease or metastatic malignancies.15,17 In this study, half of the population presented multiple images (even when clinically it appeared as unique), supporting the multifocal character of BTs. 16 Besides, BT might simulate malignancy by presenting with periosteal reaction or invading soft tissue. 6 This aspect was not reported in this study, as malignant signs were only observed through the invasion of soft tissues in 2 cases, probably because of the wide size of the lesion.
Nevertheless, BTs can easily be mistaken for a neoplasm. Hence, it is important to underline that they actually represent a reparative cellular process and a non-neoplastic lesion despite their “tumor” designation. 15
Pathology examination as well is a source of confusion since BTs exhibit no pathognomonic histologic differences from other giant cell lesions (such as giant cell granuloma (CGCG) or giant cell tumor (GCT)).3,7 For instance, among our cases, pathology rendered the diagnoses of CGCG (in 11 cases) and GCT (in 5 cases). Interestingly, in one of our cases the 2 different diagnoses of CGCG and GCT were displayed for 2 lesions located separately. Therefore, BT as a differential diagnosis should strongly be considered when presented with a CGCG, a GCT, an aneurysmal bone cyst, cherubim or Paget’s disease.7,18
When pathology reports a giant cell lesion, looking for an eventual HPTH through biochemical laboratory tests (measuring PTH, calcium, alkaline phosphatase and vitamin D levels) should be the next step in medical management.3,19 To render this diagnosis, PTH levels must be elevated no matter the HPTH type (which was the case of every patient in this study), although the rest of the test results vary depending on HPTH types. 6
Primary HPTH is characterized by hypercalcemia or rarely by normocalcemia, with low or normal values of phosphorus.3,20 In this study 2 patients out of 6 (33% of the population) had normal levels of calcium. This percentage is higher than the one reported by the literature in which 98% of PHPTH cases reveal hypercalcemia. This is explained by the fact that these 2 patients, showed a deficit of vid D after a 25-hydroxyvitamin D screening which consequently decreased the calcium level into a normal range. Furthermore, kidney function blood tests were executed for these 2 patients and rendered normal serum creatinine and blood urea nitrogen, revealing normal renal function. After a vid D supplementation and the correction of its level, biological tests reported the expected finding of a hypercalcemia. These findings added to the presence of a parathyroid adenoma confirmed the diagnosis of PHPTH masked by a vid D deficiency. In literature, the etiopathology behind the long-term co-existence of elevated levels of PTH and vitamin D deficiency is not yet elucidated. Schematically, it is reported that chronic vitamin D deficiency would lead to an autonomous stimulation of the parathyroid and would cause the serum calcium level to drop into normal values, creating the doubt toward the HPTH diagnosis which was reported in this study.21,22
Secondary HPTH is usually marked by hypocalcemia as in 2 of our cases. Although normal levels of calcium that tend toward the inferior limit can also be reported. In our study, 3 SHPTH patients out of 5 had a normal calcium level close to the inferior limit with the highest values being 2.3 mmoL/L. Therefore, our results are in accordance with the literature. Also for these cases, the absence of a parathyroid adenoma comforted the diagnosis of a SHPTH and not a THPTH. 3 On the other hand, phosphorus level in a CRI context is difficult to analyze as it depends on the nephron capital, hence it might be elevated, normal or more rarely decreased (which provokes the increase of calcium level).3,23,24 In this study, 2 patients presented hyperphosphoremia, 1 patients presented normophosphoremia, and 1 patient presented a merely hypophosphoremia of 1.1 mmoL/L (normal limit being 1.12 mmoL/L) which is in accordance with literature.
Tertiary HPTH is characterized by elevated calcium and alkaline phosphatase level in the context of a long-lasting CRI. 3 This was the case for 2 of our 5 THPTH (cases Nº 6 and Nº 16). However, literature also reports that in front of a long-lasting CRI evolving aside parathyroid abnormality, the diagnosis of THPTH should be rendered even if the calcium level is normal. The reason is that at such a stage the gland is considered autotomized, and calcium level is expected to rise above the normal value of 2.7 mmoL/L.3,18 This was observed in 3 THPTH cases. They presented a parathyroid adenoma or hyperplasia and their calcium level was increasing from an appointment to another. For instance, patient Nº 13’s first calcium test reported the value of 2.5 mmoL/L and the second one 2.57 mmoL/L (Table 3). We can assume that if this patient was not lost to follow up, we would have noted a hypercalcemia after some time. Hence, because these patients were suffering from a long lasting CRI, and had either a parathyroid adenoma or hyperplasia, we could set the diagnosis of THPTH even if the calcium level is still normal.
Once the diagnosis is rendered, treatment becomes indisputable and determining the type of HPTH is mandatory to guide us toward the right approach.3,25
Most authors advocate that the etiological attitude (targeting the endocrine and/or the renal disturbance) should only be an initial treatment, that should eventually be followed by the lesion’s enucleation. However, few authors consider the etiological approach as the unique gold standard for treatment sufficient to provoke the spontaneous regression of the tumor.3,15,26
Regarding primary HPTH, etiological treatment consists of reversing hypercalcemia via parathyroidectomy (paraX), which usually induces the spontaneous sclerosis and regression of the tumor.3,15,27 In our study, paraX was performed on 4 PHPTH patients out of 6. Regarding the 2 remaining patients: 1 patient received calcium and vitamin therapy as he presented a vitamin D deficiency that masked his PHPTH (case Nº 15), and unfortunately 1 patient died from a malignant hypercalcemia (case Nº 3). A total regression of the tumor after a mean period of 12 months (range 2-24 months) was observed except for the patient who died.
Our case Nº 4 is particularly interesting, as despite the advanced age of the patient, her lesion completely regressed after only 3 months’ post-treatment. This can only emphasize the efficacy of this etiological approach toward PHPTH cases. However, despite the fact that spontaneous regression of the lesion usually follows a successful paraX, some authors recommend in addition a tumor resection. They consider the period needed for a total regression to be too long considering the symptoms conditioned by the tumor, which was not observed in our PHPTH patients. Moreover, sometimes lesions fail to regress even after normalization of serum calcium and PTH. 16
Concerning secondary or tertiary HPTH, the approach differs in regard to the first intention of treatment. Few authors recommend controlling renal dysfunction through hemodialysis or kidney transplant first. This should be followed by an evaluation, and if the PHT levels remain abnormal, paraX would be prescribed.3,18
Another approach advocates the correction of the HPTH with paraX or vitamin D administration as the initial step. 7 In our study, all 10 SHPTH and THPTH patients received paraX as a second intention. Among them, 6 patients were already under hemodialysis by the time they consulted fort their BT. The goal was to reinforce and regulate their hemodialysis before the paraX. Regarding the 4 remaining patients, they were prescribed to start hemodialysis, after which they received paraX. Concerning severe CRI cases presenting a THPTH, kidney transplantation was not performed because of the very long waiting list encountered in our country.
It is important to note that after our first treatment plan, none of the lesions increased in size, but only 3 patients presented a regression of their lesion, and it was partial. Although for patient Nº 8, the lesion healed totally after an iterative cervicotomy that was performed because the PTH level of the patient merely decreased.
This could be explained by an insufficient paraX in the first place and a more severe chronic renal insufficiency that is arduous to contain, which prompted us to prescribe an itinerant cervicotomy and lesion resection. Indeed, authors recommend surgical excision of the lesion as an available option if there is no or too slow response to treatment. Besides, some extensive lesions are too large to totally regress and might have a negative impact on facial aesthetic and oral function or provoke respiratory distress.3,7 Therefore, case Nº 1 is a valid example as the patient presented the largest lesion of our cases (8 cm) (Figure 6), located in the maxilla and causing aesthetic concerns. The patient was already under hemodialysis. After paraX, no signs of lesion reduction were noted, and a 6-fold elevation of his PTH was reported, therefore we indicated an iterative cervicotomy and the excision of the tumor that became unbearable for the patient. Fortunately, no recurrence was noted after a follow-up of 9 months.
On the other hand, when applicable the conservative approach should be strongly thought of, without jumping to the surgical approach. Especially for THPTH cases, their renal condition is usually difficult to manage in countries such as ours, where renal transplant requires years of waiting, which might be the reason for the delayed lesion response to our treatment. Indeed, regarding patient Nº 16, we opted for an abstention and monitoring, as the PTH level decreased significantly in only 5 months, and the lesion was in regression. The advanced age of the patient prompted us to opt for this course of treatment. We expect the patient to keep ameliorating in the following months, as he is still followed up in our department.
Medical treatment such as calcitonin, vitamin D, calcium, and so on was administrated to 9 of our patients, in accordance with the literature. We opted for systemic administration since both methods (systemic and intralesional injection) have yielded fine results.3,28 However, some authors advocate the prescription of corticosteroids to reduce the size of wide or multiple lesions. In this study, calcitonin was prescribed instead of corticosteroid, as they both present similar effects. By reducing the size of the lesion, they allow more conservative surgical treatments, thus avoiding the potential morbidity of severe facial resection procedures.3,16
Limitations
Some biochemical values were not ordered for every patient such as the alkaline phosphatase and vitamin D dosage. These values could not be added by our team because of the nature of the study. Not finding the ideal complete explorations is one of the weaknesses of such retrospective studies.
The authors acknowledge the added value the markers’ study could have provided to the study. Although these testes are not routinely executed in Tunisia; and were absent from out study.
None of our CRI patient received a renal transplantation which is the gold standard and could have ameliorate the outcomes of our study. Unfortunately, this surgery requires a very long waiting list in Tunisia which is the reason our patients were under dialysis and not transplanted.
The sample size or power analysis was not performed for this study. The sample size of our population was determined by the cases sorted from the database of the maxilla facial and dental department from 2003 to 2022 presenting the inclusion criteria. The authors are aware that the sample size of our study might limit the drawing of strong conclusions, although because very few studies are reporting this topic, we are convinced that this study could benefit the scientific committee in better understanding brown tumors.
Some patients were lost to follow-up after a relatively short period of 2 months. They were mostly suffering from long-term chronic renal insufficiency, and Sahloul Hospital, being an important medical center, it serves a wide population that usually needs a long commute to arrive to the hospital. Hence, their disabling CRI, added to the commute, could have been the reason for their loss to follow-up, knowing that centers of dialysis are more frequently located in the country and could be closer to their residence compared to Sahloul Hospital.
Conclusion
In conclusion, it is important to note that, since lately calcium screening and blood testing are being more frequently performed, a decrease of BTs due to PHPTH was observed compared to the last decade. This might explain the decrease of BT suspicion in specific clinical and radiological contexts especially in the maxillary location where they are initially very rare. Therefore, reminding dentists and oral surgeons to consider BTs as a differential diagnosis for giant cell lesions and tumors is very judicious, especially when to our knowledge, only 3 retrospective studies were conducted to discuss BTs (mostly in a PHPTH context).16,29,30
The opposite is reported regarding the SHPTH and THPTH context. Because life expectancy of patients suffering from chronic renal insufficiency has increased, more BTs are being diagnosed in this setting.7,31 We expect therefore an increase of maxillary location of BTs, which prompted the elaboration of this study. Besides, elucidating the diagnosis of BTs has a systemic implication as it became in addition a reliable indicator of unregulated chronic renal insufficiency.