
Abstract
Background:
Since bariatric surgery results in massive weight loss, it may be associated with a disproportionate decrease in lean body mass.
Objective:
To evaluate body composition in post-bariatric surgery patients who had a successful weight loss at 12 months (>50% excess weight loss) with comparisons to healthy controls who were matched for age, sex and BMI.
Methods:
This is an observational analytic study using data from post-bariatric surgery patients who had laparoscopic Roux-en-Y gastric bypass (RYGB) or laparoscopic sleeve gastrectomy (SG) at King Chulalongkorn Memorial Hospital. Patients who had percentage excessive weight loss (%EWL) >50% and achieved a BMI of <30 kg/m2 within 12 months after the surgery were included. Non-operative healthy controls matched for sex, age, and BMI (1:1) were recruited. The 12-month post-bariatric surgery BMI was used to match the BMI of the control subjects. A single bioelectrical impedance analysis (BIA) (Inbody 770) machine was used for the entire study.
Results:
Sixty participants were included in this study. There are 30 post-bariatric surgery patients (female n = 19, male n = 11) and 30 non-operative controls (female n = 19, male n = 11). The 12-month post-bariatric surgery patients had lower percentage of body fat (PBF) (30.6% vs 35.9%, P-value .001) and trunk fat mass (10.3 vs 12.4 kg, P-value .04) than non-operative controls. The 12-month post-bariatric surgery patients also were found to have more soft lean mass (SLM) (47.7 vs 39.9 kg, P-value .001), fat free mass (FFM) (51.1 vs 42.3 kg, P-value .001), skeletal muscle mass (SMM) (27.5 vs 23 kg, P-value .003), and trunk lean mass (21.2 vs 19 kg, P-value .02).
Conclusion:
Despite the significant reductions in all body composition variables in post-bariatric surgery patients at 12-month follow-up, both fat free mass and skeletal muscle mass were found to be higher in the surgical patients compared to the control group.
Clinical trials:
Thai Clinical Trials Registry, https://thaiclinicaltrials.org/
ID:TCTR20200223003
Introduction
Obesity is defined as abnormal or excessive fat accumulation that presents a risk to health. Obesity is also associated with the development of type 2 diabetes mellitus, cardiovascular disease, various types of cancer, and other adverse pathological conditions. 1 Bariatric surgery is one of the treatment methods that can achieve long-term weight loss in individuals with severe obesity. 2 The criteria for consideration of bariatric surgery are a body mass index (BMI) of >40 kg/m2 or a BMI of >35 kg/m2 with comorbidities such as hypertension or dyslipidemia. Patients with pre-diabetes or diabetes may qualify with a BMI between 30 and 35 kg/m2. 3 The procedures that are applied in bariatric surgery fall under the general classifications of restrictive and malabsorptive procedures. Maximum weight loss usually occurs within 12 to 24 months following bariatric surgery, 4 and mainly due to an increase in satiety and long-term hypophagia. Possible mechanisms include changes in taste, food preferences, gastric emptying rates, vagal signaling, gastrointestinal hormone activity, circulating bile acids, and gut microbiota.5,6 Lifelong vitamin and mineral replacement therapy are often required to prevent nutritional deficiencies after surgery, especially Roux-en-Y gastric bypass (RYGB) surgery.
In the management of patients who are obese, the aim is to reduce body fat content while preserving the lean component of body mass. 6 Because weight loss following bariatric surgery, particularly Roux-en-Y gastric bypass (RYGB), is much greater than weight loss with nonsurgical methods, it may be associated with a disproportionate decrease in lean body mass (LBM). 7 Research has reported that body composition changed after bariatric surgery with both fat mass and fat free mass decreasing significantly. 8 A previous study showed no significant differences in body composition between sleeve gastrectomy (SG) and RYGB at 1 year after adjusting for differences in initial BMI pre-operatively. 9 We are particularly interested in patients who had a successful weight loss at 1 year after bariatric surgery (>50 %EWL and achieved BMI of <30 kg/m2) whether they would have altered body compositions. Our study aimed to evaluate body composition in post-bariatric surgery patients who had a successful weight loss at 12 months with comparisons to healthy controls who were matched for age, sex, and BMI.
Methods
This is an observational analytic study using data from post-bariatric surgery patients who had laparoscopic Roux-en-Y gastric bypass (RYGB) or laparoscopic sleeve gastrectomy (SG) at King Chulalongkorn Memorial Hospital during the period of January 2015 to December 2019. Patients aged 18 to 65 years who had percentage excessive weight loss (%EWL) >50 and achieved BMI of <30 kg/m2 within 12 months after surgery were included. A total of 795 patients underwent bariatric surgery during the period of January 2015 to December 2019 and 90 patients had successful weight loss at 12 months post-surgery (>50 %EWL and BMI <30 kg/m2). Thirty patients had complete data to be included in the study (Supplemental Figure 1).
Non-operative controls who were healthy (no history of heart/liver/kidney disease, endocrine disorder, cancer, AIDS), had not been participated in any previous weight loss interventions (weight loss program, medications, bariatric surgery), weight stable (no change of >5% of body weight within 3 months) and matched for sex, age, and BMI (1:1) were recruited from health care personals that had annual checkup data available. The 12-month post-bariatric surgery BMI was used to match the BMI of the control subjects. Patients taking medications that can affect body composition were excluded (diuretics, steroid-based, psychotropic, and diabetic medications). Written informed consent was obtained from all participants. We used Glim criteria of The Global Leadership Initiative on Malnutrition 2018 to evaluate malnutrition.
In the post-bariatric surgery group, data on patient history, laboratory investigation, post-bariatric surgery body composition (baseline, 6, and 12 months after surgery) were collected from electronic medical records. In the control group, data on patient history and laboratory investigation were collected from electronic medical records and body composition was measured during the study visit. Questionnaires on dietary intake and physical activity were collected for both groups. A 7-day dietary intake (protein intake and calories intake) at baseline, 6-month, and 12-month post-bariatric surgery were recorded in medical records by nutritionist at time point. Physical activity questionnaires were obtained at the 12-month post-bariatric surgery. Thai version of Short Format International Physical Activity Questionnaires (IPAQ-SF) was used for physical activity evaluation. Single bioelectrical impedance analysis (BIA) (Inbody 770) machine was used for the entire study.
In both groups, body composition variables collected from BIA (at baseline, 6, and 12 months post-bariatric surgery in the bariatric surgical patients) included body weight (kg), height (cm), BMI (kg/m2), waist-hip ratio (WHR), soft lean mass (SLM) (kg) (consist of bones, ligaments, tendons, internal organs, and muscles), fat free mass (FFM) (kg) (all of body components except fat), skeletal muscle mass (SMM) (kg) (the total mass of body skeletal muscle), body fat mass (BFM) (kg), percentage of body fat (PBF) (%), trunk lean mass (kg), trunk fat mass (kg), segmental lean, and fat analysis (fat free mass/fat mass in all body segments [Rt arm, Lt arm, trunk, Rt leg, Lt leg]), fat free mass index (FFMI) (kg/m2) (the amount of muscle mass in relation to height and weight), appendicular lean mass (ALM) (kg) (lean tissue in arms and legs), and appendicular lean mass adjusted for BMI (ALM/BMI).
Statistical Analysis
Demographic data and clinical parameters were described for each group. Continuous variables are expressed as median (interquartile range: IQR). Differences in continuous and categorical variables between post-bariatric surgery and control groups were analyzed using a Wilcoxon rank sum test and Chi-square test, respectively. The Wilcoxon signed rank test were used to compare body composition variables between the baseline and follow-up visit. All P-values reported are two-sided. Statistical significance was defined as P < .05. Stata version 15.1 (Stata Corp., College Station, Texas) was used for analysis.
Results
Sixty participants were included in this study (30 post-bariatric surgery patients, 30 non-operative controls). Table 1 shows baseline characteristics of the entire study population. Nineteen post-bariatric surgery patients were female (63.3%) with a median age of 41 years old. There were no significant differences between sex, age, BMI, total protein intake, smoking, alcohol drinking, and physical activity between the 2 groups. Total daily caloric intake was significantly lower in the post-bariatric surgery group.
Baseline characteristics.

Abbreviations: IPAQ-SF, Short Format International Physical Activity Questionnaire; RYGB, Laparoscopic Roux-en-Y gastric bypass; SG, Laparoscopic sleeve gastrectomy.
Table 2 shows body composition variables of post-bariatric surgery patients at the 12-month follow-up time point compared to non-operative controls. Comparison between the two groups reveal that the 12-month post-bariatric surgery patients had a lower waist-hip ratio (WHR) (0.83 vs 0.9, P-value < .001), lower percentage of body fat (PBF) (30.6 vs 35.9%, P-value .001), less appendicular lean mass (ALM) (9 vs 16.9 kg, P-value < .001), less trunk fat mass (10.3 vs 12.4 kg, P-value .04) and a lower ALM/BMI (0.34 vs 0.63, P-value < .001). Post-bariatric patients also showed higher levels of soft lean mass (SLM) (47.7 vs 39.9 kg, P-value .001), fat free mass (FFM) (51.1 vs 42.3 kg, P-value .001), skeletal muscle mass (SMM) (27.5 vs 23 kg, P-value .003), trunk lean mass (21.2 vs 19 kg, P-value .02), and fat free mass index (FFMI) (19.1 vs 17.3 kg/m2, P-value .001) For Glim criteria of The Global Leadership Initiative on Malnutrition 201810 (requires at least 1 Phenotypic criteria and 1 Etiologic criteria), none of 12-month post bariatric surgery patients had low body mass index or reduced muscle mass following recommended thresholds.
Body composition variables of the 12-month post-bariatric surgery patients and non-operative controls.

Figure 1 shows box plots comparing the median of body composition variables between the 12-month post-bariatric surgery patients and control groups.

Comparisons of the median of body composition variables between the 12-month post-bariatric surgery patients and control groups. (A) Waist-hip ratio (WHR). (B) soft lean mass (SLM). (C) Body fat mass (BFM). (D) Fat free mass (FFM). (E) Skeletal muscle mass (SMM). (F) Percentage of body fat (PBF). (G) Appendicular lean mass (ALM). (H) Trunk lean mass. (I) Trunk fat mass. (J) Fat free mass index (FFMI). (K) ALM/BMI.
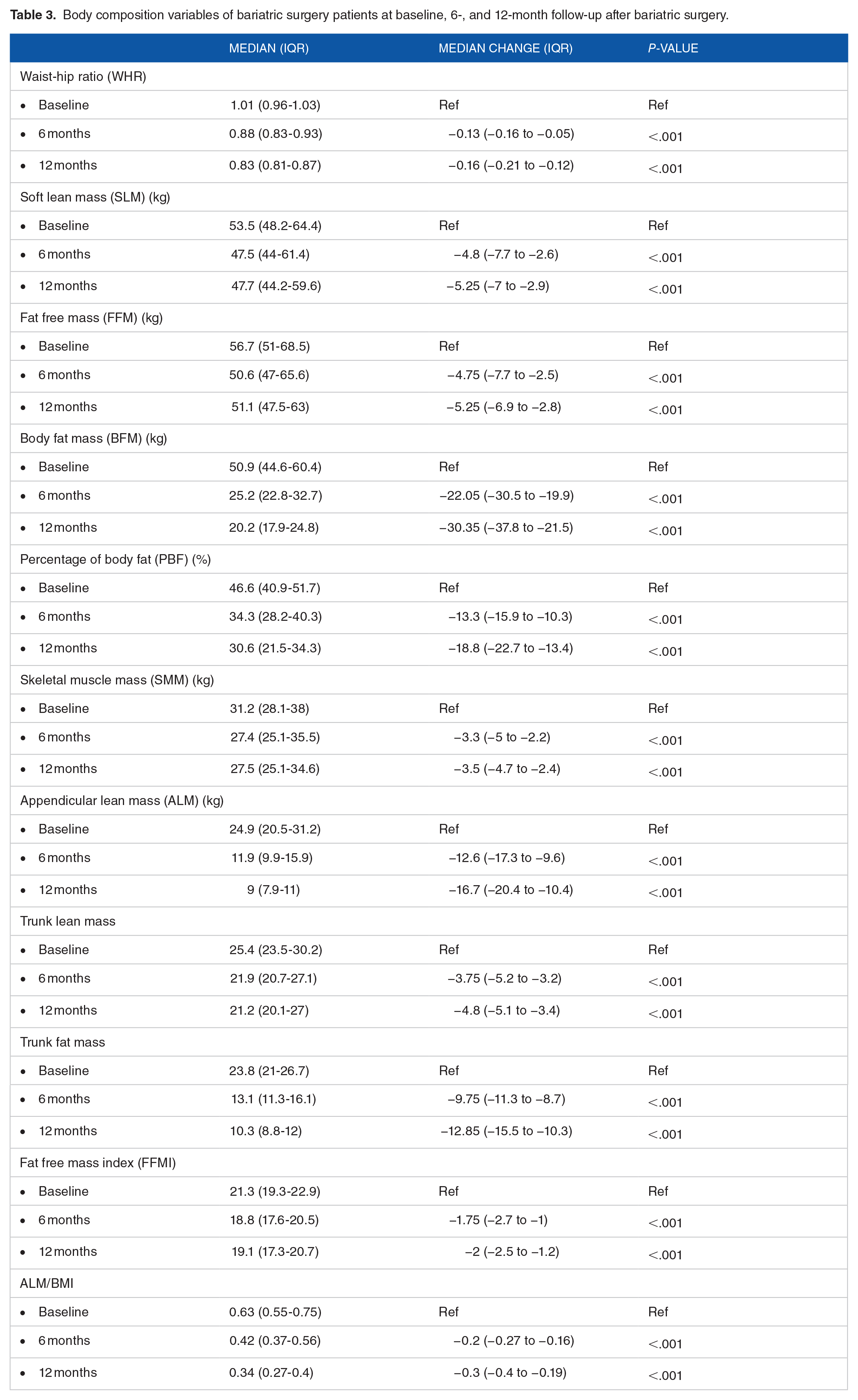
Table 3 shows the changes in body composition variables at 6 and 12 months compared to baseline levels after bariatric surgery in the post-bariatric surgery group. At 6 and 12 month follow-up, there were statistically significant decreased changes in the median levels of all body composition variables including waist-hip ratio (WHR) (−0.13 and −0.16, P-value < .001), soft lean mass (SLM) (−4.8 and −5.25 kg, P-value < .001), fat free mass (FFM) (−4.75 and −5.25 kg, P-value < .001), body fat mass (BFM) (−22.05 and −30.35 kg, P-value < .001), percentage of body fat (PBF) (−13.3 and −18.8%, P-value < .001), skeletal muscle mass (SMM) (−3.3 and −3.5 kg, P-value < .001), appendicular lean mass (ALM) (−12.6 and −16.7 kg, P-value < .001), trunk lean mass (−3.75 and −4.8 kg, P-value < .001), trunk fat mass (−9.75 and −12.85 kg, P-value < .001), fat free mass index (FFMI) (−1.75vs −2 kg/m2, P-value .001) and ALM/BMI (−0.2 vs −0.3, P-value < .001).
Body composition variables of bariatric surgery patients at baseline, 6-, and 12-month follow-up after bariatric surgery.
Discussion
This study showed that the 12-month post-bariatric surgery patients had lower waist-hip ratio (WHR), percentage of body fat (PBF), and trunk fat mass compared to controls. While no significant difference in total protein intake and physical activity between the 2 groups were found, soft lean mass (SLM), fat free mass (FFM), skeletal muscle mass (SMM), and trunk lean mass were statistically higher in the bariatric group. The 12 months post bariatric surgery follow-up revealed a significant reduction in all body composition variables.
This study produced different results compared to previous studies regarding changes in body composition. Although body fat mass, fat free mass and skeletal muscle mass were continuously lost during the 12-month follow-up period, the 12-month post-bariatric surgery patients yet had higher fat free mass and skeletal muscle mass than control groups. In theory, bariatric surgery results in very rapid weight loss from multiple mechanisms including restriction of the stomach area and decreased nutrient absorption which can lead to malnutrition, decreased muscle mass, and sarcopenia. In our study, none of the post-bariatric patients had malnutrition or sarcopenia, as defined by GLIM criteria of The Global Leadership Initiative on Malnutrition 2018. 10
One key factor that may affect changes in body composition is daily protein intake. In the first phase of active weight loss after bariatric surgery, patients should consume at least 60 to 90 g of protein per day or 1.2 to 1.5 g/kg/day 11 to prevent the breakdown of fat free mass, especially muscle mass. In this study, the average daily protein intake in the post-bariatric surgery group was 70 (50-80) g/day or 0.92 (0.41-1.59) g/kg/day and tended to be higher than the control group, although this was not statistically significant difference. It seemed that our patients were able to follow the suggested daily protein intake recommendations. In addition to higher total protein intake, exercise programs after weight loss surgery to develop muscle mass and nutrition counseling at obesity clinics can play an important role for this result.
To our knowledge, this is the first study to evaluate body composition in post-bariatric surgery patients who had a successful weight loss at 12 months (>50% excess weight loss) with comparisons to healthy controls who were matched for age, sex and BMI. In previous reports, controls compared to surgery patients were either healthy normal-weight subjects 12 or weight-reduced subjects after completing medical treatment. 13 Benedetti et al found that fat mass was not statistically different between post biliopancreatic diversion (BPD) subjects and controls (healthy volunteers matched for age, sex, and height). However, post-BPD patients retained significantly more fat free mass (FFM) than controls. 12 Ciangura et al 6 reported no evidence of a decrease in total, trunk, or appendicular LBM in weight-reduced subjects (after RYGB) compared to a nonsurgical control group of similar age and body fat.
The strengths of this study include having a control group that is matched by age, sex and BMI and using multiple parameters to evaluate body composition changes. Our matching of BMI was done using the 12-month post-operative BMI of the surgical patients. And we included only those with successful weight loss after bariatric surgery (achieving BMI of less than 30 kg/m2 and excessive weight loss of >50% at 12 months). Some limitations need to be addressed. We did not match for height and weight in this study as we could only match for BMI. There are some limitations in the use of BIA in obese populations as it is an indirect method to evaluate body compositions. And for evaluation of total protein/total calories intake and physical activity could be affected by a recall bias. Lastly, we have a small number of subjects and power analysis for sample size calculation was not done. Further prospective studies should be conducted for a period greater than 12 months or in postoperative patients with BMI >30 kg/m2 to evaluate long-term changes in body composition after performing bariatric surgery.
Conclusion
Data from this study has provided a better understanding of changes in body composition during weight loss following bariatric surgery in patients who at 12-months post-surgery have achieved a BMI <30 kg/m2 and excessive weight loss of >50%. Despite the significant reductions in all body composition variables in post-bariatric surgery patients at 12-month follow-up, both fat free mass and skeletal muscle mass were found to be higher in the surgical patients compared to the control group.
Supplemental Material
sj-docx-1-end-10.1177_11795514231206731 – Supplemental material for Comparison of Body Composition Variables between Post-Bariatric Surgery Patients and Non-Operative Controls
Supplemental material, sj-docx-1-end-10.1177_11795514231206731 for Comparison of Body Composition Variables between Post-Bariatric Surgery Patients and Non-Operative Controls by Sirinrat Tangjittrong, Suthep Udomsawaengsup and Patchaya Boonchaya-anant in Clinical Medicine Insights: Endocrinology and Diabetes
Footnotes
Acknowledgements
The authors thank all of the obesity clinic staff during the study period, all healthy controls and bariatric surgery patients who participated. The authors also thank Associate Professor Pimjai Anthanont for being part of a project committee, Wasan Punyasang for statistical consultation.
Declarations
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.